
Abstract
Introduction:
Intravesical chemotherapy instillation immediately after tumor resection is a well-known practice in the management of non-muscle invasive bladder cancer. Despite being largely well tolerated in most cases, it is not devoid of severe and life-threatening complications.
Case Presentation:
We present an unusual case of bladder perforation that happened 2 weeks after bladder tumor resection. The patient had received single dose intra-vesical instillation of doxorubicin after TUR-BT. Conservative managements failed to achieve bladder healing; as a result, open surgical repair was performed. To the best of our knowledge, this is the first reported case of bladder perforation after intra-vesical doxorubicin instillation.
Conclusion:
The occurrence of such a rare serious complication in a mostly safe intervention must be taken into consideration. A high index of suspicion, timely management, and proceeding to more invasive surgical treatments when necessary are cornerstones in the management and preserving the bladder.
Keywords
Introduction
Bladder cancer (BC) is the seventh most commonly diagnosed cancer in men worldwide. About 75% of the cases are Non-muscle invasive (NMIBC). 1 Transurethral resection of the bladder tumor (TURBT) remains the gold standard of therapy for diagnosing and treating NMIBC. To decrease the recurrence rate of low-risk tumors, a single, immediate, post-operative intravesical instillation of chemotherapy is recommended. 1
The most commonly used chemotherapeutic agent is Mitomycin C (MMC), which is an alkylating agent that inhibits DNA synthesis and causes single-strand breakage of DNA and chromosomal breaks. 2
Immediate single instillation (SI) is largely well-tolerated. However, severe complications and even death have been reported in the literature. Here we present a case wherein the patient had an extraperitoneal bladder perforation that occurred 2 weeks after TUT-BT and immediate postoperative instillation of doxorubicin.
Case Presentation
A 63-Year-old male, a heavy smoker, with no other co-morbidities, was referred to urology clinic for evaluation and management of a lesion on the left bladder wall that was incidentally detected on a CT scan. He did not have any urinary symptoms on initial presentation.
Cystourethroscopy revealed 2 papillary growths on the left lateral bladder wall, which were resected completely and smoothly by a resectoscope using a monopolar energy. Complete resection of the tumor was achieved without any intra-operative complication or perforation. Hemostasis was secured, and a urethral catheter was inserted.
In accordance of the EAU guidelines, the patient received an intravesical instillation of 50 ml of doxorubicin diluted in 100 cc of saline 6 hours after the TURBT. During the instillation, his vital signs were stable and he had neither hematuria nor abdominal pain. One hour after the instillation, the catheter was unclamped and was attached to continuous bladder irrigation.
Two days after the surgery and in the absence of hematuria, the indwelling catheter was removed, and the patient was discharged home the next day.
When seen in the clinic 1 week later the patient was fine with no alarming symptoms. The pathology report showed a low-grade Ta Papillary urothelial carcinoma. Based on the pathological diagnosis and according to the EAU guidelines, adjuvant chemotherapy instillations were planned.
Two weeks later, the patient presented with, dysuria, frequency, urgency, as well as pelvic and perineal pain. Physical examination was unremarkable. Urine analysis showed numerous WBC’s, RBC’s, and bacteria. An empirical antibiotics course was commenced.
In view of the worsening symptoms and the past history of anal fistula, a contrast enhanced pelvic MRI was performed. It showed a diffusely thickened urinary bladder wall, with evidence of a focal wall defect at its left aspect (the site of the resected tumor). The active urine leak into the perivesical space confirmed the diagnosis of retroperitoneal bladder perforation (Figure 1).
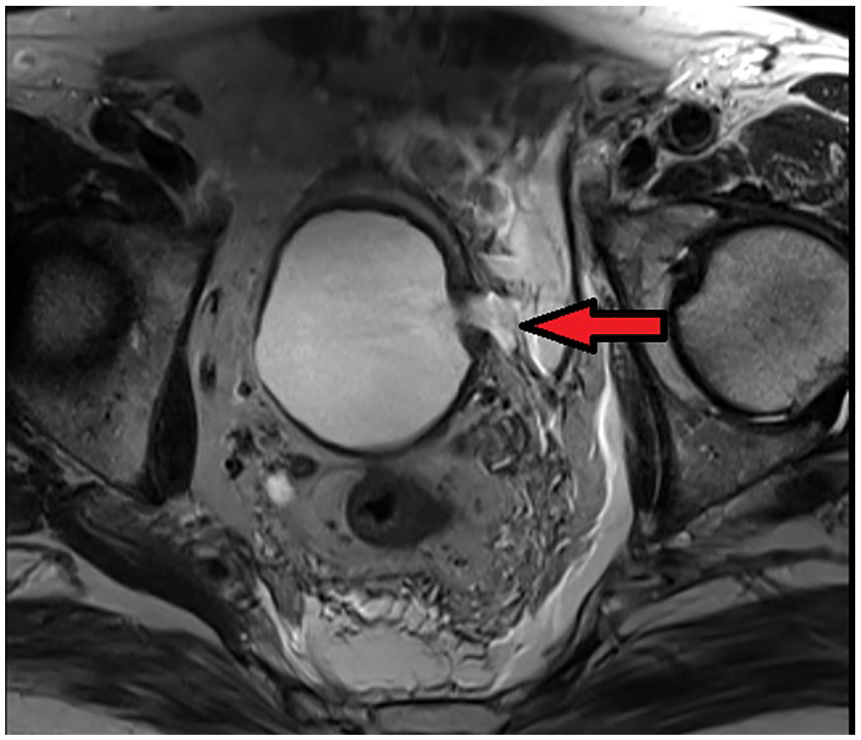
Pelvic MRI (axial view) showing extraperitoneal bladder perforation at the left lateral wall (arrow points to extravasated contrast).
The patient was managed conservatively with antibiotics and an indwelling catheter for 3 weeks.
A follow-up retrograde CT cystogram showed no improvement and a gross contrast leak from the same site was identified. The catheter was kept for 6 more weeks and the CT cystogram was repeated showing the same results with no evidence of improvement. The patient refused to keep the catheter for a longer period so the option of open surgical repair was discussed with him.
Extraperitoneal laparotomy was performed, a perivesical small abscess was drained and cultured, necrotic tissues were debrided, and the bladder wall defect was rimed and closed in 3 layers. Tissue biopsies from the pelvic wall and bladder wall were harvested. A urethral catheter and pelvic drain were kept in place. The postoperative course was uneventful, the drain was removed on the third-day postoperatively, and the patient was discharged home with the urethral catheter in.
Histopathological evaluation of the pelvic wall and the bladder biopsies verified acute and chronic inflammation as well as granulation tissue formation. However, both were negative for malignancy. The urinary bladder biopsy also showed extensive foci of dystrophic calcification while the pelvic wall biopsy revealed fat necrosis (Figures 2 and 3).

The histologic examination revealed fragments of soft tissue with fat necrosis in the lower left area, mixed acute and chronic inflammatory cell infiltrate and hemorrhage in the upper right area (Hematoxylin & Eosin, 200X).

The histologic examination revealed multiple areas of calcifications embedded deep in the tissue with associated crystal-like material suggestive of calcium-oxalate or talc powder crystals (Hematoxylin & Eosin, 200X).
A follow up CT cystogram was done 3 weeks after the bladder repair. Although it showed a considerable regression in the size of the bladder defect, interestingly it also showed persistent extra-peritoneal contrast leak from the bladder along it’s left lateral aspect (Figure 4).

Retrograde Ct cystogram showing persistent contrast leak from the left lateral aspect after surgical repair.
Due to this slow healing, the catheter was kept in. Six weeks later, a follow up CT cystogram showed healing with no extraperitoneal contrast leak (Figure 5). And hence the catheter was removed.

Retrograde Ct cystogram showing a healed bladder wall with no contrast leak.
Two follow up cystoscopies and bladder biopsy (from an erythematous area on the left lateral wall) with 3 months intervals showed good healing of the bladder wall and no recurrence of the tumor.
Discussion
Single intravesical instillation with mitomycin C (MMC), epirubicin, or pirarubicin, have shown a beneficial effect in reducing recurrence rate compared to TURBT alone. However, randomized comparisons of individual drugs have not been conducted. 3
The high recurrence rate of NMIBC may be attributed to the seeding of floating tumor cells. Immediate chemotherapy instillation has been shown to act by destroying these circulating tumor cells after TURBT. Hence the EAU guidelines recommend initiating the instillation within the first few hours after TURBT. 1
Most of the complications of intravesical chemotherapy instillation are minor and can be managed medically. Dysuria and urinary frequency and urgency were the most common complications. 4
On the other hand, reporting major complications such as bladder perforation, perirectal abscesses, eosinophilic cystitis, and ureteral stenosis is limited to case reports.5-14
In this case, we described our experience with bladder perforation after immediate intravesical instillation of doxorubicin.
One can argue that the perforation has occurred intraoperatively and gone unnoticed. However, in view of the absence of endoscopic evidence of perforation, late presentation of symptoms, and the absence of symptoms during and after the instillation we assume that the Single Dose Intravesical Doxorubicin Instillation caused the perforation rather than complicating an existing one.
To explain the mechanism of perforation, Lim et al 7 and Cliff et al 8 hypothesized that perforation is caused when attenuated muscularis propria gets necrosed after MMC instillation.
The presenting complaints of our patient were perineal and pelvic pain as well as urinary irritative symptoms. This is similar to Elmamoun et al 9 cohort in which all the 6 patients presented with perineal and pelvic pain. Other symptoms such as fever, urine retention, and recurrent UTI were variably reported by others. Table 1 summarizes the clinical presentation and management of bladder perforation in the previously published case reports.
A summary of the presentation and management of bladder perforation after immediate chemotheraputic agent intravesical instillation.

Abbreviations: Ep, epirubicin; MMC, mitomycin C.
Concerning the management, almost all the reported cases were initially managed conservatively by urethral catheterization, anticholinergics, and antibiotics. However, this was insufficient to heal the bladder in some cases which needed open repair. Moreover, some ended with cystectomy.
In our case, the patient has an extraperitoneal extravasation that failed the conservative management and needed open surgical repair.
A striking feature of the healing process that was seen in many cases including ours is the poor and slow healing. In our case, the patient needed 9 weeks for complete healing after proper open 3 layers bladder wall repair.7-9,13,14
While Lim et al attributed the slow healing in their case to the patient’s pre-existing peripheral vascular disease and suboptimal tissue oxygenation, no risk factors were identified in the other cases including our patient who was free of any comorbidities. We suppose that the poor healing is linked to the chemotherapeutic agent inflammatory effect rather than to patient factor.
This assumption is backed by the reported characteristic of mitomycin induced skin ulcer in cases of extravasation after intravenous administration. These ulcers are well known for their chronicity and the low tendency of spontaneous healing. Moreover, debridement and soft-tissue reconstruction following extravasation of MMC are recommended for patients with persistent ulceration and pain. 15
Another common finding in the cases that mandate open repair was the presence of perivesical soft tissue necrosis and extensive inflammation. Doherty et al observed that more extensive bladder wall and fat necrosis of extravesical tissue in cystectomy specimens occurred when either epirubicin or mitomycin instillation was administered than in that seen following TURBT alone. 16
This cytotoxic effect was also reported by Tyritzis et al 11 after epirubicin instillation, and by Cliff et al, 8 Nieuwenhuijzen et al, 12 and Hatem and Leifeld 14 after MMC instillation. This cytotoxic effect was recognized herein for the doxorubicin instillation, which is the first time to be reported as a complication of doxorubicin.
It is worth to mention that the perforation had no adverse oncological effect on our patient as no tumor recurrence was detected during follow up.
Conclusion
Immediate intravesical instillations of chemotherapy are not devoid from risk and serious complications as bladder perforation can occur. Whether it’s value in decreasing the recurrence justify the risk of bladder perforation is not our argument in this case report. Nevertheless, this severe complication should be kept in mind, and high index of suspicion will aid in timely management. If perforation is suspected, urethral catheterization and contrasted imaging are mandatory. In the case of failed conservative management surgical repair is warranted even in extraperitoneal leak.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Concept: AA, SAD. Design: MA, SA. Supervision: AA, SAD, MAA. Resources: MA, HM, NB. Materials: AA, MA, NB. Writing manuscript: AA, MA, HM. Critical review: AA, SAD, MAA.
Informed Consent
The patient has given his written informed consent to publish his case including publication of images. The study follows the guidelines for human studies and is conducted in accordance with the World Medical Association Declaration of Helsinki.