
Abstract
Hemoptysis after thoracic endovascular/open aortic repair is relatively rare but a well-known complication, and normally diagnosed with aortobronchial fistula (ABF). Here, we present a patient who suffered from recurrent massive hemoptyses even after multiple thoracic endovascular aortic repairs (TEVARs), where hemoptysis was ultimately controlled by pneumonectomy. In this case, the bleeding source was not the aorta but the lung parenchyma itself, indicating the importance of raising awareness that the cause of massive hemoptysis after TEVAR may not always be an ABF.
Introduction
Aortobronchial fistula (ABF) is a relatively rare but well-known complication after thoracic endovascular aortic repair (TEVAR) or open thoracic aortic surgery, the main symptom being hemoptysis. 1 Once a patient is diagnosed with ABF, additional or primary TEVAR has become the popular choice for therapy in recent years,1,2 especially if there is no sign of infection, but hemoptysis continues in some patients despite successful TEVAR procedures without endoleak. We previously reported a different case of a patient who underwent embolization of the pulmonary artery for recurrent massive hemoptyses after additional TEVAR 3 ; from that experience, we have come to think that the cause of massive hemoptysis after TEVAR may not always be an ABF but diffuse inflammatory changes presumably induced by TEVAR. Here we present another patient who suffered from recurrent massive hemoptyses after multiple TEVARs, where hemoptysis was ultimately controlled by pneumonectomy.
Case Report
A sexagenarian male patient came in with acute aortic dissection type B. The false lumen was thrombosed, but the descending aorta showed rapid aneurysmatic change in the distal aortic arch and in the middle of the descending aorta (Figure 1A), thus the patient underwent 1-debranching TEVAR (cTAG 34 mm × 200 mm for distal + cTAG 45 mm + 20 mm for proximal, Gore medical, Flagstaff, Arizona) with zone 2 landing, extra-anatomical bypass between the left common carotid artery and the left axillary artery (Propaten, 8 mm Gore medical, Arizona, USA), and coil embolization of the left subclavian artery (Figure 1B). Postoperative course was uneventful, but the patient suffered from hemoptysis 5 months after the first TEVAR. The computer tomography (CT) revealed a type Ib endoleak (Figure 1C), and additional TEVAR was done for distal cover and extension (Zenith TX2 42 mm × 162 mm, Cook, Bloomington, Indiana, Figure 1D). Thereafter, the hemoptysis ceased, and the patient was doing well until the following event.

(A) Saccular aneurysms of the descending aorta after subacute aortic dissection type B, (B) successful treatment with TEVAR, (C) type Ib endoleak 5 months after the first TEVAR, (D) CT-finding after additional TEVAR toward distal, (E) CT examination after hemoptysis revealed type II endoleak, and (F) zone 0 TEVAR with chimney method in the brachiocephalic trunk. CT indicates computer tomography; TEVAR, thoracic endovascular aortic repair.
Three years after the second TEVAR, the patient suffered from another massive hemoptysis. Immediate CT showed enlargement of the aneurysm with suspected type II endoleak (Figure 1E), but no extravasation into the bronchial system or lung parenchyma were observed. During this event, the hemoptysis was so massive that the patient went into cardiopulmonary arrest due to hypoxia, and a veno-arterial extracorporeal membrane oxygenation (ECMO) device was applied. Under veno-arterial ECMO, the general condition of the patient stabilized and could be weaned off the ECMO device on the third day. Immediately thereafter, to eliminate the possibility of ABF due to type Ia endoleak, a third TEVAR was performed (Figure 1F). The procedure extended the proximal length with zone 0 landing (cTAG 45 mm × 2000 mm, Gore medical), and included an extra-anatomical bypass between the right and left axillary artery (Propaten, 8 mm, Gore medical) and chimney stenting into the brachiocephalic trunk (Excluder leg 20 mm × 1000 mm, Gore medical). Subsequent CT showed no endoleak and no aortobronchial fistulation, but massive hemoptysis recurred the following day, and veno-venous ECMO was necessary to maintain sufficient oxygenation. Bronchoscope revealed continuous bleeding from the left main bronchus.
As a final solution to control the bleeding from the left lung, we decided on a left upper lobectomy. A left thoracotomy in the fifth intercostal space was performed. The entire left lung was severely adhered to the chest wall and aorta, and severe inflammatory change was seen in both the upper and lower lobes. Because it was uncertain whether the upper lobe adjacent to the aortic arch was the sole source of the lung bleeding, and intraoperative findings indicated rather the whole left lung to be affected than a localized lesion, we ultimately finished with a pneumonectomy (Figure 2A). The pathological examination revealed no ABFs; there was very severe diffuse inflammatory change in the upper lobe and severe inflammatory change in the lower lobe (Figure 2B) as well. After the pneumonectomy, no lung bleeding occurred and the patient could be weaned off the veno-venous ECMO 5 days after the operation, and extubated on the 20th postoperative day. The patient had done well for 4 months, but after suffering from left pyothorax, died of this pyothorax 5 months after the pneumonectomy.
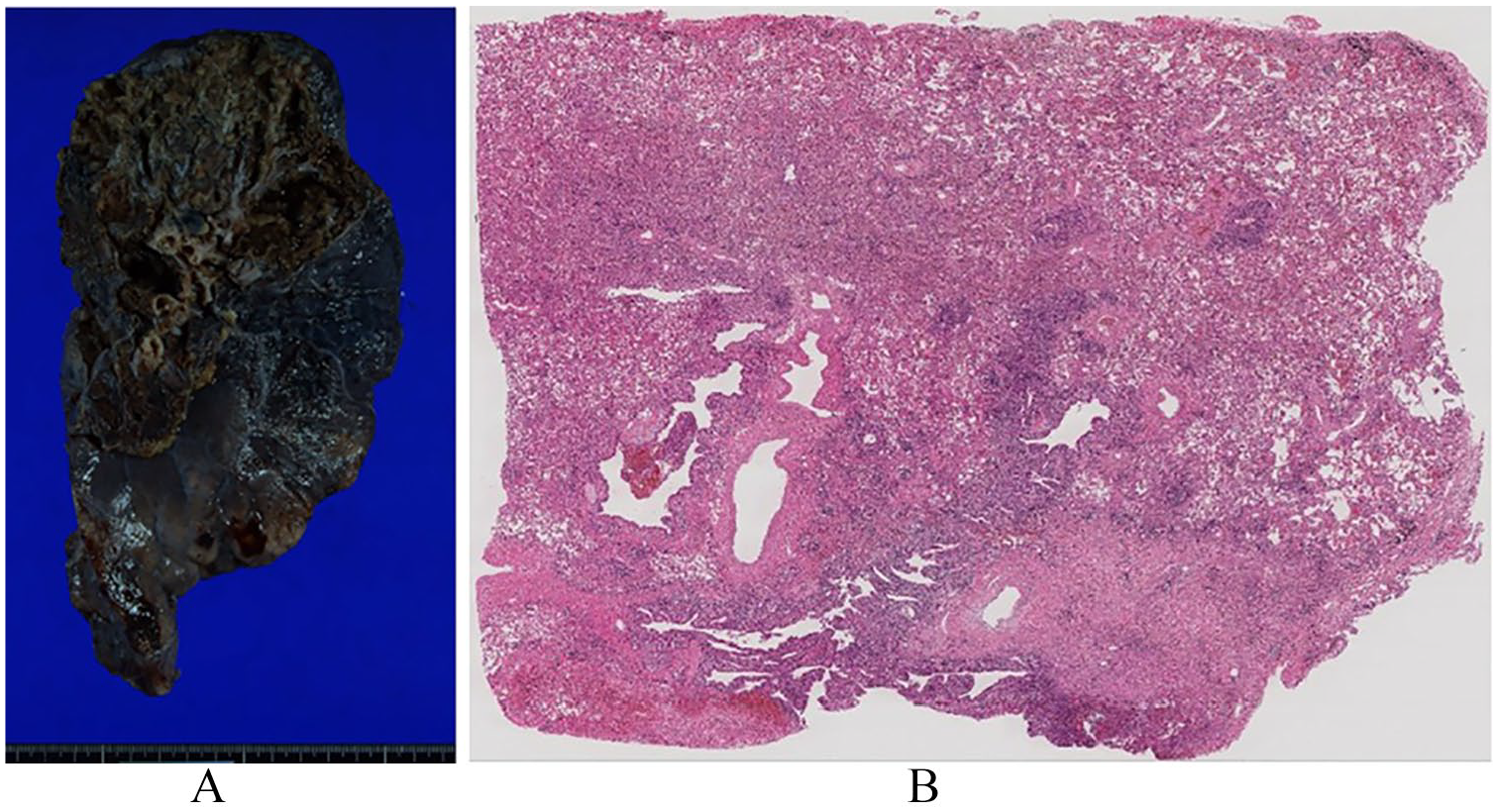
(A) Macroscopic finding of the left lung. No aortobronchial fistula was observed and (B) hematoxylin and eosin staining of the left lung. Massive inflammation with bleeding in the parenchyma was observed.
Written informed consent for publication of this case was obtained from the wife of this patient.
Discussion
Massive hemoptysis after TEVAR is normally diagnosed with ABF, but in this particular case, the bleeding was from the lung parenchyma, not the aorta. This experience suggests that in certain patients, massive hemoptysis after TEVAR that cannot be effectively treated by additional TEVARs should be considered for open aortic repair or lung resection, to control inflammatory change in the lung parenchyma adjacent to the diseased aorta. Furthermore, open aortic repair using the frozen elephant trunk technique may not be suitable for this pathology, because the diseased aorta would remain.
Where does bleeding come from in patients who underwent TEVAR? From our previous study 3 and the present experiences, we think there may be mixed pathologies cases that are commonly construed as ABF. Canaud et al 4 described postulated causes of ABF after TEVAR such as, stent graft coverage of the bronchial arteries leading to ischemic necrosis of the bronchial wall, chronic endoleaks leading to erosion into the adjacent lung, and penetration of the stent graft through the aortic wall into the lung. Although “erosion into the adjacent lung” is understandable, penetration of the stent graft through the aortic wall into the lung may be farfetched. In fact, Czerny et al summarized 26 patients with ABF from the European registry of endovascular aortic repair complications between 2001 and 2012 with a total caseload of 4680 TEVAR procedures in 14 centers, 5 and they reported that the ABF was directly visualized in no patient and endoleak was found in only 9 patients (35%). 5 Inflammatory lung diseases can cause massive hemoptysis. 6 We speculate that out of the patients who suffer from hemoptysis after TEVAR, in some, the main pathology is not ABF but inflammatory change of the adjacent lung resulting in bleeding into the bronchial system, as the present case. To detect such inflammatory changes of the lung caused by TEVAR, positron emission tomography–computed tomography (PET-CT) may be a reasonable diagnostic option, 7 but it may not be able to distinguish the inflammation of the lung parenchyma adjacent to the diseased aorta treated by TEVAR from mycotic aortic aneurysm. Further studies for detecting this cause are required.
Nevertheless, TEVAR is an attractive choice of therapy for patients having diseased aorta and suffering from hemoptysis. We agree with Anastasiadou et al 8 in that TEVAR should be the first therapy for all patients for hemodynamic stabilization, and could be the definite therapy in cases where an infectious factor is absent. However, our previous case 3 and the present case suggest that when additional TEVAR does not sufficiently treat post TEVAR hemoptysis, it is possible that ABF is not the main pathology; further endovascular repair would have no effect because the bleeding source is not the aorta but the adjacent lung parenchyma. In such cases, one should consider open aortic repair with resection of the diseased aorta and/or lung resection adjacent to the diseased aorta.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
NI and HK wrote the manuscript, SN and NW prepared the figures and AH corrected English.