
Abstract
Small-cell carcinoma of the uterine cervix is a rare and aggressive tumor, and the prognosis is poor compared with those of squamous cell carcinoma and adenocarcinoma of the uterine cervix, even when discovered at an earlier stage. We treated a patient with progressive small-cell carcinoma of the uterine cervix that metastasized to the cervical spine. The patient, a 73-year-old woman, presented with the symptom of numbness in her limbs. As she had difficulty moving her limbs (ie, quadriplegia), she was carried to an emergency room. A metastatic cervical spine tumor from the uterine cervical cancer was revealed by a computed tomography scan, and the patient was then transferred to our hospital’s neurosurgery department for treatment. We performed a resection of the cervical spine tumor and fixation of the spinal bone. Because the patient’s performance status was 4 and she remained bedridden 24 h/day, we could not perform systemic chemotherapy. We thus provided palliative care, including palliative radiotherapy, pain control, and rehabilitation to improve her limbs’ functioning. The patient died of the uterine cancer within approx. 6 months after the initiation of treatment. There is no established treatment for small-cell carcinoma as a gynecological lesion. For patients with progressive uterine cancer, the optimal treatments, including palliative care, must be determined.
Introduction
Small-cell carcinoma, also called neuroendocrine tumor (NET), is a rare tumor that arises from various organs such as the intestine and lung. 1 The NETs are classified based on their pathological features, and small-cell carcinoma is classified as a neuroendocrine carcinoma (NEC), the features of which include low differentiation and high proliferation. 2 As small-cell carcinoma is aggressive and easily recurs after various treatments, the prognosis of progressive small-cell carcinoma is poor.
The incidence of bone metastasis of uterine cervical cancer is generally low, and in all cervical cancers, this incidence is only a few percent. 3 The mechanism of the bone metastasis is unclear, but recent research indicates that several factors such as interleukin (IL)-11, transforming growth factor-beta (TGF-β), cyclooxygenase-2, and prostaglandin E2 are associated with bone destruction and metastasis. 4
We describe herein the case of a uterine small-cell carcinoma that was discovered in a patient with quadriplegia caused by cervical spine metastasis.
Case Report
The patient was a 73-year-old Japanese woman, para 5, gravida 1. She consulted with an orthopedist because of numbness in all 4 limbs, but abnormal findings were not identified at that visit. Her symptoms gradually worsened, and she eventually could not move her limbs, thus experiencing quadriplegia. She was taken to the emergency room at another hospital, and she was diagnosed there with a metastatic spinal cord tumor based on the results of magnetic resonance image (MRI). She was therefore transferred to our hospital for treatment of the tumor.
At our hospital’s neurosurgery department, we performed a mitigating operation that partially removed the tumor mass and fixed the spinal bone. The systemic examination of computed tomography (CT) scan revealed the uterine cervical cancer and detected metastasis to abdominal lymph nodes, kidney, and perimetrium.
In a gynecological examination, the patient’s uterine cervix was carcinomatous and bled easily at a touch with cotton. An MRI evaluation revealed that the uterus was completely replaced by cancer tissues (Figure 1). A histological examination was conducted with a specimen from the uterine cervix, revealing cells with enlarged round-shaped nuclei and a high nucleocytoplasmic ratio (Figure 2). Immunochemical staining for synaptophysin, chromogranin A, and neural cell adhesion molecule (NCAM) was all positive (Figure 3).

Abnormal intensity is shown by MRI at the 4th cervical spine, which was replaced by the cancer tissues and clearly infiltrated the spinal cord.
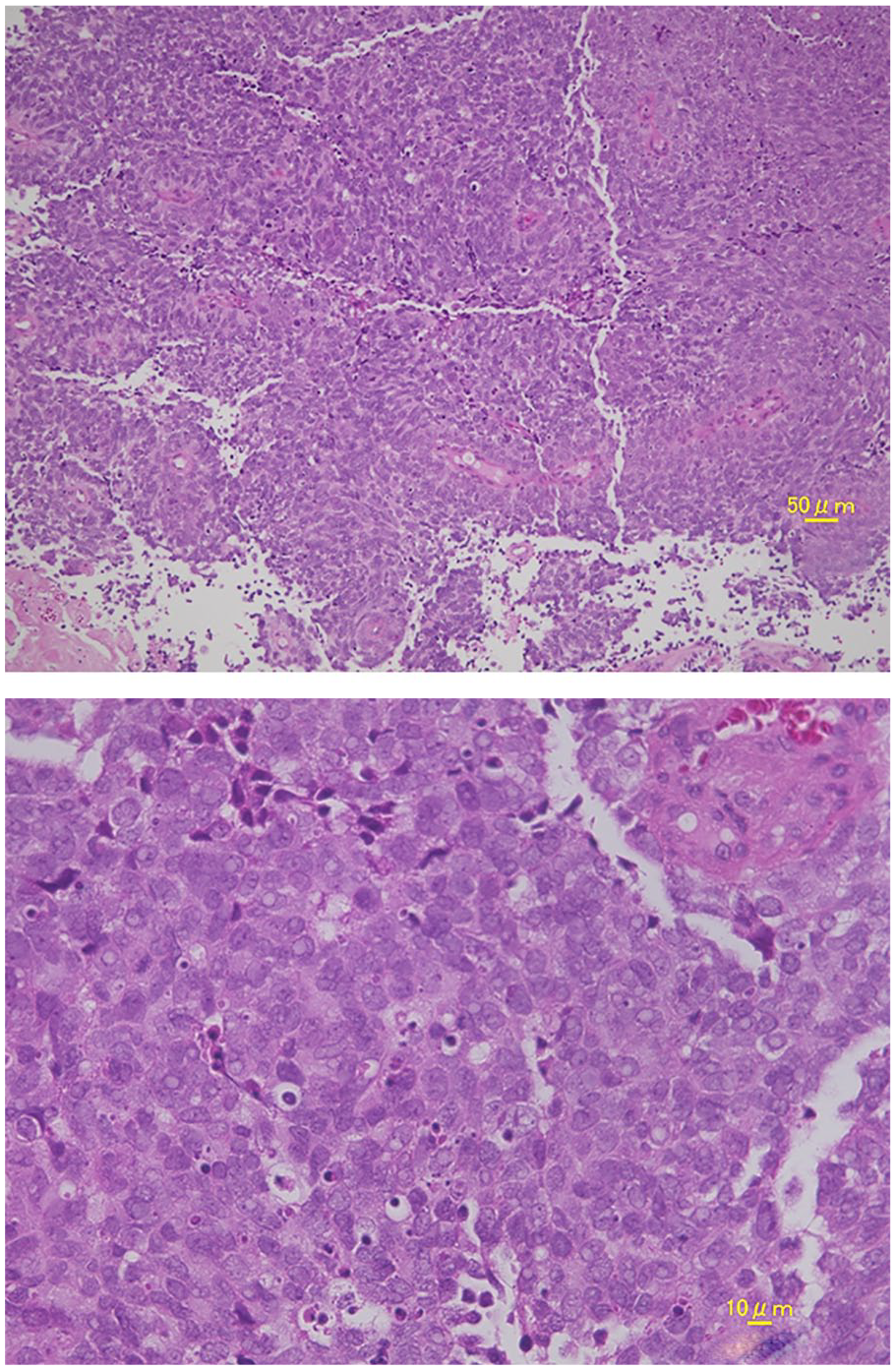
The tumor consisted of diffuse sheets of various sizes of malignant cells with finely granular nuclear chromatin and mitoses. Nucleoli were inconspicuous or absent.

Immunochemical staining for (A) synaptophysin, (B) chromogranin, (C) NCAM indicates neural call adhesion molecules.
Based on the histological findings, we made the diagnosis of small-cell carcinoma. A blood examination revealed elevated values of both neuron-specific enolase (NSE; 27.1 ng/mL, normal range: <16.3 ng/mL) and pro-gastrin releasing peptide (pro-GRP; 2626.5 pg/mL, normal range: <80 pg/mL). The patient could not move her limbs completely due to paralysis, and thus her performance status (PS) was 4. We diagnosed stage IVB uterine small-cell carcinoma and began treatment.
First, radiotherapy (39 Gy) was administered to the metastatic cervical vertebra to improve the functioning of the patient’s limbs, and she then achieved a slight recovery from the paraplegia. We then administered radiotherapy (50 Gy) for the uterine cervical cancer to reduce bleeding from the tumor. After this treatment, the uterine tumor slightly decreased in size, but new metastatic lesions were detected in the lungs, liver, and brain by CT scan.
A further improvement of the patient’s paralysis was observed, but her response was considered “progressive disease” according to the Response Evaluation Criteria in Solid Tumors (RECIST) criteria. We discussed whether additional aggressive treatment should be performed with the patient and her family, and they provided consent for such treatment. It was eventually agreed upon that the treatment plan should be best supportive care, and palliative radiotherapy, pain control, and rehabilitation to improve the patient’s limb functioning were then provided. Within approx. 6 months after the initiation of treatment, the patient died of the cervical cancer.
Discussion
The site of small-cell carcinoma is in the intestine in ~60% of the cases, and in the lung in another ~30%. A small-cell carcinoma from uterine cervical cancer is one of the rarest tumors, accounting for <5% of all uterine cancers, and small-cell carcinomas progress rapidly due to their aggressive behavior. 5 A meta-analysis by Xu et al 5 revealed that the 5-year overall survival (OS) rate for 40 patients with uterine cervical small-cell carcinoma was 20%, which is far lower compared with the 5-year OS rates of uterine cervical squamous cell carcinoma (74.3%) and adenocarcinoma (64.6%).
Among cases of general cervical cancer, there is a group of patients at high risk for human papilloma virus infection, which is associated with the pathogenesis of cancer. However, small-cell carcinoma of the uterine cervix occurs de novo with no relation to this virus infection, and the pathogenesis remains unclear.
General neoplasms are most often discovered in older individuals, but uterine cervical cancer is often detected in young patients. Pan et al 6 studied uterine cervical small-cell carcinomas that occurred during pregnancy, and the average age of their patients was 26.3 years. Those authors reported that over half of their patients with small-cell carcinoma during pregnancy died of that cancer. As patients with gynecological cancers are younger than patients with general neoplasms, another important problem is that the children of patients with gynecological cancer may lose their mothers to the cancer.
Standard treatments for small-cell carcinoma are not established, and this is an aggressive neoplasm. The current treatments for uterine cervical small-cell carcinoma are the same as those used for common cervical cancer. In early-stage (ie, less than stage IIB) small-cell carcinoma, a radical hysterectomy is chosen as the treatment in many hospitals, and radiotherapy and/or systemic chemotherapy are selected for a more progressive status. The Society of Gynecologic Oncology (based in the United States) recommends that for cervical NETs <4 cm, a radical hysterectomy with pelvic lymphadenectomy should be performed, with the option of adjuvant chemotherapy.7,8
The chemotherapy regimen used for small-cell carcinoma is different from that used for common cervical cancer. As is used for lung small-cell carcinoma, a combination of cisplatin and etoposide or cisplatin and irinotecan hydrochloride is usually selected for the first-line chemotherapy of uterine small-cell carcinoma. Our patient’s PS was so poor that systemic chemotherapy was not feasible.
Morinaga et al 4 discussed the mechanisms underlying bone metastasis. They proposed that IL-11 is the most important key factor for bone metastasis, and they noted that the metastatic tumor cells activated by TGF-β increase their levels of IL-11 (which is produced from osteoblasts) to promote bone resorption. Zhang et al 3 reported that the percentage of bone metastasis cases among women with cervical cancer was 2.42%, and the prognoses of their patients with bone metastasis were significantly poor compared with those of their other stage IV patients without bone metastasis. Moreover, they reported that the prognosis of patients with bone metastasis was even worse if the pathology was not squamous cell carcinoma or adenocarcinoma. Our patient’s metastasis to the cervical spine was discovered during an examination for her quadriplegia. After the systemic examination, she was diagnosed as having stage IVB uterine cervical small-cell carcinoma, and her first treatment for the uterine cancer was palliative radiotherapy to the metastatic lesion of the cervical spine, in an attempt to improve the quadriplegia. After radiotherapy, we considered performing systemic chemotherapy, but with the patient’s PS of 4 even after radiotherapy, we decided that systemic chemotherapy was contraindicated for her. She then received palliative care, including pain control, palliative radiotherapy, and rehabilitation for improving her motor function.
The prognosis of uterine cervical cancer with bone metastasis was reported to depend on the existence of other distant metastasis, including the brain and lung. 4 Our patient’s metastasis to the cervical spine, kidney, and pelvic lymph node was detected by CT scans, and her overall survival was a half year. However, she was able to undergo multidisciplinary treatment including palliative care. She could not receive additional chemotherapy, but her cancer pain was well controlled by the decompression surgery of the cervical spine, radiotherapy, and proper drug treatment.
In summary, we treated a patient with cervical spine metastasis of small-cell carcinoma occurring in the uterine cervix. We administered mostly palliative care to improve her quality of life. Standard treatments for small-cell carcinoma in the uterine cervix are not established, and we hope that the standard strategy for NECs developing in each organ will be determined. Early detection and treatment are most important and may lead to the complete cure in some cases.
Footnotes
Author Contributions
Oishi T and Nishida M treated the patient and wrote the paper. Takebayashi K treated the patient. Nasu K and Narahara H made the decision of the treatment for the patient.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.