
Abstract
While treating vascular aneurysms with endovascular technique, short neck and severe bending of the artery are one of the biggest challenges, whether choosing coil embolization or stent-graft (SG) deployment. Here, we report a case with large aneurysm of the splenic artery, which had anomalistically arisen from the superior mesenteric artery and had very severe bending. Because the proximal neck was too short to exclude with SG only, we decided to treat with a combination of coil embolization and SG. At the time of deploying the VIABAHN (self-expandable SG) at the ostium of the splenic artery, the VIABAHN started to deform as the strings were pulled and finally jumped away from the start position. A second VIABAHN was deployed using the sheath-covering technique, which involved alternating short deployment of the VIABAHN with short pullback of the sheath. This report highlights the tricks and traps of deploying VIABAHN at the arteries with very severe bending.
Introduction
Visceral artery aneurysms are a relatively rare clinical entity, discovered in 1% of autopsy cases. Of these, splenic artery aneurysm (SAA) is the most common form, involving approximately 60% of the visceral artery aneurysms. 1 There are several options to treat SAA, including coil embolization, endovascular exclusion with membrane-covered stents, ligation, and simultaneous resection and revascularization. 2 Advances in techniques and equipment have resulted in an increase in the successful endovascular treatment of SAA over time. While treating vascular aneurysms with endovascular technique, short neck and severe bending of the artery are one of the biggest challenges, whether choosing coil embolization or stent-graft (SG) deployment.
Case Presentation
A 75-year-old man presented with an incidentally discovered large aneurysm of the splenic artery (SA), which had anomalistically arisen from the superior mesenteric artery (SMA) (Figure 1A). Computed tomography (CT) revealed saccular morphology and a maximum diameter of 60.8 mm (Figure 1B), both of which inspired invasive treatment. After extensive discussion among the heart team and with the patient, we decided to treat the SAA with endovascular exclusion. However, the proximal neck of SA was approximately 5 mm on the stretched view of curved planar reconstruction images of the CT (Figure 1C and D). The proximal landing zone was too short to treat with an SG alone or coil embolization for main trunk of SA; the neck of SAA was too thick for complete coil packing. Therefore, we decided to exclude the aneurysm using a combination of coil embolization and an SG. As the diameter of the proximal vessel was approximately 6 mm, we planned to use 7 mm self-expandable SG (VIABAHN; W.L. Gore, Flagstaff, AZ) because self-expandable SG is more flexible, adaptable, and suitable than rigid, balloon-expandable SG for visceral artery aneurysms due to the tortuosity of visceral arteries. 3 Owing to its bulkiness, it seemed difficult to deliver the SG across the bending portion of SA without prior advancement of guiding catheter to the distal portion of SA. Therefore, we planned to, first, start with coil packing of SAA, followed by SG deployment after removal of the microcatheter from the aneurysm.

Computed tomography of a large aneurysm of the splenic artery (SA). (A) Computed tomography showing a large aneurysm of the SA arising from the SMA. (B) Axial image of maximal diameter of SA aneurysm (SAA). (C and D) The stretched view of curved planar reconstruction images showing the (C) bifurcation of SA and (D) ostium of SAA. SMA indicates superior mesenteric artery.
A 7F guiding sheath (Flexor Ansel 3; Cook Medical, Bloomington, IN) was engaged to SMA via the right femoral artery. Angiography confirmed that a highly bending SA diverged from the SMA, and the aneurysm was located approximately 5 mm from the bifurcation (Figure 2A; Online Video 1). Following coil embolization (Ruby Coil COMPLEX STANDARD; Penumbra Inc., Alameda, CA; and Target coil; Stryker, Portage, MI) (Figure 2B), we tried to advance the guiding catheter. However, we cannot advance the guiding catheter to the distal portion of SA across the SAA and to the bending portion of SA, even using balloon anchoring and squeezing technique with 7 mm balloon (SHIDEN 7.0 × 50 mm; Kaneka Corporation, Tokyo, Japan). As GuideLiner PV (Vascular Solutions Inc., Minneapolis, MN) could pass the bending portion of SA with balloon anchoring and squeezing technique, 4F straight catheter (Glidecath; Terumo, Tokyo, Japan) was advanced to the distal SA and Amplatz Extra-Stiff Support guide wire (Cook Medical) was placed. Subsequently, the guiding sheath could be advanced across the bending portion of SA along the Amplatz Extra-Stiff Support guide wire. After exchanging the guide wire to 0.018-inch support wire (Thruway; Boston Scientific, Marlborough, MA), we tried to deploy the SG (VIABAHN 7.0 × 50 mm) at the ostium of the SA (Figure 2C; Online Video 2). However, the SG started to deflect as the suture was pulled and finally jumped away from the start position (Figure 2D; Online Video 3). A second SG (VIABAHN 7.0 × 50 mm) was deployed using the sheath-covering technique, which involved alternating short deployment of the SG with short pullback of the sheath (Figure 3; Online Video 4). Final angiography showed complete exclusion of the aneurysm (Figure 2E; Online Video 5). After the procedure, we planned to perform abdominal ultrasound at 1, 6, 12 months and every 12 months (Figure 4).
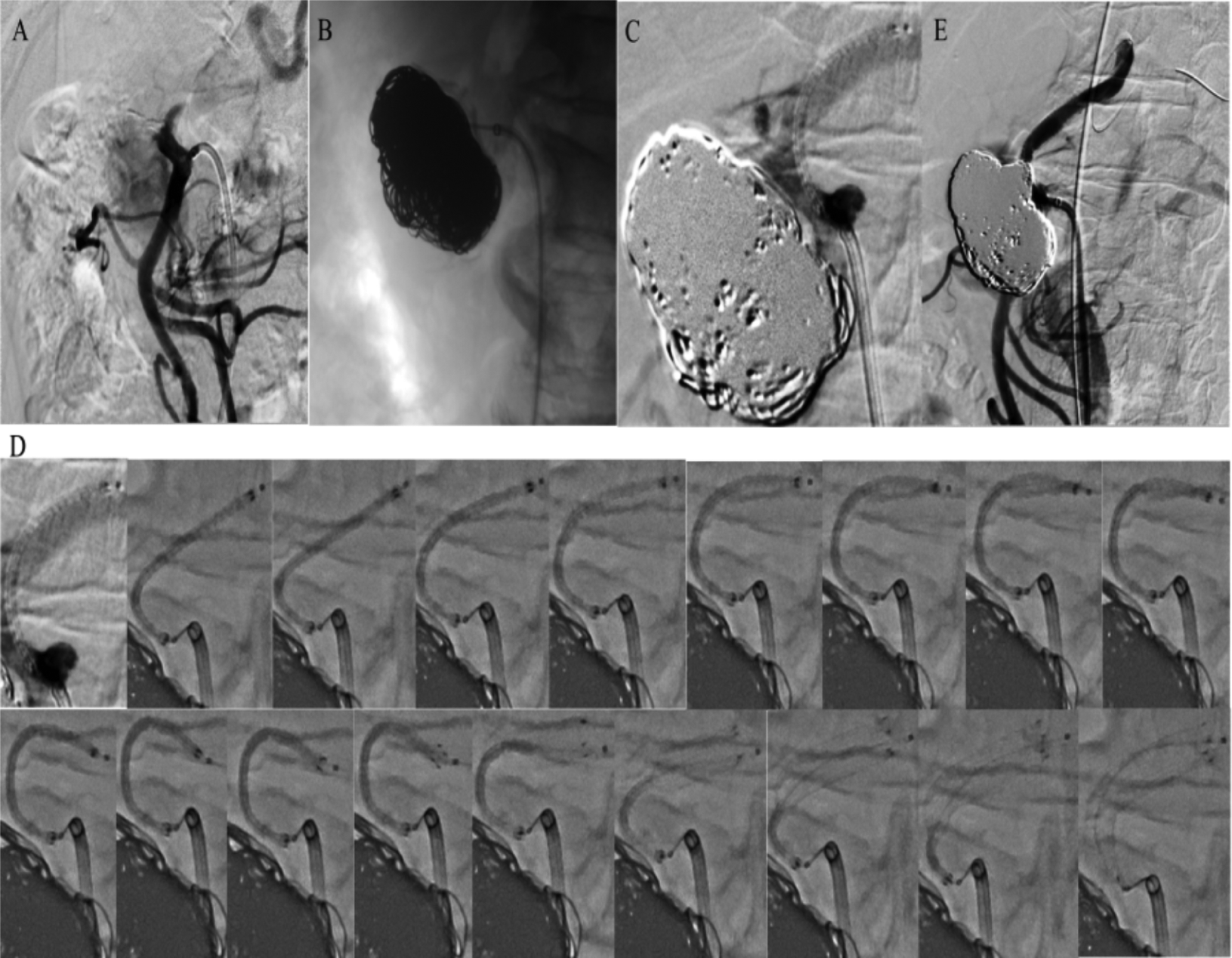
Angiography, coil embolization, and deployment of self-expandable stent-graft (SG). (A) Preangiogram confirmed the large aneurysm and short proximal neck. (B) Angiogram after coil embolization. (C) Start position of the SG. (D) A sequence of images during SG deployment showing deformation of the SG and dive into the splenic artery. (E) Final angiogram showing complete exclusion of the aneurysm.
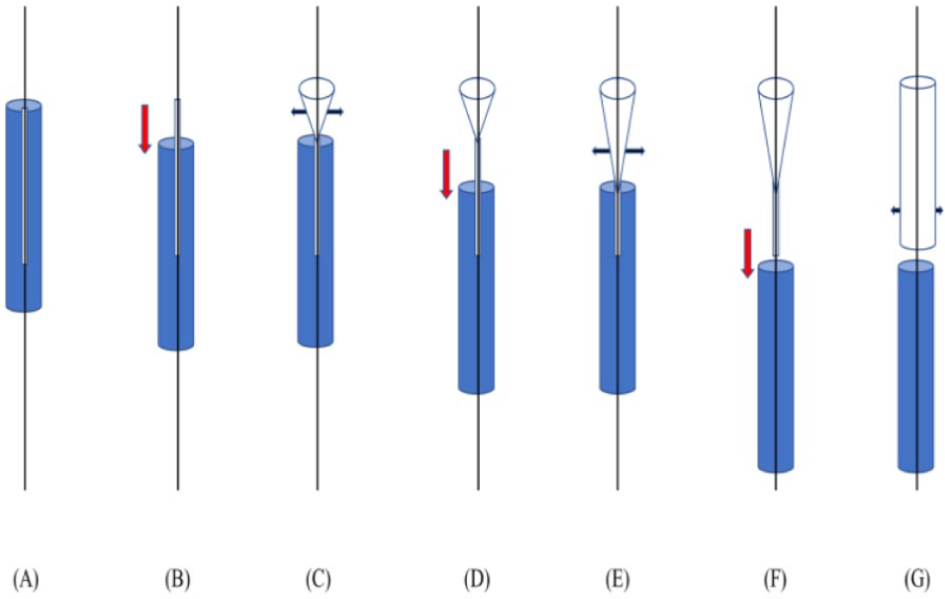
Schema of sheath-covering technique. (A) Deliver stent-graft (SG) together with the sheath across the lesion. (B) Short pullback of the sheath. (C) Short deployment of the SG. Repeat (B) and (C) little by little (D-G).

One year follow-up images of abdominal ultrasound (AUS). (A) The AUS showed that the maximal diameter of splenic artery aneurysm was unchanged (approximately 60 mm). (B-D) The implanted stent-graft was patent.
Discussion
Here, we present a case of incidentally discovered large aneurysm of the SA with very short proximal landing zone and severe bending of main trunk, which leads to the migration of first self-expandable VIABAHN SG and necessity of second SG. This case well represents the characteristics of self-expandable VIABAHN SG as well as highlights tricks and traps of deploying VIABAHN SG at very severe bending portion.
Previously, a similar case of VIABAHN SG migration was reported in an attempt to treat popliteal aneurysm. However, the present case illustrates more severe bowstring phenomenon. 4 This is a VIABAHN-specific phenomenon which results from its unique structure and deployment mechanism. The SG was covered by a polytetrafluoroethylene (PTFE) jacket, and deployment was accomplished by pulling on a PTFE suture that opens the constraining tetrafluoroethylene jacket from around the device. Furthermore, the direction of deployment is in a tip to hub. If the SG is placed in a severe bending portion, aggressive tension on the PTFE suture could bow the tip of the delivery system, known as the bowstring phenomenon. 5 In the present case, despite using 0.018-in stiff support guide wire, this phenomenon occurred. VIABAHN SG of less than 9 mm diameter is 0.014/0.018-in guide wire compatible; therefore, stiffer 0.035-in guide wires, such as Amplatz Extra-Stiff Support guide wire, could not be used. Accordingly, the sheath-covering technique is the only solution which can prevent SG migration in severe bending vessels, although the precise positioning of proximal landing is difficult without using double guiding technique owing to impossibility of angiography.
Conclusion
When implanting a self-expandable VIABAHN SG in highly bending lesion, extreme care should be taken, and the sheath-covering technique is a useful option.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
R.Y. contributed to the initial conceptualization of the research design, data collection, data analysis, interpretation of the results, writing in all sections of the manuscript and serves as a guarantor of the integrity of manuscript. K.T. contributed to the interpretation of the results, critically revised the manuscript and serves as a guarantor of the integrity of manuscript. Y.M., S.K, and I.M. contributed to the oversight and general feedback on the manuscript.
Informed Consent
The patient provided consent for participating in this case report and to publish it.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.