
Abstract
Transient contrast neurotoxicity is a rare but well-recognized complication of angiography that is due to neurotoxicity of the contrast agent. Patients with renal dysfunction may be inclined to develop contrast medium neurotoxicity due to delayed elimination of the contrast medium in renal metabolism. In this report, we present an unusual case of transient neurotoxicity in a patient with severe chronic kidney disease following percutaneous coronary intervention mimicking clinically and radiologically subarachnoid hemorrhage. The patient’s clinical symptoms improved rapidly and fully recovered after hemodialysis and conservative treatment. We believe that performing early hemodialysis is an effective treatment to improve symptoms in end-stage renal disease patients with contrast-induced encephalopathy.
Introduction
Contrast-induced encephalopathy (CIE) which is a transient phenomenon associated with the use of intravascular radiocontrast media is a very rare complication of angiography. Clinical effects of neurotoxicity from iodinated contrast agents include encephalopathy, seizures, cortical blindness, and focal neurological deficits, such as ophthalmoplegia.1,2 Although all types of contrast media agents irrespective of their osmolarity or ionic states can induce CIE, the excess amount of iodinated contrast is considered as a major risk factor. 1 Neurologic findings generally appear 2 to 12 h after the contrast injection and usually resolve within 24 to 72 h.2,3 Owing to various clinical presentations, it gives rise to a broad differential diagnosis and imaging, which is important in excluding hemorrhagic and thromboembolic complications of coronary angiography. Typical radiological findings include cerebral edema and cortical enhancement. 4 Although there are many case reports in the literature describing CIE following use of contrast agents in diverse procedures such as cerebral or carotid, it has been reported quite rare after coronary angiography.5-7 Herein, we report a case of a 68-year-old man who developed CIE mimicking subarachnoid hemorrhage following coronary angiogram in a patient with moderate chronic kidney disease. The patient has given consent for publication of this report.
Case Report
A 68-year-old man with a history of diabetes mellitus (DM), hypertension, coronary artery disease, and severe renal impairment with an estimated glomerular filtration rate of 27 mL/min/1.73 m2 was admitted to outpatient clinic with chest pain. He has suffered from type 2 DM for 15 years and renal impairment for 3 years as a complication of DM. The patient has no contrast matter exposure recently. We performed an elective coronary angiography and implanted 2.75 mm × 38 mm and 3.0 mm × 15 mm drug-eluting stents into the mid-portion of the circumflex artery to relieve symptoms of angina. Coronary angioplasty was performed by using 230 mL of iohexol (BIEMEXOL® 300), which is a slightly higher dosage compared with standard coronary intervention. After 4 h from the procedure, the patient has realized that he had twitching in his left foot. First, we suspected that it arised from nerve irritation caused by puncturing the femoral arterial access. After a while, it turned into a generalized tonic-clonic seizure that ended spontaneously after 20 s. Two hours later, he had another generalized tonic-clonic seizure, which was longer than the first. The seizure was terminated with midazolam (2 mg iv). Postictally, the patient suffered from dizziness, vomiting, and somnolence. Then, he has started on antiepileptic treatment with loading dose infusion of sodium valproate, and then a daily dose of 500 mg 2 times a day. Although the patient has been evaluated neurologically, non-contrast head computerized tomography (CT) was performed immediately without contrast agent to exclude the potential causes of the seizure such as subarachnoid hemorrhage. Cranial CT scan revealed that there is a faded image of right frontal lobe sulci and there are hyperdense fields at the vertex and at the right frontal lobe (Figure 1A and B). The cranial arteries and veins are also filled with contrast matter. Initially, we could not be certain of whether those hyperdense fields are subarachnoid hemorrhage or contrast extravasation due to recent coronary angiography and usage of contrast agent. Hence, he was commenced on dexamethasone and mannitol for anti-edema treatment. Besides the seizures, the patient’s metabolic parameters have shown progression, he developed metabolic acidosis and hyperkalemia and had progression of renal function tests (pH: 7.30, K: 6 mEq/L, and creatinine: 4 mg/dL). After the patient was unresponsive to verbal commands and developed confusion and disorientation, he was transitioned to hemodialysis immediately about after 24 h from the first seizure for rapid removal of contrast agent and improve the metabolic acidosis and hyperkalemia. Non-contrast head CT scanning performed 48 h after the onset of symptoms showed sulcal effacement in the right cerebral hemisphere due to cerebral swelling (Figure 2). The neurological symptoms fully resolved after performing hemodialysis a second time and conservative treatment. During the observation period after the first hemodialysis, the patient remained seizure-free. A magnetic resonance imaging (MRI) and MR angiography at 90 ho from patient’s symptoms showed no sign of bleeding no edema and no swelling or cortical enhancement on the T1-weighted images (T1WIs) or on the fluid-attenuated inversion recovery (FLAIR) images (Figure 3A to C). Subarachnoid hemorrhage was also ruled out by the absence of any hyperdensity in the sulci on the MRI and the control CT. Actually, CIE was diagnosed based on the patient’s clinical findings recovery and aforementioned cerebral imaging. Furthermore, the clinical symptoms started 4 h after the contrast injection and neurological recovery occurred after approximately 60 h. The patient has taken to the routine hemodialysis program and he was transferred to the nephrology department after 6 days from the procedure.

Non-contrast head computerized tomography 6 h after the coronary angiogram showing intravascular contrast with cortical staining and effacement of the sulci in the right frontal lobe.

Non-contrast head computerized tomography image taken after 48 h indicating sulcal effacement in the right cerebral hemisphere due to cerebral swelling and no contrast enhancement in the right frontal lobe.
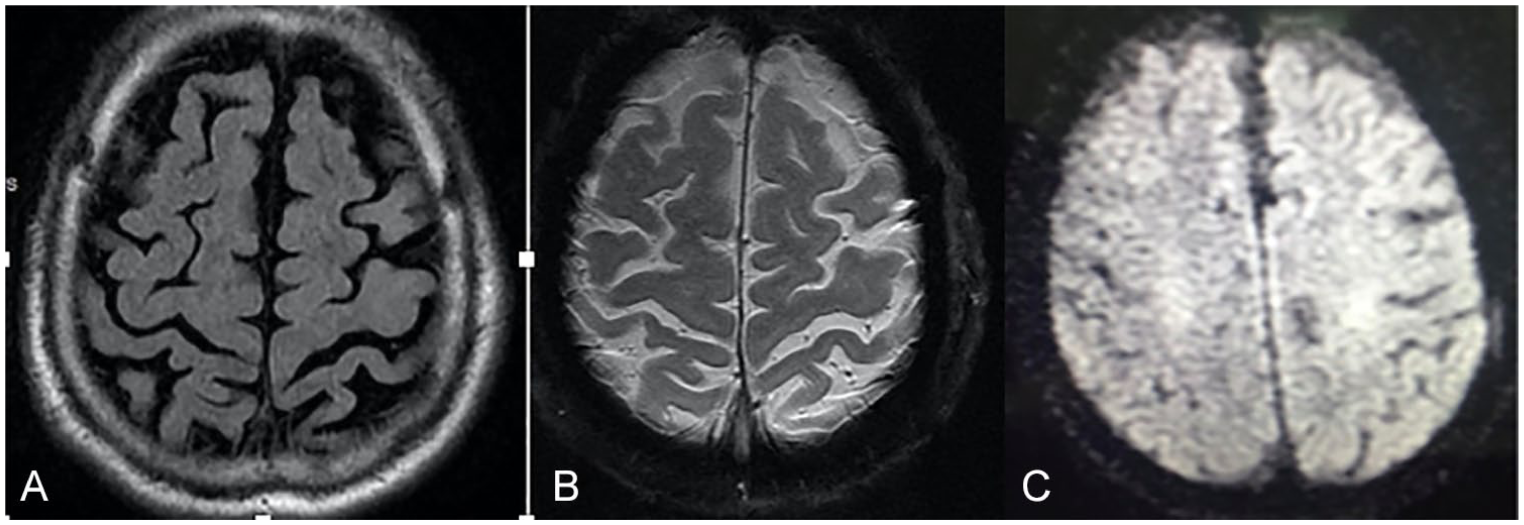
Normal cranial diffusion MRI performed a mean 90 h after the onset of symptoms. MRI images revealing that the contrast agent was reabsorbed from the subarachnoid space and showing no hemorrhage or ischemia: (A) flair, (B) SWI (susceptibility weighted imaging), and (C) diffusion sequence.
Discussion
Neurotoxicity caused by iodinated contrast agents used in angiography is an uncommon but important complication. Neurointerventional procedures are more commonly associated with CIE because repeated intracranial selective injections of smaller volume contrast agent may cause dysfunction of the blood-brain barrier directly. 3 Therefore, the incidence of CIE ranges between 0.3% and 1.0% irrespective of procedure type, whereas the incidence is 0.06% for the patients undergoing coronary angiography.7,8 Although the detailed mechanism of CIE is unclear, it is considered to be an osmotic disruption of the blood-brain barrier and cerebral edema from the hyperosmolar contrast.1,9 Another potential mechanism is that repeated injections of contrast agents within several minutes may result in neurotoxic effects. 10 The risk factors for developing CIE include male sex, advanced age, hypertension, impaired kidney function, injection of large volumes of contrast media, and underlying brain disturbances.1,3,11 The aforementioned patient was male, he had moderate chronic kidney disease, controlled hypertension, and for the culprit coronary angioplasty procedure, 230 mL of Iohexol had been used. It is likely that delayed elimination of the contrast medium in renal metabolism facilitates developing contrast medium neurotoxicity. 12
Clinical examination and imaging follow-up would help in confirming the diagnosis and excluding thromboembolic and hemorrhagic complications. Brain CT without contrast may be normal or, as in our patient, show a combination of poorly localized cortical and/or subcortical enhancement, cerebral edema, and hyperdensity in the subarachnoid space similar to subarachnoid hemorrhage. 13 MRI may demonstrate hyperintense areas in the affected cortices on T2, FLAIR, and diffusion-weighted images. 14 The localized and rapid recovery of the neurological deficit with complete resolution of contrast staining on follow-up CT effectively help the differential diagnosis. 7 In our case, the patient was initially assessed as a hemorrhagic stroke according to the first brain CT. Then, the diagnosis interpreted as a CIE based on MRI, follow-up CT, and rapid recovery of neurologic findings.
The prognosis of CIE is excellent. Although there is no specific treatment for this condition, symptomatic treatments such as anticonvulsant therapy with benzodiazepines for seizures, 15 hydration, and close observation of the patient in the immediate postprocedural period are usually sufficient. 3 In addition, contrast media can be effectively removed from the blood by dialysis in patients with chronic kidney disease.
In conclusion, we reported a rare case of CIE following percutaneous coronary intervention in a patient with chronic kidney disease, who was treated by performing early hemodialysis to remove contrast agents. CIE is a rare condition that should be kept in mind as an expected complication during angioplasty, especially in patients with end-stage renal disease (ESRD).
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
ECS wrote the first draft of the manuscript. EE contributed to the writing of the manuscript. RU contributed with the images. IM performed coronary intervention. AOY, CE, CS, and ECS made contributions to the acquisition of the clinical data. CE and CS made critical revisions and approved the final version. All authors reviewed and approved the final manuscript.