
Abstract
Epstein-Barr virus (EBV) infection might induce not only posttransplantation lymphoproliferative disorder (PTLD) but also leiomyosarcoma. We report a case of EBV-associated leiomyosarcoma concurrently with PTLD after renal transplantation. The patient was a 30-year-old woman who underwent living donor kidney transplantation at 27 years of age. Preoperative EBV viral capsid antibody immunoglobulin M, immunoglobulin G (IgG), and EBV nuclear antigen IgG were negative. Multiple lung and liver tumors were detected 1.5 years after transplantation. She was diagnosed with PTLD after tumor biopsy. Her EBV DNA was 110 copies/mL detected by real-time polymerase chain reaction when PTLD was diagnosed. She received dose reduction of immunosuppressive therapy and several chemotherapies. Because her hepatic lesion was still progressive while pulmonary lesion was reduced, a liver tumor biopsy was performed, but the biopsy specimens were necrotic. A left lateral segmentectomy was performed as a third biopsy for treatment-resistant hepatic lesion 2.5 years after her first PTLD diagnosis. Pathologically, she was diagnosed with EBV-associated leiomyosarcoma. She was treated with sirolimus, but died 7 months after the operation. This is the first case of the coincidence of leiomyosarcoma associated with EBV and PTLD. This case was exceedingly rare; however, we must consider the coincidence of leiomyosarcoma associated with EBV and PTLD when encountering treatment-resistant PTLD.
Keywords
Introduction
Epstein-Barr virus (EBV) infection, which has the potential to induce neoplastic disease, is one of the most important complications after organ transplantation. Primary EBV infection after transplantation from an EBV-immunoglobulin G (IgG)-seropositive donor to an EBV-IgG-seronegative recipient is known to be associated with a higher risk of posttransplantation lymphoproliferative disorder (PTLD), which is induced by the infection of B lymphocytes. Epstein-Barr virus infection might also induce leiomyosarcoma, which can be diagnosed based on the detection of Epstein-Barr virus–encoded small RNA (EBER) in tumor tissue.
Herein, we report a rare case of the coincidence of leiomyosarcoma associated with EBV and PTLD after renal transplantation.
Case Description
The patient was a 30-year-old woman. She was admitted to our hospital to examine advanced liver tumors. She began to receive hemodialysis due to lupus nephritis when she was 15 years of age. She had undergone ABO blood type–incompatible kidney transplantation from a living relation (the donor was her mother) 4 years ago. She underwent splenectomy 2 weeks before transplantation and 3 double-filtration plasmapheresis and plasma exchanges and was treated with mycophenolate mofetil (MMF; 1000 mg, daily, orally), tacrolimus (4 mg, daily, orally), and prednisolone (10 mg, daily, orally) for 4 weeks as hyposensitization therapy. Basiliximab (20 mg, intravenous) was administered on days 0 and 4 after transplantation, and oral treatment with tacrolimus, MMF, and prednisolone was maintained as immunosuppressive therapy. A preoperative serum examination was negative for EBV viral capsid antibody immunoglobulin M (IgM), IgG, and EBV nuclear antigen IgG.
Multiple lung and liver tumors were detected 1.5 years after transplantation (Figure 1A and B), and a biopsy revealed PTLD (diffuse large B-cell lymphoma). Epstein-Barr virus DNA (110 copies/mL) was detected in whole blood by a real-time polymerase chain reaction at the time of PTLD diagnosis. Tacrolimus and MMF were reduced to half dosage, and rituximab (400 mg, intravenous, weekly) was administered 8 times. Dynamic computed tomography after this treatment revealed stable disease of the pulmonary lesion and progressive disease of the hepatic lesion. Thus, tacrolimus was withdrawn, and additional chemotherapy agents were introduced to treat the tumor, including rituximab, CHOP (cyclophosphamide, doxorubicin, vincristine, and prednisolone), EPOCH (etoposide, prednisone, vincristine, cyclophosphamide, and doxorubicin), irinotecan with doxorubicin, and MINE (mesna, ifosfamide, novantrone, and etoposide). After these treatments, the pulmonary lesions gradually reduced. In contrast, no treatment was able to control progression of the hepatic lesion. A liver biopsy was performed because the hepatic lesion continued to progress while the pulmonary lesion decreased in size (Figure 1C and D); however, only necrotic tissue was detected. Additional treatments, including etoposide and rituximab, were continued. However, liver tumors had further progressed, and she had got abdominal pain. At this time, neck pain appeared, and a spinal tumor was detected on magnetic resonance imaging (Figure 2).

(A and B) Computed tomography (CT) before treatment for posttransplantation lymphoproliferative disorder. Large tumors are present in the left lung (arrow) and left lobe of the liver (arrowhead). (C and D) CT before segmentectomy of the liver. Due to administration of several chemotherapy agents, the left lung tumor was reduced in size. In contrast, the size of the tumor in the left lobe of the liver increased (arrowhead).

Magnetic resonance imaging before liver segmentectomy: (A) sagittal plane and (B) coronal plane. A spinal tumor was detected at the level of C2 (arrow).
After hospitalization, left lateral segmentectomy was performed as the third biopsy of the treatment-resistant hepatic lesion. A pathologic examination observed a foci of spindle-type cells with normal tissue dispersed around the tumor. Several mitotic figures were detected (Figure 3A and B). Immunohistochemical staining was positive for alpha-smooth muscle actin (α-SMA) and negative for CD20, CD34, S100, and c-kit (Figure 3C). Finally, the tumor was diagnosed as EBV-associated leiomyosarcoma based on the detection of EBER in the spindle cells (Figure 3D).
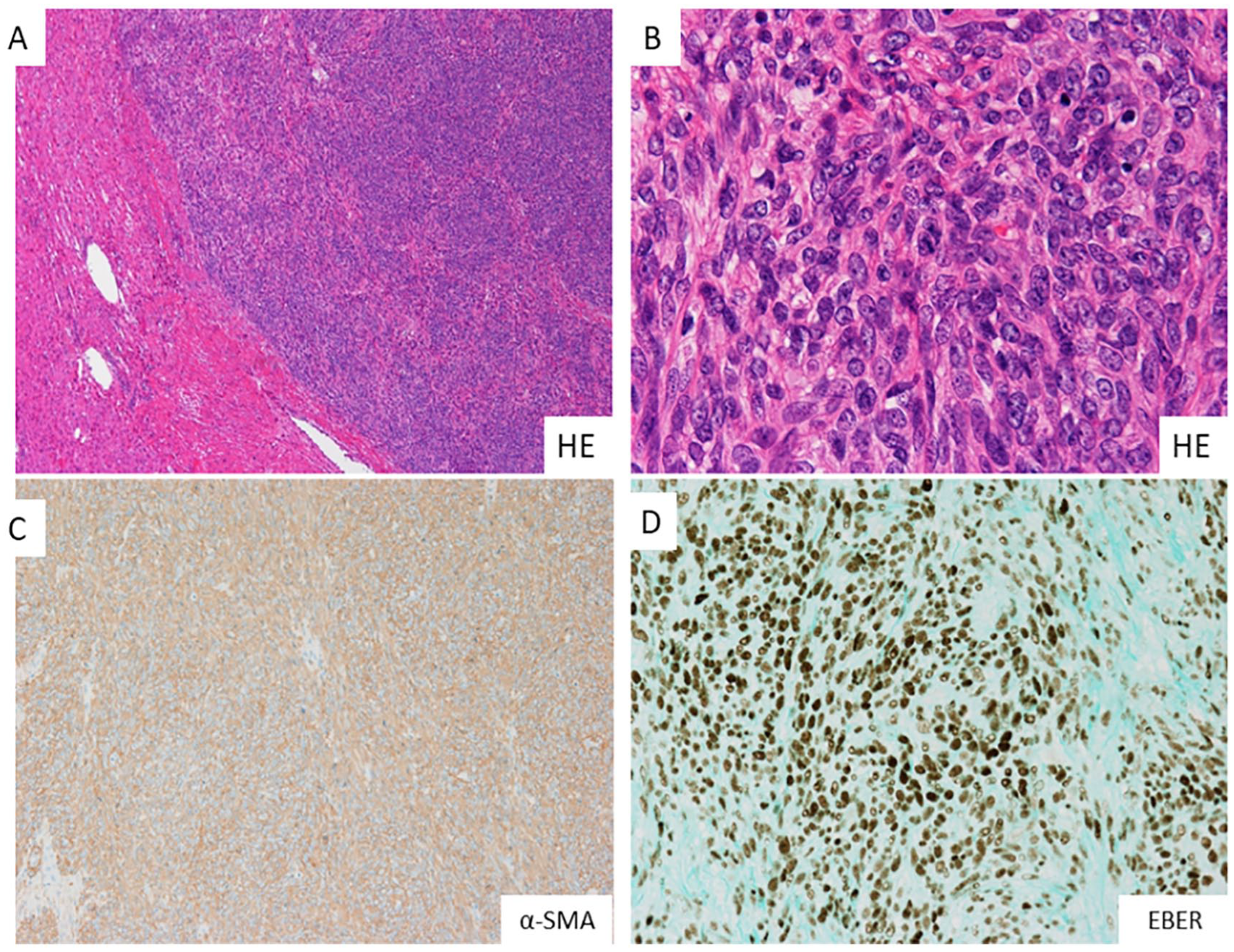
The histopathology of the tumor. Hematoxylin-eosin (HE) staining (A) ×20, (B) ×200 and immunohistochemical staining, (C) α-SMA, and (D) EBER. (A) The cellularity of the tumor tissue is very high. Tumor cells spread into the normal tissue around the tumor. (B) The tumor cells were spindle type. Numerous mitotic figures were detected. (C and D) The tumor was positive for α-SMA and EBER. α-SMA indicates alpha-smooth muscle actin; EBER, Epstein-Barr virus–encoded small RNA.
The patient was treated with sirolimus (2 mg, daily), but died 7 months after the operation.
Discussion
Primary EBV infection occurs with subclinical or nonspecific symptoms for most people. It is conceivable that EBV would remain as a dormant infection in host cells, such as B lymphocytes, T lymphocytes, natural killer (NK) cells, or epidermal cells, and it is reported to be a cause of neoplasms, such as Burkitt lymphoma, NK/T lymphoma, upper pharynx cancer, and gastric cancer. 1 Lee et al 2 and McClain et al 3 recently reported a relationship between EBV infection and an incidence of leiomyosarcoma in patients under immunosuppression.
Searching for transplantation, EBV, and leiomyosarcoma as keywords in PubMed database, only 16 cases of EBV-associated leiomyosarcoma in organ transplant recipients have been reported, including our case (Table 1).4-17 The median age at the onset of leiomyosarcoma was 20 years, with a median of 2.5 years after transplantation. Although the onset of leiomyosarcoma occurred within 5 years after transplantation in 14 of these cases, in 2 cases, the onset was at more than 10 years after transplantation; thus, the distribution is bimodal. The onset of leiomyosarcoma after transplantation tends to be earlier in younger recipients; ie, the median age of the patients who developed leiomyosarcoma within 5 years after transplantation was 12 years, whereas the median age of patients who developed leiomyosarcoma within 10 years (late onset) after transplantation was 36 years.
Cases of EBV-associated leiomyosarcoma in organ transplant recipients.
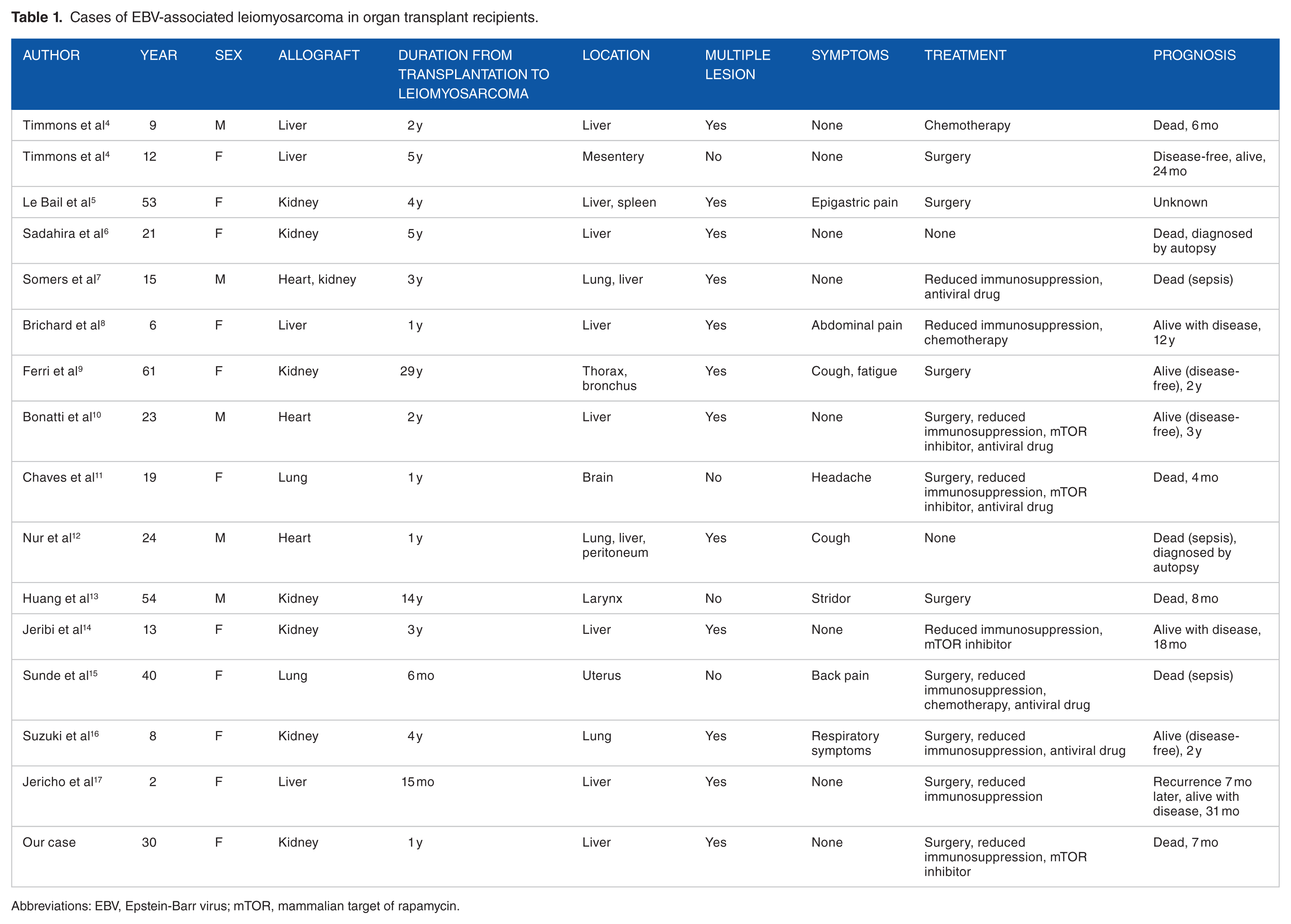
Abbreviations: EBV, Epstein-Barr virus; mTOR, mammalian target of rapamycin.
Leiomyosarcoma most commonly occurs on the extremities, followed by abdominal/retroperitoneal sites. 18 However, in the reports that we reviewed, leiomyosarcoma after organ transplantation occurred in the liver in 14 cases and in the lung in 3 cases. In 2 cases, leiomyosarcoma developed in the central nervous system, which is a common site of occurrence in patients with PTLD. More than 60% of the patients had multiple lesions. Although leiomyosarcoma tends to undergo blood-borne metastasis to sites such as the liver and lung, it was reported to occur multicentrically and with monoclonal growth of each lesion in cases of EBV-associated leiomyosarcoma. 19 Most cases of leiomyosarcoma are asymptomatic, whereas most patients with PTLD are symptomatic. Therefore, it is important for transplant recipients to undergo regular tumor screening. Leiomyosarcoma should be diagnosed by biopsy; however, it is sometimes difficult to diagnose based on fine-needle biopsy because of the small amount of material that is collected. Thus, some cases may require surgical biopsy, similar to our case.
The primary therapy for leiomyosarcoma is surgical removal. In contrast, the primary therapy for PTLD is medication. Jonigk et al 20 reported that reduction of immunosuppression may be effective for EBV-associated leiomyosarcoma, similar to the management of PTLD. Furthermore, some reports suggest that the mammalian target of rapamycin (mTOR) inhibitor, which is one of the immunosuppression drugs, is effective against leiomyosarcoma.21,22 Therefore, it is considered to change the immunosuppression drug to the mTOR inhibitor when patients are diagnosed with leiomyosarcoma. Only 4 of the 16 cases that we reviewed achieved disease-free survival; however, all 4 cases were treated by multimodal treatment including surgical resection. This suggests that surgical removal is recommended for a patient with EBV-associated leiomyosarcoma.
This is a rare case of the coincidence of leiomyosarcoma associated with EBV and PTLD. Reduction of immunosuppression may be effective for both EBV-associated leiomyosarcoma and PTLD. However, subsequent treatment is different in both. Thus, it is important to distinguish between both diseases. Although the present case was exceedingly rare, it suggests that physicians should consider the possible coincidence of leiomyosarcoma in association with EBV and PTLD in cases involving treatment-resistant PTLD.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
All authors contributed to the writing of the manuscript.
Informed Consent
Informed consent was obtained from the patient.