
Abstract
A rare complication-basilic vein thrombus of brachial access was reported by duplex ultrasound in this case 2 days after stenting implantation surgery on the left iliac artery via brachial access. More attention should be paid on the procedure of artery access puncture in operation to avoid the unexpected complications.
With the development of vascular surgery, alternative options for the treatment of complex aortoiliac artery disease have been proposed. Because the “traditional” femoral artery approach may not deal with some hard conditions well in clinical, like severe aortoiliac artery disease, 1 obesity, skin infections of the groin, multiple femoral catheterization, or previous groin surgery. Furthermore, patients who have undergone aortic reconstructions with neo-bifurcations previously may face difficulty during endovascular treatment via a trans-femoral access. 2 Therefore, other alternative access needs to be evaluated, such as brachial or radial way which has been used in coronary interventions for many years. 3 Transbrachial access for lower extremity interventions has an advantage over radial method on its larger diameter and less complication (eg, artery occlusion). 3 Some reports have shown its complication rate is 6.5%, including artery thrombosis, hematomas, artery bleeding, puncture site infection, pseudoaneurysm, or nerve defect.3–5 Venous thrombosis after transbrachial artery access represents a rare, if not, under-reported complications, such as pulmonary embolism (PE), which is life-threatening and costs a lot, operators should learn it well and try to avoid this complication. In this case, patient informed consent for publication was granted.
Case Report
A 61-year-old man with left extremity pain for 4 years and intermittent claudication for 1 year was diagnosed as occlusive iliac disease which was demonstrated by computed tomography (CT) scan and physical test that showed no pulsation on the left femoral artery, and weak on the right. Because of the severe stenosis of the contralateral femoral artery, transbrachial access was chosen to perform the intervention (Figure 1A to C) with routine heparinizing (12 500 U heparin was dissolved in 10 mL 0.9% NaCl, 0.1 mL/kg). Compression bandaging was applied on the puncture site after surgery. The radial pulsation could be monitored after compression. Low molecular weight heparin (LMWH, 100 AXa IU/kg, q12h) begun to be used after 6 h.
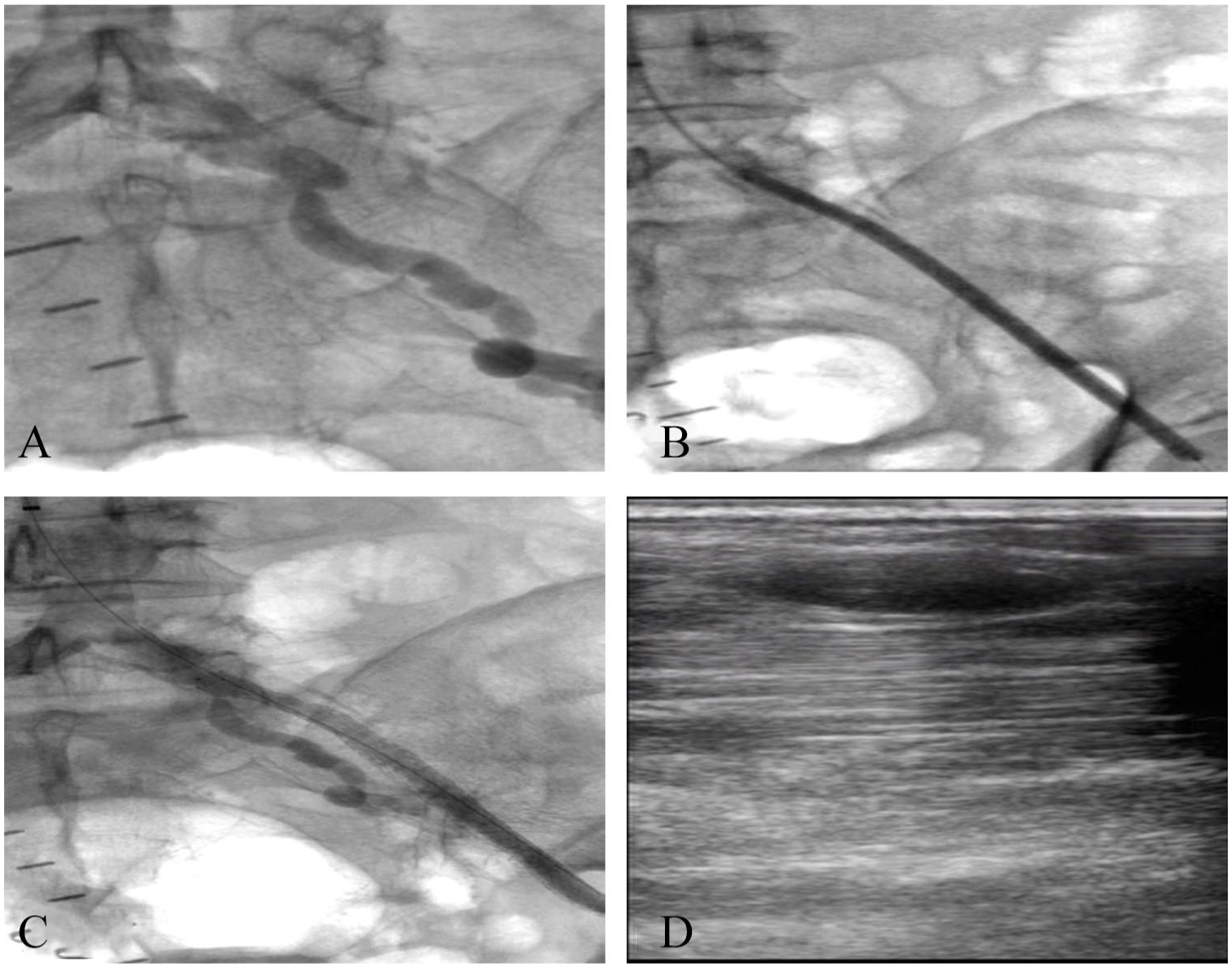
(A) The contrast venography of left iliac artery before surgery, an occlusion was shown; (B) the dilation of the occlusive iliac artery with balloon; (C) the venography shows the well perfusion of the left iliac artery after implanting stent in artery; (D) the duplex ultrasound picture of brachial artery 2 days after surgery.
However, on the next day, there was a distending pain on the patient’s left upper medial arm without skin color or temperature changes, or cutaneous edema. Duplex ultrasound demonstrated the thrombus existed in the vena basilica (Figure 1D) which is close to the arterial puncture point, and the venous wall was coarse. Anticoagulation was applied with LMWH (100 IU, q12h) for 3 days in hospital and Devashaban (20 mg, qd) after discharge. The pain had retrieved and the ultrasound showed complete patency of the vena basilica after anticoagulation for 5 months.
Discussions
Upper extremity deep vein thrombosis (UEDVT) is a rare disease and accounts for only 1% to 4% of all deep vein thrombosis (DVT) events (including DVT in the lower extremities). 1 In turn, upper extremity superficial vein thrombosis (UESVT) accounts for 50% of upper extremity venous thrombosis (UEVT). 6 And in superficial vein thrombosis (SVT), the great saphenous vein accounts for 60% to 80% of cases, and the small saphenous vein for 10% to 20%, 7 and SVT could also develop in the chest wall or the penis (Mondor disease), or the neck. 8 Thus, similar with UEDVT, UESVT is also a rare disease in clinical. It is defined as thrombophlebitis which is thrombosis localized in the cephalic vein, median cubital vein, or basilic vein. In which, secondary UESVT is mainly caused by the irritation of intravenous infusion treatment (such as intravenous Amiodarone), 9 pregnancy, infectious disease, intravenous catheters, malignancy, Behcet’s disease, Buerger’s disease, Mondor’s disease. 8 The SVT has long been considered as a benign disease. However, there are reports showed the SVT accompanied by DVT in 6% to 36% of patients, and PE in ~33% of patients. 10 And the extension of SVT within 3 cm of the junction may be regard as serious as a proximal DVT. 10 Furthermore, the prognosis of DVT is not good. As the research showed that 50% of UEDVT may proceed to be post-thrombotic syndrome (PTS). 1 And the possibility of death risk of PE also needs to be noticed.
In this case, some factors may contribute to the venous thrombus process. First, the operator did not perform the brachial puncture under the guidance of duplex ultrasound; therefore, the intragenic injury may be the most important reason for the complication. Second, the compression bandage was used after surgery which may promote the formation of thrombus, even though routine heparinizing is kept during and after surgery. Third, the patient may not be sensitive to the anticoagulation treatment which may promote the pro-thrombotic states during the operation. Thus, as an operator, we need to do more to prevent the happening of venous thrombus complicated by puncture site. For example, because of the high anatomical varieties, duplex ultrasound guided puncture reduces the risk of access site complications. On other hand, some vascular closure devices11,12 can be used to prevent the long time pressure on the vein which may influence the hemodynamics and also can reduce the bleeding after removing the catheter. Last but not the least, for the patients with heparinizing, activated clotting time (ACT) levels could be monitored (our target ACT is ⩾300 s). 4 The level can be checked every 30 min during the surgery.
With respect of the treatment of UEVT, different causes have different treatments; there is no standard therapy for the UEVT following brachial artery puncture; however, the research showed that patient who had a major thromboembolic event without anticoagulants would face a very high risk of DVT/PE recurrence during the acute phase, and thus, the antithrombotic therapy is necessary. 13 And the research of catheter-related UEDVT showed that anticoagulation without thrombolysis for 3 to 6 months was safe and efficiency. In this case, we took anticoagulation treatment only; on one hand, because the patient just undergone the operation, thrombolysis treatment may induce the uncontrolled bleeding which may danger the patient’s life or local hematomas; the later condition may increase the pressure of upper arm which may induce osteofascial compartment syndrome. With the consideration of the slightly symptom, neither consequence mentioned above can pay off the efficiency of thrombolysis. Therefore, anticoagulation treatment without thrombolysis was chosen. Besides the medical treatment, some physical exercises, such as lift the arm or handgrip exercise, were used to promote the hemodynamics of vena. Whether filter is needed or not is not sure. For this patient, long-term following is needed. Once the following complications like PE or DVT are found, early find and treatment in time is necessary.
Conclusion
Superficial or deep venous thrombosis after brachial artery access for peripheral interventions represents a rare but not less important issue which could be associated with thromboembolic complications. Ultrasound guided puncture should be performed to reduce the risk of this complication.
Footnotes
Acknowledgements
Thanks for Dr Tao Zheng who provides the case.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author’s Note
There is no prior presentation.