
Abstract
Arteria lusoria is a rare vascular aberration; its presence is frequently associated with dysphagia or dyspnea due to esophageal or bronchial compression. We present a case of a stenotic arteria lusoria causing upper extremities blood pressure difference, claudication, and Raynaud’s syndrome of the right hand. The patient opted against endovascular recanalization and was treated conservatively. This case demonstrates a rare cause of upper extremity blood pressure difference that must be considered as differential diagnosis. Furthermore, the knowledge of arteria lusoria is pivotal for successful transbrachial coronary or peripheral endovascular interventions.
Background
Arteria lusoria is an aberrant right subclavian artery leaving the aortic arch as last major branch and crossing between the esophagus and the vertebral column to the right side (Figure 1). Its prevalence varied between 0.05% and 2.3%. 2 The presence of arteria lusoria is frequently associated with dysphagia 3 , 4 and dyspnea 5 due to arterial compression of the esophagus or trachea. A recent literature search revealed no cases of blood pressure differences nor claudication of upper limbs caused by a stenotic arteria lusoria.

Simplified scheme of thoracic situs including arteria lusoria. 1
Clinical Case
A 78-year-old Caucasian female patient presented 2016 with a systolic blood pressure difference of the brachial arteries of 40 mmHg, cold sensations of the right hand, Raynaud’s phenomenon of the right fingers (Dig. II-V) and claudication of right forearm. Her medical history revealed a single episode of vasovagal syncope, hypertensive chronic renal disease, and arterial hypertension. Dysphagia and upper extremity sensory deficits were denied. Laboratory findings showed only dyslipidemia.
The initial computed tomography (CT) scan (Figure 2 to 4) showed at least 75% stenosis of the proximal arteria lusoria. The cerebral blood supply was independent of it and therefore not restricted. Additional tests confirmed Raynaud’s syndrome of stenotic origin.

3D reconstruction of heart and main vessels, arrow indicating arteria lusoria.
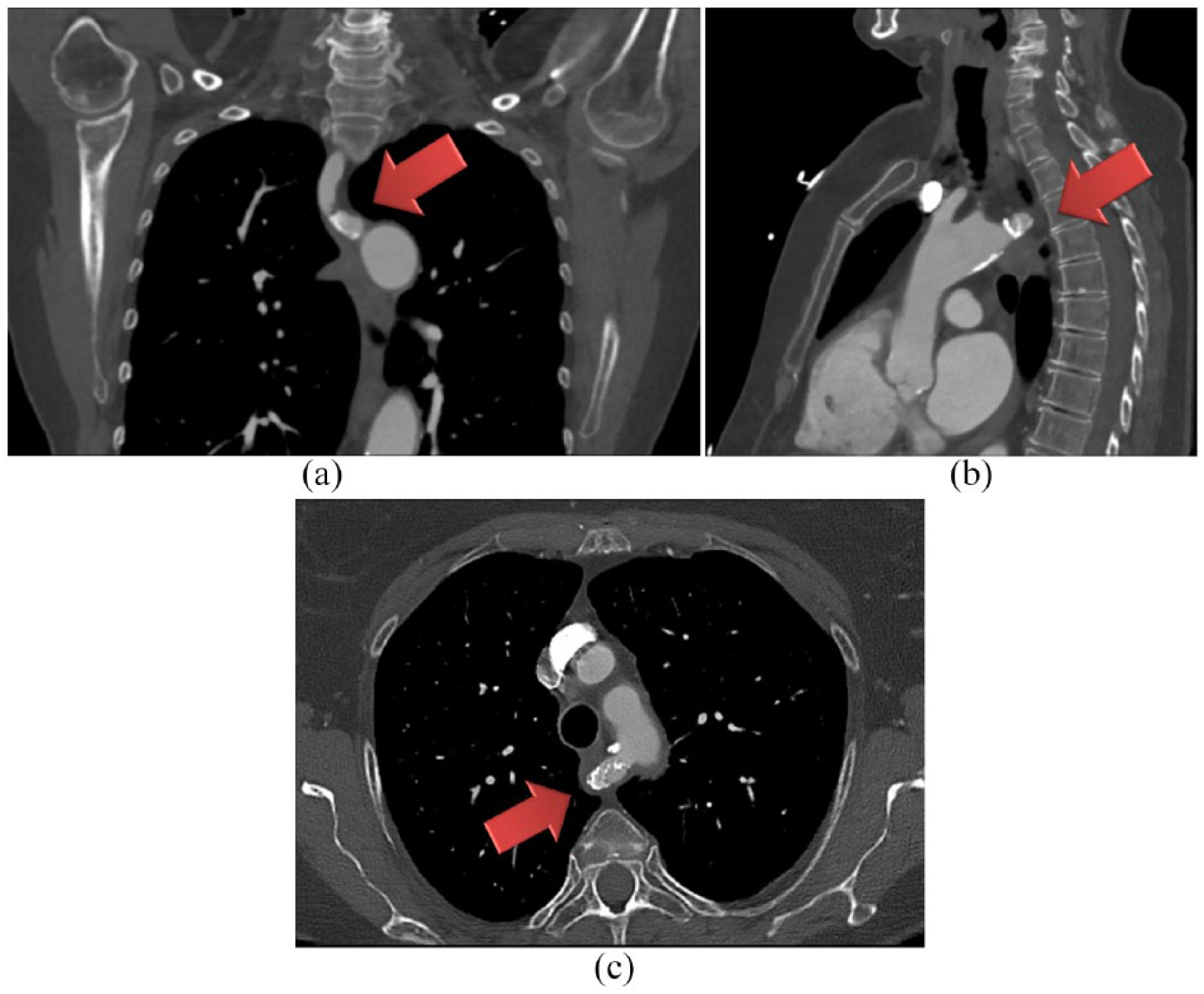
Computed tomography angiography (CTA SOMATOM Definition Flash) thoracic scan, arrow indicating arteria lusoria. (A) coronal image, (B) sagittal image, and (C) transversal image.

2D reconstruction of arteria lusoria.
The patient opted against endovascular recanalization and for conservative management instead. Accordingly, we recommended to modify cardiovascular risk factors, and the patient was placed on primary prevention with a statin (pravastatin 40 mg QD) and antiplatelet therapy (aspirin 100 mg QD). Raynaud’s syndrome was symptomatically treated with amlodipine 5 mg QD.
The follow-up CT scan 1 year after diagnosis showed a stable finding of the stenosis. The patient reported persistent slight weakness of the right hand, however, with regression of Raynaud’s signs. No additional symptoms were presented.
Conclusions
This case demonstrates a rare cause of upper extremity blood pressure difference that must be considered as differential diagnosis. Furthermore, knowledge of an anatomic variant in the form of an arteria lusoria is pivotal for successful transbrachial coronary or peripheral endovascular interventions. Providing informed consent, our patient agreed for publishing her deidentified data.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
AT and MS wrote the article, chose the pictures. IB edited and approved the draft.