
Abstract
Aggressive digital papillary adenocarcinoma (ADPA) is a rare tumour of eccrine origin. They present as asymptomatic nodules with flattened and thickened surface skin, most commonly on fingers and toes. It mimics many benign entities and tumours, hence leading to a delay in diagnosis. It has a high metastasizing potential, but is slowly progressive. Histopathologically, it has both a nodular and a cystic component with papillary projections into cystic spaces. We present a 54-year man with a tumorous mass on right heel, which was diagnosed by histopathology and immunohistochemistry as ADPA. Our case had ADPA lesion, a rarely reported malignancy on an uncommon site with distant metastasis.
Keywords
Introduction
Aggressive digital papillary adenocarcinoma (ADPA) is a malignancy of eccrine gland. Helwig, in 1979, first described it as ‘eccrine acrospiroma’. 1 After a decade, the term ‘aggressive digital papillary adenocarcinoma’ was introduced by Duke et al 2 for this tumour. Aggressive digital as the name suggests is a malignancy that has a metastatic potential with a tendency to recur and is commonly located over digits. We describe a 54-year man with a growth on the heel, which was proven, by histopathology and immunohistochemistry, to be ADPA.
Case Presentation
A 54-year Indian man presented with solitary painless mass on the right heel for last 2 years, which was progressively increasing in size. There was no history of trauma or manipulation with a thorn. There was no history of any other systemic complaint. On cutaneous examination, there was an exophytic tumorous mass of size 2.0 cm × 2.0 cm with ulceration and crust in the centre (Figure 1). The margins were hyperkeratotic posteriorly. Systemic examination was normal. With a clinical suspicion of foreign-body granuloma, adnexal tumour, or squamous cell carcinoma, a wedge biopsy was sent.

Ulcerative nodular lesion on right heel.
Investigations
Routine haematological and biochemical reports were within normal limits. Radiological examination of chest showed multiple cannon ball secondaries (Figure 2). Ultrasound abdomen and head computed tomography (CT) were within normal limits. Right foot magnetic resonance imaging (MRI) showed a mass lesion in the plantar aspect of right heel, which was slightly exophytic and nodular measuring 1.8 cm × 1.9 cm in subcutaneous plane (Figure 3). This was markedly hyperintense on short tau inversion recovery (STIR), hyperintense on T2 weighted image (T2WI), and hypointense on T1 weighted image (T1WI). There was no muscle or bony involvement. Histopathologic examination showed hyperkeratosis and acanthosis of overlying squamous epithelium. Dermis showed variable-sized nodules without any connection to epidermis. These nodules showed syncytial and cribriform patterns along with papillae lined by mildly pleomorphic cuboidal-to-columnar cells with scattered mitosis (Figures 4 and 5). Based on histopathology, diagnosis of ADPA was suggested. Immunohistochemistry showed positivity for cytokeratin (CK) and epithelial membrane antigen (EMA). Basal cells were immunoreactive for p63 and S-100. Ki-67 index was 8% to 10%.

Chest X-ray showing canon ball secondaries.

MRI showing nodular exophytic growth right heel with no musculoskeletal invasion. MRI indicates magnetic resonance imaging.
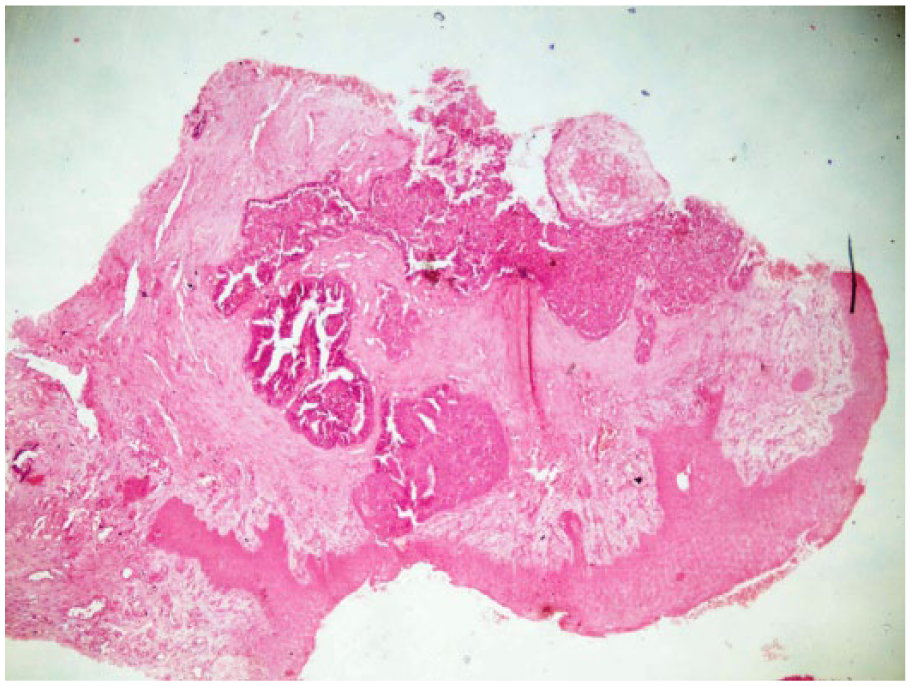
(H&E 40×) Nodules with syncytial and cribriform pattern along with papillae lying within dermis not attached to epidermis.

(H&E 100×) Nodules with syncytial and cribriform pattern along with papillae lined by columnar cells (H&E 400×) inset showing cribriform pattern of cuboidal and columnar cells.
Differential Diagnosis
Based on histopathologic and immunohistochemistry findings, diagnosis of ADPA was made. Eccrine adenocarcinoma was ruled out because of papillary projections that are seen in ADPA, but not in eccrine adenocarcinoma, although immunohistochemistry may be common in both.
Treatment
Amputation (so as to reduce the tumour load) was planned, but patient refused for any operative interference, so the patient was referred for chemoradiotherapy.
Discussion
Sweat gland carcinomas are rare malignant tumours of skin. ADPA are tumours of sweat gland. ADPA and adenoma were described as distinct entities initially, but later thought to be indistinct clinically, by progression and histologically. 2 In spite of the metastatic potential (14%-22%) and high rate of recurrences (50%), the tumour is slowly progressive and is thought to be a low-grade malignancy. 3 There is a delay between onset of disease and diagnosis of 10 to 30 years. 4 Suchak et al 5 and Chen and Asgari 6 suggested removal of nomenclature aggressive from ADPA because of its slow progression. ADPA has no specific morphological features, hence is very rarely suspected clinically. This tumour is more common in men (with men:women ratio of 9:1), usually seen in fifth to seventh decade. 7
There are only 3 case series and individual case reports of ADPA with a total of less than 170 cases reported till date. They present as painless nodules with flat and thickened overlying skin less than 2 cm in size. Very rarely, they may be painful. About 80% ADPA have been reported on fingers with 5% arising on hands elsewhere. 4 On the fingers, they usually arise between the nail bed and distal interphalangeal joint. 8 Atypical sites are reported on the thigh, scalp, lower leg, web-spaces of the hands and feet, lips, and ears. 9 On the foot, most of the lesions are seen on toes, and no case has been reported over the heel. The presentation of ADPA at these atypical sites warrants a deletion in the word digital in ADPA. Also, the tumour being of eccrine origin, there is no definite reason why these lesions cannot be located anywhere else on the body.
ADPA mimics many benign tumours and non-tumorous entities, hence is rarely suspected clinically leading to delay in diagnosis. Histopathology of the lesion shows hyperkeratosis and acanthosis in epidermis. Dermis shows a grenz zone with nodules and cysts in epidermis showing papillary projections lined by cuboidal cells and arranged in syncytial cribriform pattern with scattered mitosis. There are few cases of ADPA described without cysts also. Histopathologic differentials of ADPA are hidradenoma, apocrine cystadenoma, apocrine adenoma, tubular apocrine adenoma, spiradenocarcinoma (eccrine acrospiroma), eccrine adenocarcinoma, papillary eccrine adenoma, and metastatic adenocarcinoma. Metastasis will have clinical and histomorphic features suggestive of primary malignancy. Also, p63 positivity suggests a primary adnexal tumour. Apocrine tumours have apocrine differentiation. Hidradenoma has nodules of clear and polyhedral cells with scattered squamoid foci. Spiradenocarcinoma arises from spiradenoma, so transitional zones of benign and malignant zones are seen. Eccrine tumours may show similar immunohistochemistry, but the nodules with papillae projecting into cystic spaces and cribriform pattern are characteristic of ADPA. 10 ADPA shows CK and EMA positivity, which supports its eccrine origin, although few authors have suggested an apocrine origin also. Ki-67 index is usually less (8%-10% in our case), which suggests that ADPA is a low-grade malignancy.
Metastasis may be by haematogenous or lymphatic route. Lung tissue is the commonest site for metastasis (seen in 71% of total metastasis), with other sites being lymph nodes, brain, skin, bones, and kidneys. 11 Cannon ball secondaries, which were asymptomatic, were seen in our case. There are no clinical or histopathologic features that can predict the chances of recurrence or metastasis.
Wide excision or amputation of the part is the treatment of choice. Inadequate excision leads to recurrence.2,12 Benefits of chemotherapy and radiotherapy have been variable. 12 As metastasis can be seen even after wide excision or amputation even after 20 years, a regular and long-term follow-up is required. 13 Hormone therapy has been suggested for metastatic disease. 4
Take-Home Messages
ADPA is a slow-growing painless malignancy of eccrine glands;
Clinically may present as slowly progressive nodules on digits;
Histology shows nodular and cystic areas with papillary growth into cyst and mitotic figures;
Digits are not the exclusive sites involved;
Pulmonary metastasis is quite common.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
JG edited and designed, AnG design and literature search, MG literature search and edited, AG literature search and intellectual content.