
Abstract
Aims:
Renovascular hypertension is a rare cause of paediatric hypertension. It is however, a potentially treatable cause particularly when caused by renal artery stenosis (RAS).
Materials and Methods:
We present the case of an 11-month-old girl presenting with cardiac dysfunction. She was found to be hypertensive with a systolic blood pressure >180mmHg. DMSA demonstrated a small right kidney and a divided renal function of 6% on the right and 94% on the left. Spectral analysis demonstrated abnormal waveforms suggestive of RAS of the left kidney.
Results:
Angioplasty with a cutting balloon was successful. Blood pressure measurements, renal function and left ventricular function improved.
Conclusion:
RAS can be successfully treated with cutting balloon angioplasty after failure of convention balloon angioplasty to relieve the narrowing. In our case, there was an immediate successful angiographic result that on mid-term follow-up demonstrated significant improvement in clinical and biochemical outcomes and cessation of all anti-hypertensive medication.
Introduction
Although hypertension is rare in the paediatric population, renal artery stenosis (RAS) is the most common renovascular cause. 1 Despite RAS being difficult to diagnose in children, it is potentially treatable. It is most commonly encountered with fibromuscular dystrophy, neurofibromatosis, vascular malformation, Moyamoya disease, Takayasu arteritis, and, rarely, atherosclerosis.2,3
The treatment options for RAS include open surgery and percutaneous transluminal angioplasty (PTA).4,5 The latter may be performed with minimal complications, under local anaesthesia (with the exception of the paediatric population) and with minimal invasion. Percutaneous transluminal angioplasty typically uses a conventional balloon for revascularisation. Surgery is reserved for cases of RAS that are resistant to PTA. More recent advances, however, incorporate balloons with cutting technology that aim not just to tear the vessel wall but to incise the wall, reducing elastic recoil and improving outcomes both in the short and long term.6–8
In the present report, we describe a case of RAS, of unknown aetiology, that was resistant to medical management and conventional balloon angioplasty, which was successfully treated with cutting balloon angioplasty.
Case Presentation
A previously healthy 11-month-old girl presented with failure to thrive and dyspnoea secondary to cardiac dysfunction. She was found to be hypertensive. Blood pressure measurements demonstrated a persistent systolic pressure over 180 mm Hg. She was initiated on antihypertensive and diuretic medication. There was no family history of significance and no stigmata of autoimmune disease or neurofibromatosis. There was no syndromic phenotype. Biochemistry revealed marginally renal function (creatinine 25 mmol/L), but urinalysis was normal. Vasculitic screen was negative. Echocardiogram revealed left ventricular dysfunction and hypertrophy. Renal Doppler ultrasound demonstrated a reduced blood flow through a comparatively smaller right kidney (1 SD below mean) with abnormal spectral trace in the right renal artery. Divided renal function was estimated at 30% on the right and 70% on the left. No dysplastic changes were seen. Dimercaptosuccinic acid (DMSA) demonstrated a small right kidney and a divided renal function of 6% on the right and 94% on the left.
At this time, the patient was referred to our tertiary centre for a review at a multidisciplinary team (MDT) meeting to consider angioplasty versus nephrectomy as a treatment. The tests had not at this point identified any pathology in the left kidney (which DMSA had demonstrated to contribute to 94% of renal function), renal function was only slightly deranged, and bilateral RAS was thought to be usual. The decision was made to perform a right nephrectomy in the belief that the poorly functioning right kidney, and associated reduced renal perfusion, was driving a compensatory hypertensive response via the renin-angiotensin system. This was confirmed on biochemical assay of renin and aldosterone levels. At this point, she was taking 5 different classes of antihypertensive medication and the DMSA had shown only 6% function from the right kidney.
The nephrectomy was performed and the resected right kidney demonstrated no histological abnormality such as fibromuscular dysplasia (FMD). There was compensatory hypertrophy of the left kidney on follow-up ultrasound (>2 SDs above the mean), but the hypertension persisted and the marginally impaired renal function did not improve (thought due, in part, to the Angiotensin converting enzyme (ACE) inhibitor). Spectral analysis demonstrated abnormal waveforms suggestive of RAS of the solitary left kidney. Following further MDT meeting discussion, it was decided to attempt angioplasty of the left renal artery.
Percutaneous transluminal angioplasty was performed via a 4Fr vascular sheath in the right common femoral artery. Angiogram demonstrated no aortic coarctation but a tight ostial stenosis of the left renal artery (Figure 1) suggestive of possible unifocal FMD. The stenosis was crossed and angioplastied with both 2 and 3 mm conventional balloons (Sterling, Boston Scientific, Massachusetts, United States), but there was failure to relieve the stenosis (Figure 2) despite high inflation pressures. As the use of a cutting balloon and its inherent risk had not been discussed or consented for the decision was made to stop and the use of a cutting balloon discussed in the paediatric urology meeting. A second attempt was scheduled for 3 months later. The MDT decision was to have a renal transplant surgeon available during PTA so that, should a complication, such as dissection, arise with loss of the solitary kidney, then the kidney could be auto transplanted and re-anastomosed in the pelvis. Using a 6Fr sheath, an over-the-wire 3 mm × 15 mm cutting balloon (Boston Scientific) was used over a 0.014 wire (Figure 3) to relieve the stenosis. The stenosis was post dilated with 3.5 mm × 20 mm balloon with excellent angiographic results and release of the stenosis (Figure 4). There were no immediate complications.

Angiogram demonstrating the tight left renal artery stenosis.

Plain balloon angioplasty failing to relieve the stenosis.
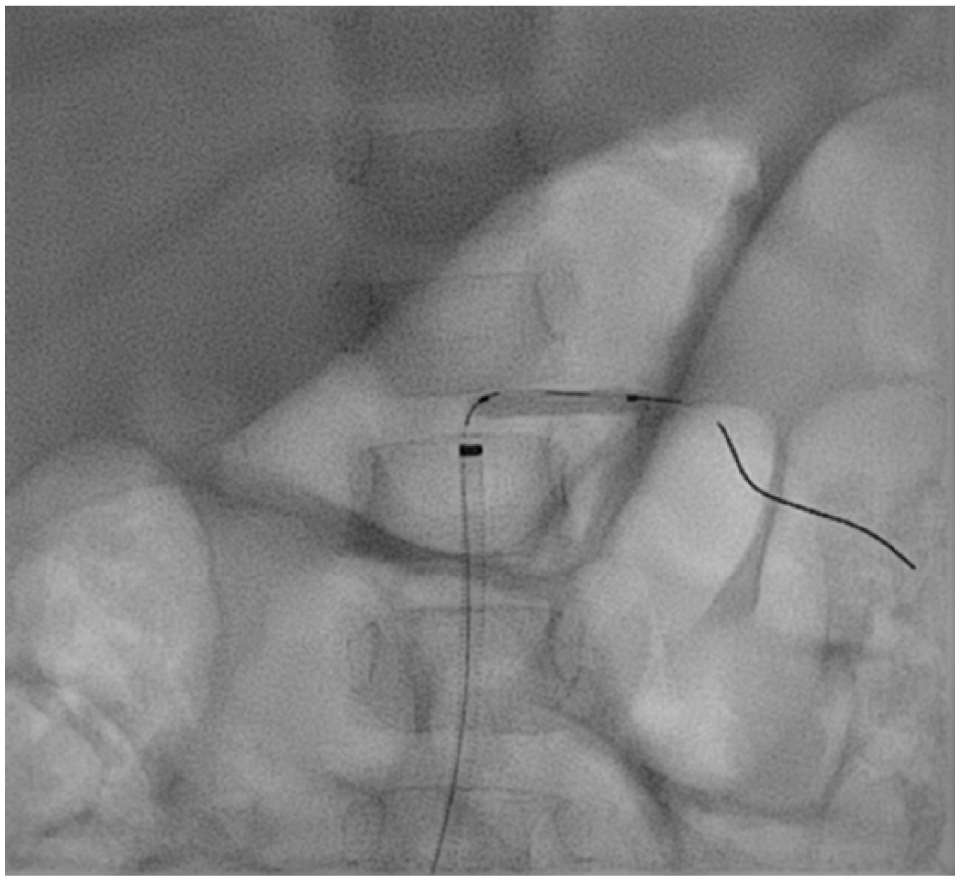
Cutting balloon angioplasty successfully relieving the stenosis.

Post-procedure angiogram.
During the month following cutting balloon angioplasty, there was an improvement in blood pressure and antihypertensive medications were slowly weaned off. Three months following treatment, she had stopped 2 antihypertensives and 1 was reduced, leaving her taking 2 antihypertensives. The parents reported increased wet nappies, thought perhaps due to increased renal perfusion. Echocardiogram revealed improved left ventricular function. In addition, the biochemical profile demonstrated an improvement in renal function with a reduction in creatinine. At 1 year of follow-up, she had stopped all antihypertensives and remained with stable good blood pressure and normalised end-organ function.
Discussion
We present a case of resistant RAS causing renovascular hypertension in a paediatric patient. While not uncommon in the adult population, it is infrequently described in the paediatric literature. It is seldom described in a solitary paediatric kidney, following contralateral nephrectomy, with the associated risks of complications of PTA causing potential renal loss.
Paediatric patients with RAS may be asymptomatic or, as in our case, present with nonspecific symptoms secondary to end-organ injury. The cause for our case reports RAS remains unknown. Although FMD is the most common cause of paediatric RAS, the case we present had no features to suggest that this was the underlying aetiology in the resected right kidney although imaging findings in the right kidney would be in keeping with unifocal FMD.
After a short period of follow-up, cutting balloon PTA produced an excellent clinical outcome. Other authors have described similar success in treating paediatric RAS. Shroff et al 5 examined 33 cases of paediatric (median age of 10.3 years) renovascular hypertension treated with PTA ± stenting. Clinical improvement was seen in 50% of patients; however, high rates of restenosis were encountered in patients treated with stents (36.8%). The same group later reported a further series in 78 children (median age of 6.5 years) and demonstrated improved hypertension in 62.8%. This was most pronounced in RAS effecting only the main renal artery (the cohort also comprised children with intrarenal stenosis, mid-aortic syndrome, and coexisting cerebrovascular disease). 9
The youngest child treated for RAS is an 8-day-old baby described in a case report by Daehnert and colleagues who successfully performed PTA using a 2 mm × 10 mm balloon . 10 There was no recurrence on Doppler sonographer at 8 months of follow-up.
Our case report documents only a midterm period of follow-up, and the literature suggests that re-intervention rates are high for RAS.9,11–13 Frequently, stents have been used due to poor long-term results of PTA and are recommended for severe or difficult ostial and restenotic lesions.5,14,15 While most authors report the use of bare-metal stents, there are cases of drug-eluting stent (DES) use with good results on 6 months of follow-up. 16 There is, however, a paucity of data for the use of DES outside the coronary system. The concerns of using stents in the paediatric cohort relate to the renal artery diameter increasing over time and the stent may fracture or reocclude at which point salvage is often only possible surgically. We anticipate that the child in our case report will require further PTA in the future for recurrent disease. There is currently no consensus on the best method of follow-up for recurrence; however, we plan to measure renal function biochemically quarterly in the short term.
Conclusion
We present a unique case of paediatric RAS causing symptomatic renovascular hypertension. The stenosis was successfully treated with cutting balloon PTA after failure of convention balloon angioplasty to relieve the narrowing. There was an immediate successful angiographic result that, on midterm follow-up, demonstrated significant improvement in clinical and biochemical outcomes and complete cessation of antihypertensive medication.
Footnotes
Acknowledgements
The case was presented as a poster presentation at Cardiovascular and Interventional Radiological Society of Europe (CIRSE) Annual Congress 2018 in Lisbon.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
TCH was responsible for writing the manuscript. AW, FH and RON all provided critical appraisal and assistance in writing the completed manuscript.
Consent Statement
We confirm that full written consent has been obtained by the patients’ parents both for the publication of the report and for the procedure undertaken.