
Abstract
Long term outcomes following coronary artery bypass grafting are governed by patency of vascular grafts. In this regard, the use of arterial grafts, (preferably the left internal mammary artery) has demonstrated improved survival relative to their venous counterparts. These benefits are a consequence of greater patency of LIMA at 10 years vis-a-vis venous grafts. Uncommonly, there is a possibility of occlusion of LIMA early in the post operative period due to procedural reasons but late occlusion of LIMA is rare. We report an unusual case of late occlusion of LIMA after seven years of CABG.
Introduction
The long-term outcomes after coronary artery bypass grafting (CABG) are dependent on the patency of the arterial and venous grafts. Internal mammary artery (IMA) grafts have shown greater long-term patency rates and improved survival than saphenous vein grafts (SVGs). Acute occlusion of the left internal mammary artery (LIMA) with patent venous grafts causing acute coronary syndrome (ACS) in the late postoperative period is rare.
Case Report
A 59-year-old diabetic and hypertensive male patient presented to our department with acute onset chest pain radiating to the left arm. His blood pressure was 110/70 mmHg, pulse rate was 68 beats/min, the respiratory rate was 16 breaths/min, and oxygen saturation was 99% on room air. His 12-lead electrocardiography revealed QS complexes in the inferior leads (Figure 1). Two-dimensional echocardiography showed the absence of regional wall abnormality of the left ventricle and normal valvular function. His high-sensitivity troponin T (Elecsys Assay, Roche diagnostics, MA) level was 5.16 ng/mL (N < 0.014 ng/mL). The patient had undergone CABG 7 years back in another hospital for stable angina. One arterial graft, that is, LIMA to left anterior descending (LAD) artery and two venous grafts, one each to the first obtuse marginal (OM1) and the posterior descending artery (PDA) were implanted at that time. His previous left ventricular ejection fraction was also normal. He was doing well on guideline-directed medical therapy since then. He was compliant to drugs. His blood sugar levels were under control with oral hypoglycemic agents. His estimated glomerular filtration rate (eGFR) by the Modification of Diet in Renal Disease (MDRD) equation was 65.87 mL/min/1.73 m2. Other hematological and biochemical parameters were within normal range.
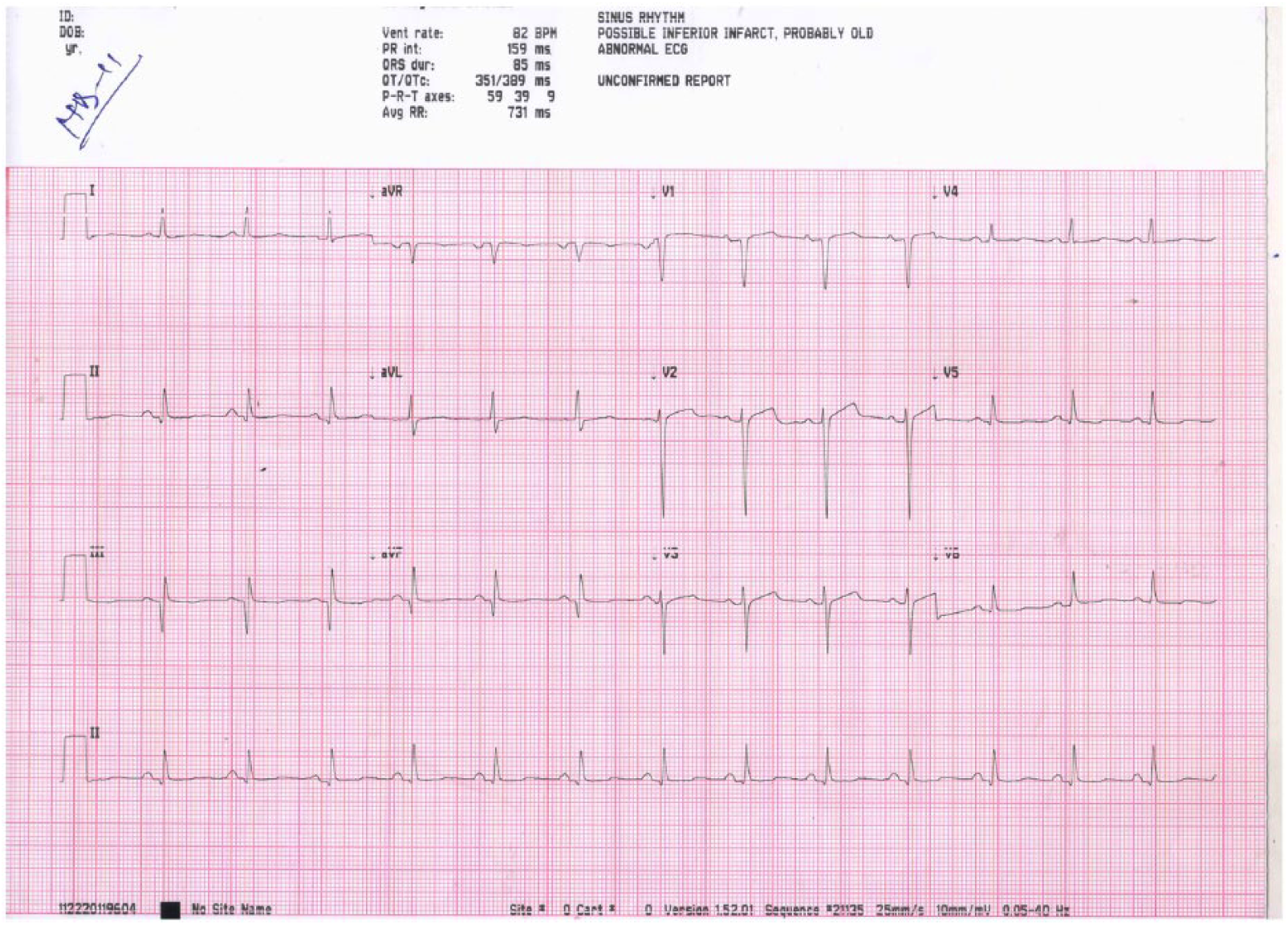
A 12-lead electrocardiogram showing QS complexes in inferior leads.
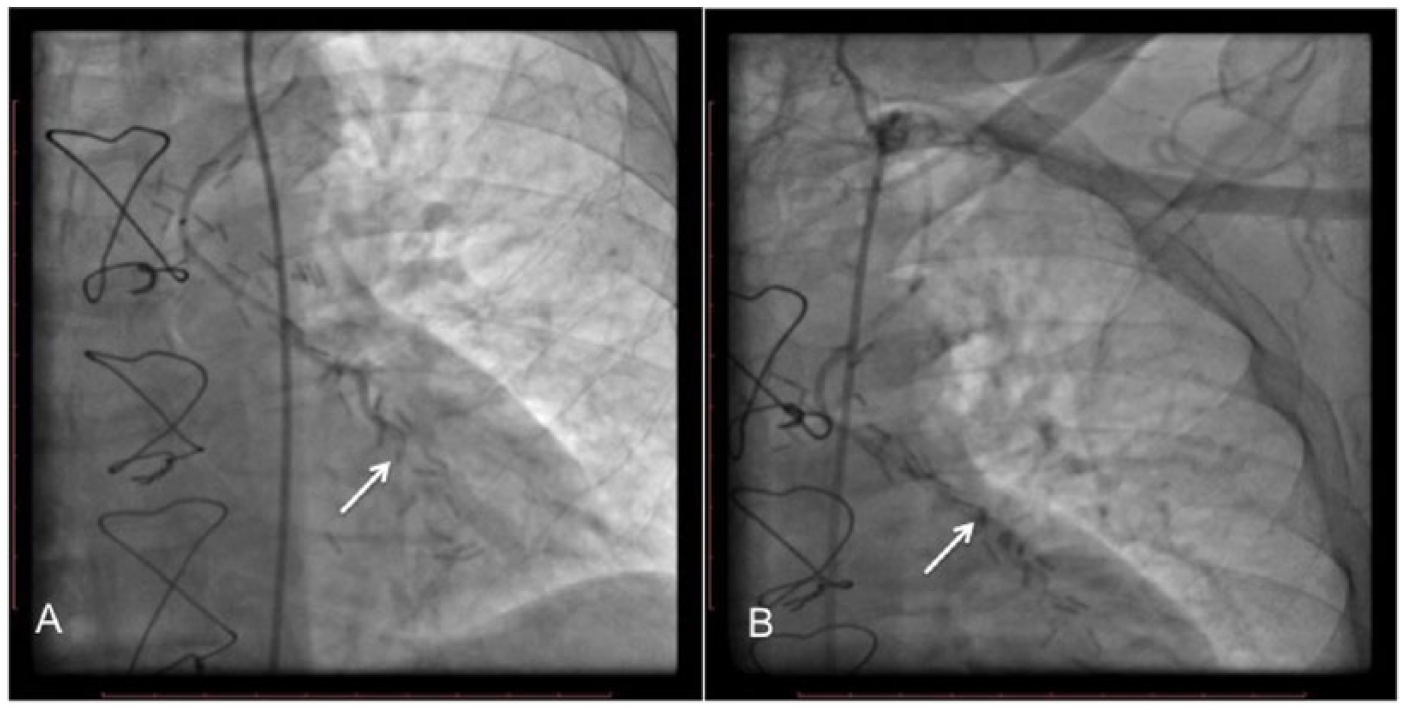
He was taken up for coronary angiogram with an intention to revascularize. His native coronary angiogram revealed severe triple vessel disease with total occlusion of the right coronary artery in mid part (Figure 2A and B). To our surprise, both venous grafts were patent (Figure 3A and B). To our dismay, LIMA graft to LAD graft was 100% occluded proximal to distal anastomotic site (Figure 4A and B). Therefore, we considered LIMA graft as the culprit lesion and decided to intervene. However, the patient refused any intervention and opted for medical therapy. During his hospital stay, he demonstrated hemodynamic stability and pain-free status for the next 72 hours. He was discharged on dual antiplatelet (aspirin plus ticagrelor) regimen supplemented by other drugs for secondary prevention after myocardial infarction as directed by the guidelines. At first and second follow ups at 15 days and 1 month thereafter, he was symptom free on optimal medical therapy.

(A) Native vessel angiogram showing severe disease (near total occlusion) of left coronary system and (B) total occlusion of right coronary artery (RCA) in the mid part.

Selective graft angiogram showing patency of both saphenous venous grafts (arrows) to (A) right coronary artery (RCA) and (B) obtuse marginal (OM).
Discussion
Coronary artery bypass grafting surgery is the treatment of choice for coronary artery disease (CAD) patients with multi-vessel disease and diabetes, left ventricular dysfunction as well as involvement of left main coronary artery (LMCA). 1 The majority of these patients receive IMA grafts to the LAD coronary artery and SVGs or other conduits to the remaining vessels. The benefit of IMAs over SVGs on mortality has been consistently demonstrated.1,2 The main differences in outcomes are related to the development of atherosclerosis which has rarely been observed in the IMA graft, while it develops at a fairly rapid rate in the SVG.1,2
In 1986, Loop et al studied the 10-year survival of patients who received an IMA graft to the LAD with or without one or more vein grafts versus patients who received only SVGs. They demonstrated that the survival was higher with an IMA graft (93.4%) versus SVG (88.0%) for those with one-vessel disease, 90.0% versus 79.5% for two-vessel disease, and 82.6% versus 71.0% for those with disease in three-vessels. Saphenous vein grafts are known to undergo early atherosclerosis, and angiographic studies demonstrated a 2% per year occlusion rate from the first to the seventh postoperative year, further increasing to 5% per year from the 7th to the 12th year. 3
Results from a Department of Veterans Affairs Cooperative study showed that patency at 10 years was 61% for SVGs compared with 85% for IMA grafts (P < 0.001). 4
The mechanisms responsible for rapid neointimal proliferation in SVGs are considered to involve response to endothelial injury along with hemodynamic stress as the vein is now subjected to arterial pressures. 3 The superiority of IMAs over SVGs with less mortality and greater patency rates could be attributed to the resistance of IMA to atheroma. The endothelial layer of the LIMA generally has fewer fenestrations, lower intercellular junction permeability, large amounts of anti-thrombotic molecules like heparin sulfate and tissue plasminogen activator, and higher production of endothelial nitric oxide. These features prevent atherosclerotic changes in the LIMA. 5
Uncommonly, ischemic events can occur due to lesion of an IMA graft. Various mechanisms have been explained in literature for this. This may occur due to the development of significant atheroma in the grafted native vessel distal to the anastomotic site. Less commonly, stenosis occurs within the IMA, usually at the distal anastomosis, as a result of intimal hyperplasia, procedural errors, or rarely, atherosclerotic changes. Performing an IMA bypass on a low-grade LAD stenosis or supplying an infarcted LAD territory leads to competitive flow and low flow, respectively, and impairs IMA graft patency. 6
Early IMA graft failure is most commonly attributed to technical errors related to the graft anastomosis. Most LIMA occlusions occur in the early postoperative period and are associated with surgical complications such as hematoma, spasm, dissection, or atherosclerotic lesion at the anastomosis site. 6
Traditionally, the non-invasive evaluation of post-CABG patients has been done by myocardial perfusion imaging. Computed tomography (CT) coronary angiography has emerged as a vital non-invasive diagnostic tool in follow-up of patients following CABG. 7 The venous graft vessels with large diameter and less motion are easier to map. The LIMA grafts can pose a challenge in imaging due to metal clips and small diameters. The native vessels too can be difficult to interpret due to high calcium burden and low caliber of distal vessels seen in chronic CAD. Nevertheless, it has excellent diagnostic performance in this scenario. 8 Recently, certain studies have shown prognostic significance of CT angiography in post-CABG scenario with patients having higher number of unprotected coronary territories on CT showing worse prognosis. 9
The rarity of our case lies in LIMA-LAD graft occlusion 7 years after CABG, with patent venous grafts presenting as ACS. Acute coronary syndrome caused by arterial graft occlusion with patent venous graft is a very uncommon presentation.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
AP and VG were instrumental in drafting the main part of the manuscript. MB and PV provided all the images and legends. RS critically reviewed the draft and finally approved it.