
Abstract
Ovarian cancer often occurs distant metastasis to the peritoneum, liver, lungs, and lymph nodes. However, there has been no reported case of direct metastasis to the duodenal major papilla. We herein reported 72-year-old woman with history of ovarian cancer surgery 11 years ago presenting with obstructive jaundice. Abdominal CT showed a small mass in the distal bile duct. Forceps biopsy from the small mass was done under endoscopic retrograde cholangiography, and histologic examination revealed adenocarcinoma. Pancreaticoduodenectomy was performed and diagnosed immunohistochemically direct metastasis to the papilla from ovarian cancer. The duodenal major papilla is known to be rich in lymph vessels, and these lymph vessels are considered the likely pathway of metastasis in this case.
Introduction
Ovarian cancer is a common malignancy with a high mortality rate, 1 attributed to the frequent occurrence of distant metastasis to the peritoneum, liver, lungs, lymph nodes, and other organs. Almost all intrabiliary tumors that cause obstructive jaundice originate in the biliary duct, although there are reports of rare cases of biliary/papillary metastasis arising from colorectal cancer, breast cancer, lung cancer, malignant melanoma, and other malignancies.2-9 Obstructive jaundice caused by metastatic biliary tract/papillary lesions sometimes occurs because of compression or infiltration of bile ducts due to widespread liver metastases, or in exceptional cases, because of direct metastatic involvement of the extrahepatic bile ducts and duodenal major papilla in the absence of hepatic lesions.7,10,11
We present a case of obstructive jaundice caused by direct metastasis to the duodenal major papilla from ovarian cancer that was treated surgically 11 years ago. This is a very rare case, as no such cases have been documented in the literature.
Case Presentation
A 72-year-old woman presented with abdominal pain. She was diagnosed with ovarian cancer 11 years ago and was treated with neoadjuvant chemotherapy (weekly carboplatin and cyclophosphamide) before undergoing a bilateral salpingo-oophorectomy and hysterectomy. After 2 years of the surgery, a swollen para-aortic lymph node was discovered via computed tomography (CT), and a recurrence of the ovarian cancer was considered. The lymph node was surgically removed, and a peritoneal metastasis was identified during the surgery. The patient was administered postoperative adjuvant chemotherapy (weekly docetaxel and cyclophosphamide), followed by second/third-line chemotherapy (gemcitabine, docetaxel, and nedaplatin) for 9 years after the initial treatment. Thereafter, the patient was followed up with periodic blood tests and imaging examinations (CT or magnetic resonance imaging).
Laboratory tests performed during the first visit to our hospital indicated biliary obstruction: AST (aspartate aminotransferase) 638 IU/L, ALT (alanine aminotransferase) 569 IU/L, ALP (alkaline phosphatase) 1236 IU/L, GGTP (γ-glutamyl transpeptidase) 1632 IU/L, and total bilirubin 1.4 mg/dL. In addition, abdominal ultrasound revealed a dilated intra-extrahepatic bile duct, whereas contrast-enhanced CT showed a small mass in the distal bile duct (Figure 1A) and a peritoneal nodule in the left abdominal cavity (Figure 1B). Endoscopic ultrasound revealed a 13-mm mass in the duodenal major papilla, and endoscopic retrograde cholangiography (ERC) showed a filling defect in the distal bile duct (Figure 2). Subsequently, a fluoroscopy-guided forceps biopsy under ERC was performed, and an endoscopic nasobiliary drainage tube was inserted to obtain a cytological specimen of the bile juice. Pathologic examination revealed adenocarcinoma in both the biopsy specimen and the bile juice. Lower bile ductal carcinoma was diagnosed, and the patient was referred to the department of surgery to undergo subtotal stomach-preserving pancreaticoduodenectomy and peritoneal nodule excision. Pathologic examination revealed that the distal bile duct tumor was a metastatic ovarian carcinoma with peritoneal metastasis. Pathologically, the tumor was an adenocarcinoma with papillary growth and psammoma bodies that closely resembled the histology of the ovarian cancer removed 11 years ago (Figure 3A and B). Examination of the peritoneal nodule revealed the same findings. Immunostaining showed the tumor was cytokeratin (CK) 7 positive, CK20 negative, Wilms tumor 1 (WT-1) positive, cancer antigen 125 (CA-125) positive, estrogen receptor (ER) antibody positive. The tumor showed weak positivity for progesterone receptor antibodies, and these results were compatible with papillary/peritoneal metastasis of the ovarian cancer (Figure 4). Chemotherapy for ovarian cancer was restarted after the surgery, and at the time of writing this report, the treatment was ongoing.
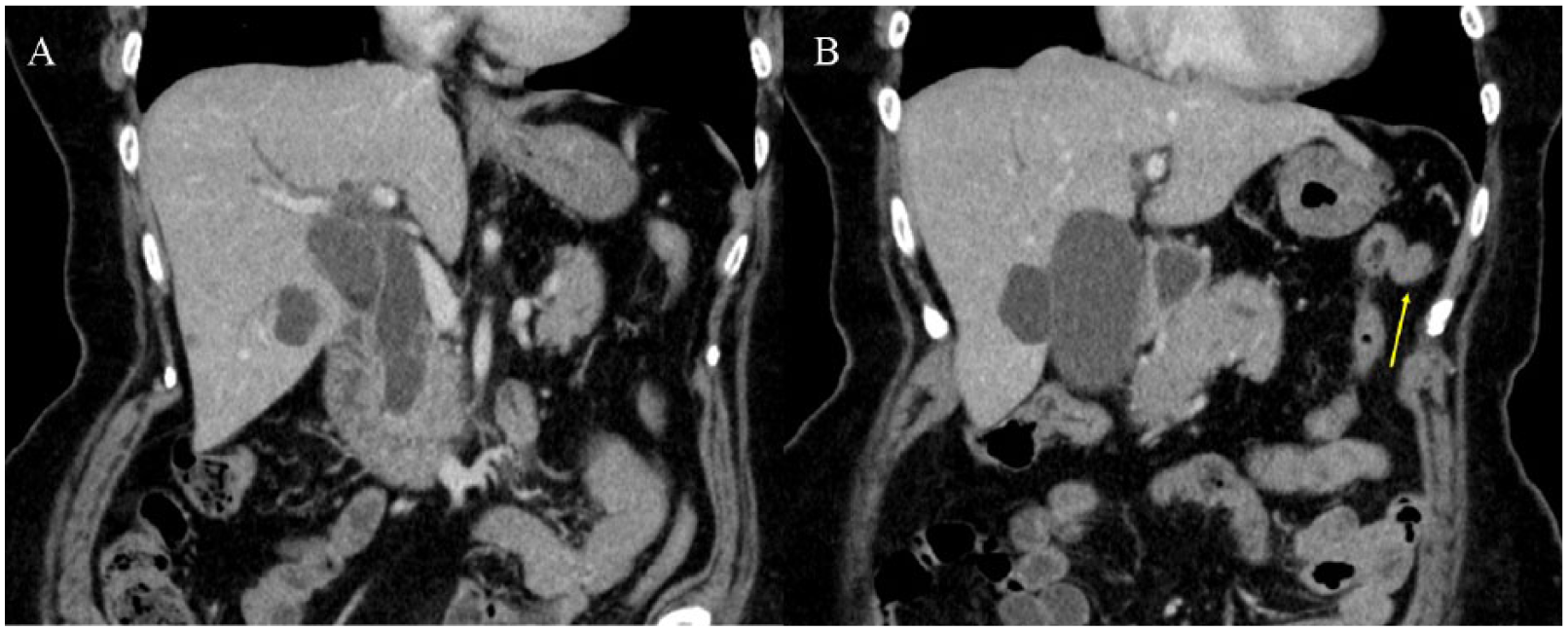
Enhanced computed tomography demonstrated (A) a small high-density mass in the distal common bile duct and dilated common bile duct and (B) a peritoneal nodule in the left abdominal cavity (yellow arrow).

Endoscopic retrograde cholangiography revealed filling defect in the distal common bile duct.

Histologic finding of (A) the tumor in the ampulla of Vater (x400) and (B) primary ovarian cancer (x200). Psammoma body was found in the both findings. Histologic findings of the tumor in the ampulla of Vater closely resemble ovarian cancer resected 11 years ago in hematoxylin-eosin staining.

Immunohistochemical stains of (A) Wilms tumor 1, (B) cancer antigen-125, and (C) estrogen receptor were positive, (D) progesterone receptor were weak positive.
Discussion
Metastatic tumor–induced obstructive jaundice is often caused by liver metastasis, lymph node metastasis, or peritoneal dissemination, and very rarely, by metastasis to the bile duct or papilla. In addition, many reported cases to date stated breast cancer, kidney cancer, or malignant melanoma as the primary lesion.5-9 There is only one reported case of obstructive jaundice caused by ovarian cancer due to extramural pushing/infiltration from lymph node metastasis. 12 To the best of our knowledge, there has been no reported case of obstructive jaundice caused by direct metastasis to the duodenal major papilla. Possible routes of biliary/papilla metastasis are hematogenous metastasis, lymphogenous metastasis, peritoneal dissemination, and direct infiltration from an adjacent organ. In our case, the metastatic pathway is speculated to be lymphatic metastasis because the tumor was principally located in the lumen, and there was no sign of external compression and little venous invasion, whereas pronounced lymphatic invasion in the pathologic specimens was noted. The papilla is known to be rich in lymph vessels, and these lymph vessels are considered the likely pathway of metastasis in this case.
In all cases of metastatic biliary/papillary tumors reported to date, preoperative diagnostic imaging and endoscopically guided biopsy findings have not indicated the likelihood of a metastatic tumor. Based on the literature, these tumors are commonly discovered 2 to 3 years after the diagnosis and treatment of the primary tumor and are difficult to diagnose before surgery. In this case, obstructive jaundice occurred as a result of direct metastasis to the papilla 11 years after surgery for ovarian cancer. Although not the same organ, a few late recurrences were reported.13-15 No definite reason has been determined for this relatively long period of time between primary tumor treatment and metastasis treatment; several theories have been suggested. One of these theories focuses on tumor growth rate and proposes a period of tumor cell dormancy when tumor cells at the metastatic lesion are dormant 16 or grow extremely slow until exposure to some kind of stimulation. 17
In light of the discussion presented, we strongly recommend additional immunostaining of biopsy specimens in the cases of obstructive jaundice caused by biliary/papilla tumor in patients with a history of any kind of cancer. Serous adenocarcinoma is the most common in the ovarian cancer and is histologically characterized by papillary growth, often accompanied by psammoma bodies. Primary ovarian high-grade serous carcinoma (HGSC) cells are strongly immunoreactive for CK7 (almost 100%), whereas CK20 is expressed focally in a minority of cases. The HGSCs are also reported to express the WT1 protein (80%-90%) and ER antibody (76%-95%). 18 Therefore, immunostaining of these proteins would probably be useful for differential diagnosis. Because histologic diagnosis would identify both primary papilla cancer and papilla metastasis of ovarian cancer as adenocarcinomas, immunostaining can be an effective method of reaching an appropriate diagnosis.
Conclusions
We have reported the first case of obstructive jaundice caused by direct metastasis of ovarian cancer to the duodenal major papilla. Although such cases are rare, the possibility of metastatic tumors must be considered alongside primary biliary cancer in patients with obstructive jaundice and a history of malignancy. Immunostaining informed by cancer history can be used to determine the appropriate treatment strategy.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
YT and AI made an equal contribution to this article. GS, AS, YA, AY, NA, TM, YY, RI, SY, and TI participated in manuscript development and care/treatment (including EUS, ERCP, and bile drainage under ERCP) for the patient. NS and TS performed surgical operation and advised the surgical findings, and HH histopathologically examined and advised the pathological findings. All authors reviewed and approved the final manuscript.
Disclosures and Ethics
The authors have read and confirmed their agreement with the ICMJE criteria on authorship and conflict of interest. The authors also confirm that this article is unique and has not been published or is currently under consideration in any other publication.