
Abstract
Hydroxyurea (HU) is a drug frequently used in the treatment of chronic myeloproliferative neoplasms. The most common side effects of this drug are pancytopenia, digestive and skin disorders. Respiratory complications are rare and there are less than 20 cases described, only 5 of which underwent an anatomopathological study. We present the case of a patient with chronic myeloproliferative neoplasm who developed interstitial pneumonitis probably due to HU according to histological study.
Keywords
Introduction
Hydroxyurea (HU) is a drug frequently used in the treatment of chronic myeloproliferative neoplasms. The most common side effects of this drug are pancytopenia, digestive, and skin disorders. Respiratory complications are rare and there are less than 20 cases described, of which only 5 underwent an anatomopathologic study. We present the case of a patient with chronic myeloproliferative neoplasm who developed interstitial pneumonitis probably due to HU according to histologic study.
Case Report
A 68-year-old man (1.78 m in height, 82 kg in weight) without any drug allergies or toxic habits consulted for asthenia and dyspnea of several weeks of evolution. A year earlier, the patient had been diagnosed with an unclassifiable chronic myeloproliferative neoplasm due to the detection of thrombocytosis and leukocytosis in peripheral blood count. It presented a complex karyotype (46, XY, add (1) (q44), (11) (q13q23), (13) (q14) [10]/46, XY [1]) and absence of the mutations JAKV617F, CALR, MPL, and SRSF2. Treatment was started with HU 500 mg/8 h orally. During the following year, the dose was increased to 1500 mg/d orally because of persistent leukocytosis, with a later descent to 1000 mg/d orally because of anemia that required transfusion of 4 units of red blood cells.
The patient consulted for dyspnea with dry cough, asthenia, and low fever of at least 2 weeks of evolution that had been treated with antipyretics (paracetamol 1 g/8 h and eventually ibuprofen 400 mg/8 h). Physical exploration highlighted arterial oxygen saturation (SatO2) of 97%, minimal cracks, absence of respiratory secretions, and sinus rhythm without signs of cardiac failure. Peripheral blood count presented leukocyte count of 56 × 109/L (similar to previous controls), without other alterations. Hemocultures were taken with negative result. Chest x-ray showed multiple bilateral alveoli-interstitial infiltrates. Under the diagnosis of mild respiratory infection, treatment with amoxicillin/clavulanic acid and furosemide was initiated. Due to clinical stability, hospital discharge was decided.
The patient consulted 24 hours later for worsening dyspnea, tremor and fever of 38°C. Physical examination revealed a SatO2 of 77%, temperature of 37.6°C, tachypnea of 45 breaths per minute, bilateral cracks predominating in lower fields, and important intercostal impression. Peripheral blood count revealed a leukocyte count of 71 × 109/L with neutrophilia and left deviation, hemoglobin of 7.8 g/dL, and platelet count of 76 × 109/L. Cultures were taken again, the results of which were also negative. Chest x-ray showed an increase in the alveoli-interstitial infiltrate occupying both lung fields.
Despite broad-spectrum antibiotic treatment (meropenem and amikacin) and ventilatory support with Monaghan mask with FiO2 100%, in the first 24 hours, the patient presented a rapid respiratory worsening, with severe hypoxemia in arterial blood samples (pH 7.42, PCO2 29 mm Hg, PO2 55 mm Hg, HCO3 19 mmol/L), and required admission to the intensive care unit (ICU) for orotracheal intubation and invasive mechanical ventilation.
Once admitted in the ICU, the patient required significant ventilatory support with 70% FiO2 and maneuver of prone position. No changes after intubation were observed with respect to the physical examination or on chest radiography. Urinary antigens of Streptococcus pneumoniae and Legionella pneumophila were negative. The remaining microbiological studies (cytomegalovirus polymerase chain reaction in peripheral blood and the auramine and Ziehl-Neelsen staining as well as the bacteriological and mycological cultures of the bronchial culture and bronchoalveolar lavage [BAL]), taken within the first 48 hours of admission, were negative. Transthoracic cardiac ultrasonography showed a correct ventricular function, without alterations in myocardial contractility, valvulopathies, or alteration of the right cavities. The study of autoimmunity (rheumatoid factor, antinuclear antibodies, and antineutrophil cytoplasm) was also negative.
Once the major infectious, cardiovascular, or autoimmune causes were ruled out approximately the 10th day of admission, and under the suspicion of pharmacologic toxicity, HU was suspended and busulfan treatment (maximum dose 6 mg/24 h orally) was initiated. The antibiotic spectrum was empirically extended with linezolid, co-trimoxazole, ganciclovir, and anidulafungin (removed after the microbiological results) and high-resolution computed tomography (CT) was performed, revealing diffuse alveoli-interstitial infiltrates in both lung fields, hypertrophy of interlobular septum and bronchiectasis, compatible with autoimmune disease or pharmacologic lung injury. With this last diagnostic possibility, a bronchoscopy was performed observing an intra-alveolar hemorrhage; therefore, treatment with glucocorticoids (methylprednisolone 1 g/24 h intravenous for 3 days and maintenance with 50 mg/24 h intravenous) was initiated.
The patient presented a poor clinical course with persistent severe hypoxemia, nonresolution of alveoli-interstitial infiltrates, and increased leukocyte count (reaching a maximum of 205 × 109/L) despite treatment with busulfan at high doses, and finally deceased within 29 days of admission.
A postmortem lung biopsy was authorized for the causal study of respiratory failure. The results revealed areas of patched fibrosis with few fibroblastic nodules, foci of intense intra-alveolar histiocytic infiltrate typical of desquamative pneumonia, and signs of recent intra-alveolar hemorrhage with thrombus and diffuse siderosis (Figure 1). It was not possible to perform the lymphocyte simulation test for drugs because it was not available in our center.

Desquamative pneumonia. Alveolar spaces filled with macrophages with hemosiderin pigment (hematoxylin-eosin, original magnification ×100).
Discussion
Hydroxyurea is a cytoreductor drug widely used in the treatment of chronic myeloproliferative neoplasms that have high thrombotic risk. Hydroxyurea inhibits DNA replication (through inhibition of ribonucleotide reductase) on the S phase of the cell cycle by a mechanism not completely cleared. 1 Its toxicity profile is good and among the most frequent side effects there are hematologic (pancytopenia), digestive (nausea, vomiting, gastritis), or cutaneous toxicities. 2 Otherwise, respiratory complications are uncommon: in literature, only 17 cases of interstitial pneumonitis or acute alveolitis have been described (Table 1). These present in a similar way to the aforementioned case both in symptoms (fever, dry cough, absence of respiratory secretions) and radiological findings (diffuse alveoli-interstitial infiltrates in lung fields) The findings observed in CT show more variability, with the predominance of tarnished glass or panalization patterns, bilateral interstitial infiltrates, and reticulonodular opacities.1-3,5 To our best understanding, only 5 cases with anatomopathologic study compatible with HU pneumonitis have been described in the literature. In these cases, samples were obtained with transbronchial biopsy (1 case), lung biopsy (3 cases), or autopsy (1 case).
Review of literature on the topic.
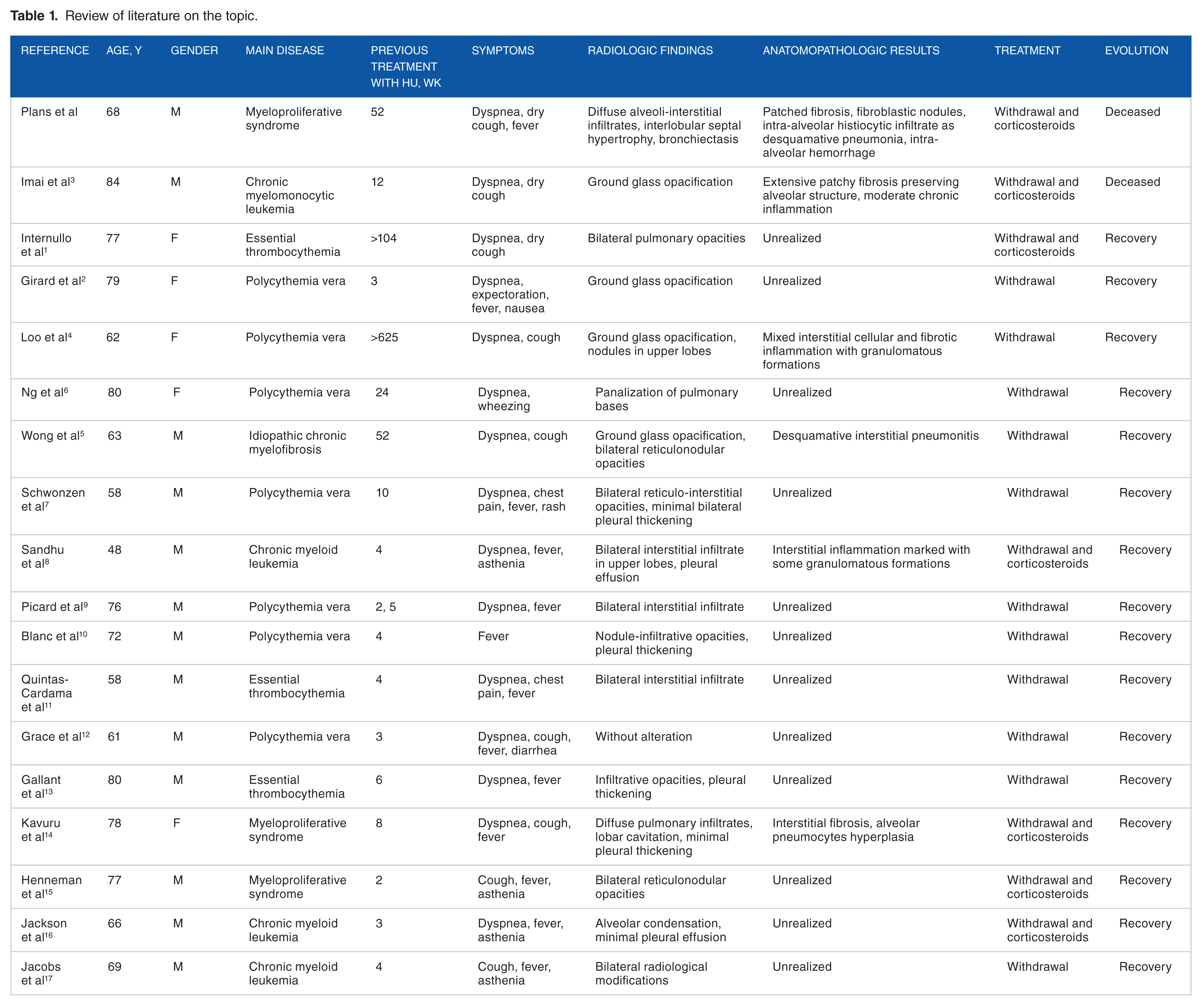
Pulmonary lesions attributable to HU (nonspecific generalized interstitial inflammation, occasional granuloma formation, desquamative pneumonitis patterns, alveolar hemorrhage, pneumocyte hyperplasia, or a mixed pattern of cellular and fibrotic pneumonia) are not specific and can be found in other pulmonary pathologies of pharmacologic origin or other origins; therefore, the anatomopathologic study of lung biopsy is not pathognomonic.
Because it is an uncommon adverse reaction, it is not known which is the best attitude to take, although HU is usually withdrawn initially. It seems possible to reintroduce the drug after the acute phase with correct evolution of the patients. Only 5 cases have been reported in the literature, in which glucocorticoids were associated (daily doses of milligram per kilogram of weight intravenous/orally or bolus of 1 g intravenous/orally) and 1 of them deceased as a consequence of respiratory insufficiency.
In our case, due to the great respiratory instability of the patient and the findings compatible with alveolar hemorrhage, treatment with methylprednisolone 1 g/24 h for 3 days and maintenance with 50 mg/24 h intravenous later was started without success. Viral, bacterial, or fungal infection was never demonstrated in this patient.
Thus, it can be concluded that HU-associated pneumonitis is infrequent, although it may be underdiagnosed because there are few documented cases with histologic study and the anatomopathologic findings are nonspecific and heterogeneous. It is necessary to know better the pathogenesis of this side effect of HU and establish the diagnosis, if necessary with a lung biopsy, as well as the most appropriate treatment. The study of lymphocytes obtained from BAL could facilitate the diagnosis of this entity.
Supplemental Material
Supplementary_Figure – Supplemental material for Hydroxyurea-Induced Pneumopathy in a Patient With Myeloproliferative Syndrome
Supplemental material, Supplementary_Figure for Hydroxyurea-Induced Pneumopathy in a Patient With Myeloproliferative Syndrome by Oriol Plans Galván, Hipólito Pérez Moltó, Ariadna Fabià-Mayans, Blanca Xicoy, José Luis Mate and Pilar Ricart Martí in Clinical Medicine Insights: Case Reports
Supplemental Material
Supplementary_Table – Supplemental material for Hydroxyurea-Induced Pneumopathy in a Patient With Myeloproliferative Syndrome
Supplemental material, Supplementary_Table for Hydroxyurea-Induced Pneumopathy in a Patient With Myeloproliferative Syndrome by Oriol Plans Galván, Hipólito Pérez Moltó, Ariadna Fabià-Mayans, Blanca Xicoy, José Luis Mate and Pilar Ricart Martí in Clinical Medicine Insights: Case Reports
Footnotes
Author Contributions
OPG and HPM treated the patient. OPG wrote the first draft of the manuscript. HPM, AFM, BX, JLM, PRM contributed to the writing of the manuscript. AFM contributed to the translation of the manuscript. BX contributed advising on the hematological pathology. JLM contributed with the images and advising on anatomo-pathological findings. All authors reviewed and approved the final manuscript.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.