
Abstract
Until 2018, 236 cases of acute pancreatitis have been reported in patients who underwent peritoneal dialysis. Here, we presented a patient with double renal transplantation with chronic renal failure, under renal replacement therapy by peritoneal dialysis, who developed acute pancreatitis with abdominal pain, nausea, vomiting, leukocytosis with neutrophil left shift which is complicated by pancreatic pseudocyst, candida peritonitis, fungal sepsis, overlapping of Acinetobacter baumannii sepsis, and pneumonitis. After the percutaneous cystogastrostomy drainage of pancreatic pseudocyst, changes from peritoneal dialysis to hemodialysis, various thoracentesis, and polyantibiotics therapy, the resolution of the sepsis state was seen. The particular aspect of our case is the various comorbidity risks, severe pancreatitis associated with candida and A baumannii sepsis, and treatment strategy that lead to heal this kind of the high mortality rate condition.
Introduction
A search of the current literature was performed using the PubMed database which let us to take 168 articles, analyzing them and adding others from bibliography database, we obtained 236 cases of pancreatitis in peritoneal dialysis (PD) (17 case reports,1–17 5 case series,18–22 11 population-based studies23–33).
In 15 articles it was documented the concomitance of peritonitis, from databases with reached that only 25 from 44 patients had concomitance peritonitis in PD.
Fungal infection is common in patients on PD. Peritonitis is an important complication of the PD; only in some cases the fungal peritonitis is recognized but with 15%-45% of mortality rate. 34
The clinical features of pancreatitis in patients with chronic kidney disease are no different from those in the general population. The only exception is the coexistence of peritonitis and pancreatitis which is clinically difficult to differentiate. 25
The incidence of acute and chronic pancreatitis is increased in PD for the high level of uremic toxin, local hypercalcemia, and toxicity of peritoneal dialysate.2,3 In these patients, the diagnosis is based on the clinical and radiological evaluations because of the altered level of pancreatic enzyme in PD. More often, acute pancreatitis is associated with complete healing without complications, but can complicate to pseudocyst formation in some other cases, which in some condition may require drainage intervention. Until now, there is no specific treatment guideline for pancreatitis in PD, so we handled our case initially with empiric therapy and ensuing according to the dialysis liquid and blood culture results. The peculiarity of this case is represented by numerous morbidities that the patient developed simultaneously, with the genesis of a complex clinical picture, by the combination of infections due to Candida albicans and Acinetobacter baumannii.
Case Report
A 54-year-old woman was hospitalized for abdominal pain, nausea, vomiting, anorexia, and fever, in poor clinical condition, with fever, and unstable hemodynamic state.
Past medical history of the patient is as follows:
Hepatitis C virus positive;
Chronic glomerulonephritis caused by glomerulonephritis of unknown cause in 2002, on hemodialysis from 2007 to 2012, failure of first renal transplantation in 2008 for acute rejection, failure of second transplantation from living donor in 2012 for acute rejection, successive start of hemodialysis, and interrupted after 1 year for vascular access problems. On February 2013, peritoneal dialysis catheter was placed.
Secondary hyperparathyroidism;
Steno-obstructive vasculopathy, percutaneous transluminal angioplasty in subclavian vein on January 2013;
Hypertension;
Recently, she was hospitalized for acute pancreatitis, treated with antibiotics, and consequently temporarily changed from peritoneal dialysis to hemodialysis (2 weeks).
Abdominal physical examination demonstrated epigastric and left lower quadrant tenderness. Blood examination showed leukocytosis with neutrophil left shift and increased levels of inflammatory markers.
Few hours after recovery, the patient underwent PD exchange; the liquid in the dialysis bag appeared yellow and cloudy. On the basis of the white blood cell count and peritoneal culture examination, we added tobramycin and vancomycin to peritoneal dialysate.
After 2 days from recovery, the peritoneal fluid culture was positive for C albicans peritonitis.
Therefore, the peritoneal catheter was removed, a right femoral central venous catheter (CVC) line was inserted, meropenem and anidulafungin were started, and tacrolimus was interrupted.
Contrast enhanced computed tomography (CT) scan of the abdomen and abdominal magnetic resonance imaging (MRI) without contrast evidence “numerous pseudo cystic formation containing the corpuscular liquid defined by a thick wall adherent to the corpo caudal of the pancreas, long to the anterior zone of the left renal, that extends from the retro cavity of the greater omentum in the anterior para renal to the left lateral conal interfacial” (Figure 1, panel A). Consequently, an acute complicated pancreatitis with pseudocyst was diagnosed.

Panel A: pancreatic pseudocyst in abdominal computed tomographic scan. Panel B: abdominal magnetic resonance imaging, percutaneous cystogastrostomy drainage.
A CT-guided percutaneous cystogastrostomy catheter was maintained to drain purulent fluid (Figure 1, panel B) for 25 days.
After 2 weeks from the recovery, for the dyspnea and hypoxia, due to pulmonary consolidation and severe bilateral pleural effusion, 3 times of plural effusion tapping was needed.
After 1 month of recovery, for the febrile peaks after the dialysis session, the CVC culture examination and hemoculture were positive to Acinetobacter so the patient at first developed candida peritonitis and then sepsis due to A baumannii. The blood examination revealed procalcitonin >200 ng/mL and β-
Therapeutic regimen.

Abbreviation: HD, hemodialysis.
A CT angiography, performed 6 weeks after recovery, evidenced the “complete thrombosis of the right subclavian vein, internal jugular vein with precaval tract stenosis and thrombosis of the left common femoral vein.” Images showed the abdominal presence “of the abscess formation in the left parietocolic facial in the mesosigma tract similar to the involvement of the left fallopian tube, small fluid collection like abscess formation between tail of the pancreas and the gastric lesser curvature.” A Tesio catheter was placed in jugular vein after dilatation procedure for jugular stenosis and the left femoral catheter was removed.
For the resistant anemia, it was necessary an hemotransfusion, while was also necessary fresh frozen plasma transfusion for the suspicion of disseminated intravascular coagulation state. The patient was discharged after 3 months in improved clinical conditions, feverless stable hemodynamic state, without respiratory problems and improved inflammatory index, and the resolution of abscess formation between tail of the pancreas and gastric lesser curvature due to antibiotic therapy. The patient went on hemodialysis, 1 month after discharge.
Discussion
Acute pancreatitis is divided in 3 states: (a) mild acute pancreatitis, characterized by absence of organ failure nor local or systemic complication; (b) moderately severe acute pancreatitis, characterized by organ failure that resolves within 48 hours and/or local or systemic complication without persistent organ failure; and (c) severe acute pancreatitis, characterized by persistence of organ failure (>48 hours). The incidence of pancreatitis is higher in end-stage renal disease state and in PD patients.
Icodextrin produces a chemical irritation in the peritoneum and pancreatic glands and can be the cause of pancreatitis. 17 High intra-abdominal pressure caused by peritoneal fluid and nonphysiological composition that are able to promote the premature activation of the proteolytic pancreatic enzyme, local toxicity of peritoneal dialysate,35,36 and high level of uremic toxin and local hypercalcemia are frequent causes of pancreatitis in PD. 35
Pancreatic dysfunction can be caused by the elevated gastrointestinal enzymes such as cholecystokinin, glucagon, and gastric inhibitory polypeptide that stimulate the oversecretion of pancreatic enzymes 37 and histologic lesion similar to chronic pancreatitis. 38
Acute pancreatitis manifests with a sudden sharp severe and persistent epigastric pain; nausea and vomiting that persist for different hours 39 ; fever; tachypnea; hypotension; and retroperitoneal hemorrhage such as Cullen sign and Grey Turner sign. 25
Acute pancreatitis can be diagnosed by the sudden onset of epigastric pain with back region radiation, increase in the serum amylase or lipase enzymes 3 times higher than normal range, and evidence of the pancreatitis in the imaging examinations such as CT or MRI. 17 In patients on renal replacement therapy, it is necessary to evaluate the clinical and radiological state to diagnose the pancreatitis for the association with high-level amylase and lipase without evidence of pancreatitis 40 because of the renal clearance changes. Icodextrin can decrease amylase activity so in PD patients, it is necessary to evaluate the lipase level instead of the amylase level. Pseudocyst formation is one of the complications related to 10% of the pancreatitis, usually 4 weeks after the acute state. Pancreatic tissue necrosis can progress toward liquefaction to develop the pseudocyst that can start in pancreatic duct or can be organized by the parenchymal necrosis that destroys the ducts with high dispersion of the pancreatic secretion. This formation can be associated with abdominal pain, duodenal or vascular obstruction, fistula formation to in adjacent organs, in pleural or pericardium cavity that may cause pleural effusion, or ascites, which can be diagnosed by imaging examination (CT and MRI). About 40% of the pseudocysts improve spontaneously. The other patients should be treated with surgery methods, percutaneous or endoscopic cystogastrostomy drainage (Table 2).
Evolution of serum amylase and lipase.
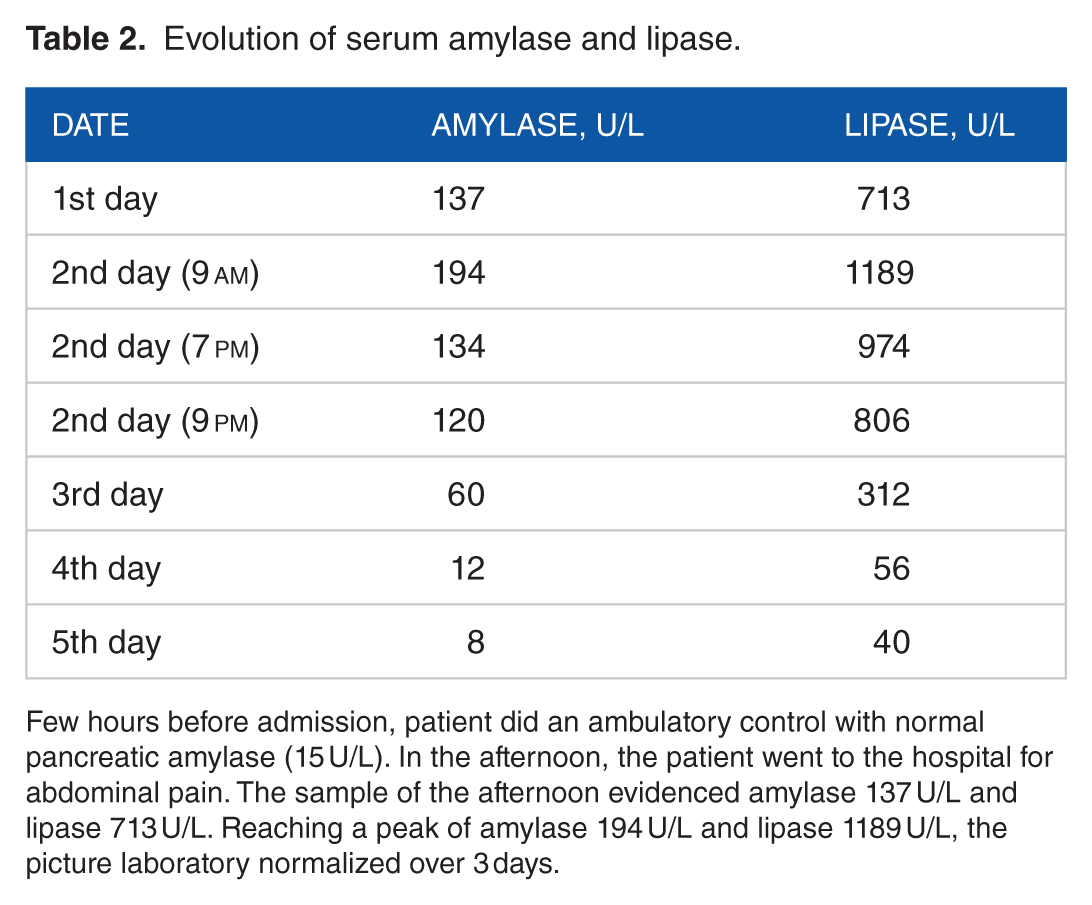
Few hours before admission, patient did an ambulatory control with normal pancreatic amylase (15 U/L). In the afternoon, the patient went to the hospital for abdominal pain. The sample of the afternoon evidenced amylase 137 U/L and lipase 713 U/L. Reaching a peak of amylase 194 U/L and lipase 1189 U/L, the picture laboratory normalized over 3 days.
Conclusions
In this clinical case, at first, the patient presented 1 episode of acute pancreatitis which demonstrated the increase in the pancreatic enzyme level, resolved within 3 days, whereas the second acute episode occurred in presence of normal amylase and lipase levels. Only the radiologic images (CT scan and MRI) demonstrated the presence of acute complicated pancreatitis with the “numerous communicated pseudo cystic formations.” This radiologic finding can be considered an acute idiopathic pancreatitis or a pancreatitis secondary to PD. The patient evidenced complicated candida peritonitis associated with acute pancreatitis and pseudocyst complicated by the overlap of pneumonitis and A baumannii sepsis.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
RA and LZ conceived and designed the experiments. LZ analyzed the data. RA wrote the first draft of the manuscript. IL, RG, SF, ER, SR, and SR contributed to the writing of the manuscript. RA, LZ, IL, RG, SF, ER, SR, SR, and FR agree with manuscript results and conclusions and made critical revisions and approved final version. RA, LZ, IL, RG, SF, ER, SR, and SR jointly developed the structure and arguments for the paper. All authors reviewed and approved the final manuscript.
Disclosures and Ethics
As a requirement of publication, authors have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality, and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. The external blind peer reviewers report no conflicts of interest.