
Abstract
Purpose:
Limited research exists regarding use of Astym® therapy with neurologic conditions. The purpose of this case was to describe using Astym therapy in treating spastic diplegic cerebral palsy (CP).
Case description:
A 6-year-old female was treated more than 9 months (36 sessions) for decreased flexibility, muscle weakness, spasticity, and abnormal gait.
Examination findings:
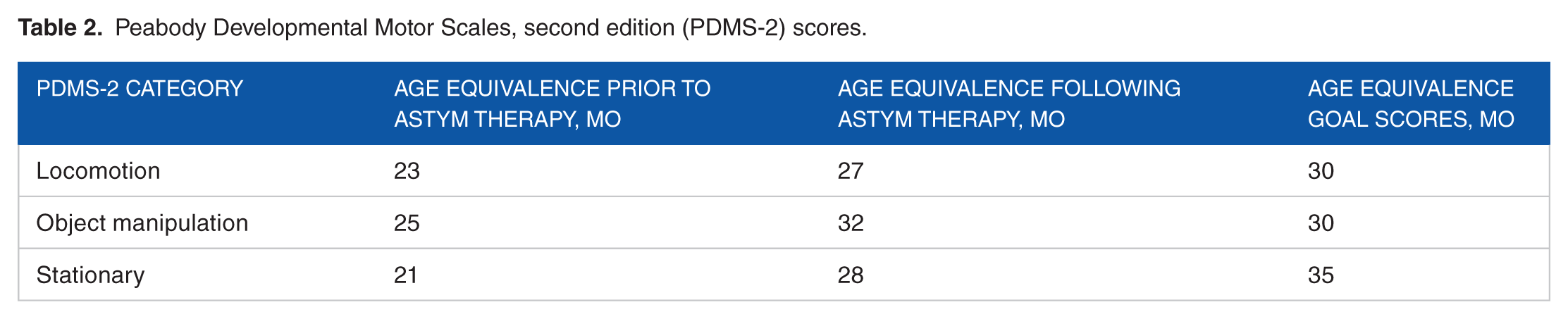
Gait performed with articulated ankle-foot orthoses (75% of the time) or foot orthosis (25%); lack of active dorsiflexion (DF); lack of heel strike during gait; spasticity in hamstrings, gastrocnemius, hip adductors; hamstring flexibility (90/90 test position) 50° right and 60° left; gastrocnemius flexibility neutral bilaterally; and Peabody Developmental Motor Scales, second edition (PDMS-2) age equivalence (in months) 23 locomotion, 25 object manipulation, and 21 stationary tasks. Therapeutic interventions included Astym therapy, stretching, strengthening, neuromuscular reeducation, and gait training.
Outcomes:
At 6 months, flexibility improved bilaterally to 10° past neutral in gastrocnemius and 0° in hamstrings. The PDMS-2 age equivalence scores were 27 locomotion, 32 object manipulation, and 28 stationary tasks. At discharge, patient ambulated full-time with foot orthosis, exhibiting improved stride length bilaterally with active ankle DF to initiate heel strike. Spasticity was unchanged.
Discussion:
Astym therapy was effective in treating a child with spastic diplegic CP, resulting in enhanced strength, flexibility, and gait.
Cerebral palsy (CP) is a nonprogressive neurologic disorder caused from brain damage incurred before, during, or after birth 1 and is the most common neurologic disorder diagnosed in children. 2 Spastic diplegic CP is one of the most common forms of the condition, affecting primarily the lower limbs and resulting in typical patient presentation of spasticity, weakness, decreased postural control, coordination issues, and gait abnormalities.1,3,4 Spasticity is a significant treatment concern for children with spastic diplegic CP, with the condition implicated in such adverse effects as deformation of maturing bone, inhibition of movement, impairment in muscle growth, and decreased protein synthesis in muscle cells. 5 Management of spasticity in children with spastic diplegic CP includes pharmacologic intervention, physical therapy, occupational therapy, use of orthoses, and surgery. 5 Components of physical therapy treatment can include stretching, tone inhibition techniques, strengthening, balance and coordination, and gait training. 5 One area that has very limited research documentation is the use of Astym therapy (Performance Dynamics, Muncie, IN, USA) for the treatment of muscular impairments from spasticity in lower extremity musculature.
Astym therapy is a therapeutic approach that has been shown to be effective in the treatment of soft tissue impairments and to promote healing associated with several musculoskeletal pathologies.6–8 The aim of Astym therapy is to engage the regenerative mechanisms of the body, stimulating tissue turnover, scar resorption, and the regeneration of healthy soft tissue structures.7,9,10 In vivo studies revealed that Astym therapy protocols improved tissue repair, increased limb function, and normalized movement patterns in an animal model.11,12 Furthermore, this research demonstrated that Astym treatment resulted in a significant increase in both fibroblast activation and fibroblast number. Clinical studies have demonstrated Astym therapy to be beneficial in the treatment of multiple musculoskeletal diagnoses by decreasing patient pain, improving function, increasing soft tissue flexibility, and joint mobility.6–9,13
Astym treatment is a noninvasive soft tissue therapy that uses handheld instruments to topically address soft tissue dysfunction. 7 The Astym instrumentation is designed to assess the presence of dysfunctional tissue by amplifying the tactile sensation of the underlying texture of the soft tissue to provide the treating clinician with indications where rough or improperly organized tissue is located. 9 As the instruments glide over dysfunctional areas, they catch on the irregularities and give the clinician and the patient a sense of roughness. 9 Astym therapy has demonstrated safety and effectiveness in the soft tissue conditions studied and is reported to be well tolerated by patients.7–9,14
Prior research on Astym therapy has mostly been conducted in patients with musculoskeletal injuries, with limited research on its use in individuals with neurologic disorders, such as spastic diplegic CP. 14 Thus, the purpose of this case report was to identify the effectiveness of Astym therapy combined with traditional outpatient physical therapy intervention in the treatment of a child with spastic diplegic CP.
Case Description
Patient information
The patient was a 6-year-old white female with spastic diplegic CP. She was diagnosed with CP shortly after birth. She began outpatient physical therapy as well as early intervention at 9 months of age to address deficits associated with CP including lower extremity weakness, developmental delay with gross and fine motor skills, and decreased flexibility. She had a history of falling due to decreased balance, limited ankle dorsiflexion (DF), and decreased strength in the lower extremities. The patient’s parents reported that she had never taken medication to treat muscle spasticity.
The patient attended a public school district with the use of a one-on-one aid. She required handhold assist when walking through the hallways or using the bathroom at school. In addition, she required assistance to open doors in the community, at home, and at school. She wore bilateral articulated ankle-foot orthoses (AFOs) 75% of the time, which included school and recreational activities. When not using the AFOs, she wore shoe-inserted foot orthoses while at home and on the weekends with light activity.
Examination
Physical therapy documentation on the episode of care was obtained retrospectively. The patient demonstrated decreased flexibility, weakness, abnormal gait, and decreased balance. Table 1 lists the patient’s flexibility in bilateral hamstrings and the gastrocnemius.
Lower extremity flexibility.

Age equivalence scores from the Peabody Developmental Motor Scales, second edition (PDMS-2) were obtained regarding her gross motor function and are depicted in Table 2. The patient presented with genu valgus bilaterally with lack of heel strike and weight bearing on toes when ambulating with foot orthosis rather than AFOs. In addition, she was unable to demonstrate active DF against the spasticity and tightness in the gastrocnemius. The patient was able to ascend and descend stairs with reciprocal pattern with use of 2 handrails. Spasticity of 1+ using the Modified Ashworth Scale was documented in bilateral hamstrings, gastrocnemius, soleus, and hip adductors.
Peabody Developmental Motor Scales, second edition (PDMS-2) scores.
The evaluating therapist was Astym certified and established a plan of care to provide weekly physical therapy treatment for this patient over a 36-week period including Astym therapy, manual stretching, functional balance, trunk stabilization, strengthening, and functional task training including gait and transfers. Rehabilitation potential for this patient was good for the goals established by the physical therapist.
Intervention
The patient was treated once a week for 36 weeks, with interventions including Astym therapy, balance training, gait training, strengthening, and manual stretching activities.
Astym therapy was begun on the first treatment session following the initial patient evaluation. Using the specialized treatment instruments (see Figure 1), Astym treatment was performed by applying instruments topically in a protocol-directed systematic pattern to deliver particular pressures and shear forces to the underlying dysfunctional tissue.9,14

Astym treatment instruments.
When performing Astym therapy, a total of 52 strokes are typically performed along the anterior aspect of a single lower extremity. An additional 58 strokes are performed on the posterior aspect of each lower extremity making for a total of 110 strokes per leg. At the beginning of therapy in this case, the strokes were performed at a faster rate of approximately 27.5 strokes per minute due to initial heightened patient sensitivity to the treatment. As the patient’s tolerance to the treatment improved, the stroke speed was decreased to approximately 22 strokes per minute. The treatment time for each Astym treatment varied between 8 and 10 minutes depending on the patient’s tolerance and her cooperation for position changes. Table 3 provides a detailed description of the Astym treatment protocol used with the patient in this case.
Astym treatment protocol to the lower extremity.
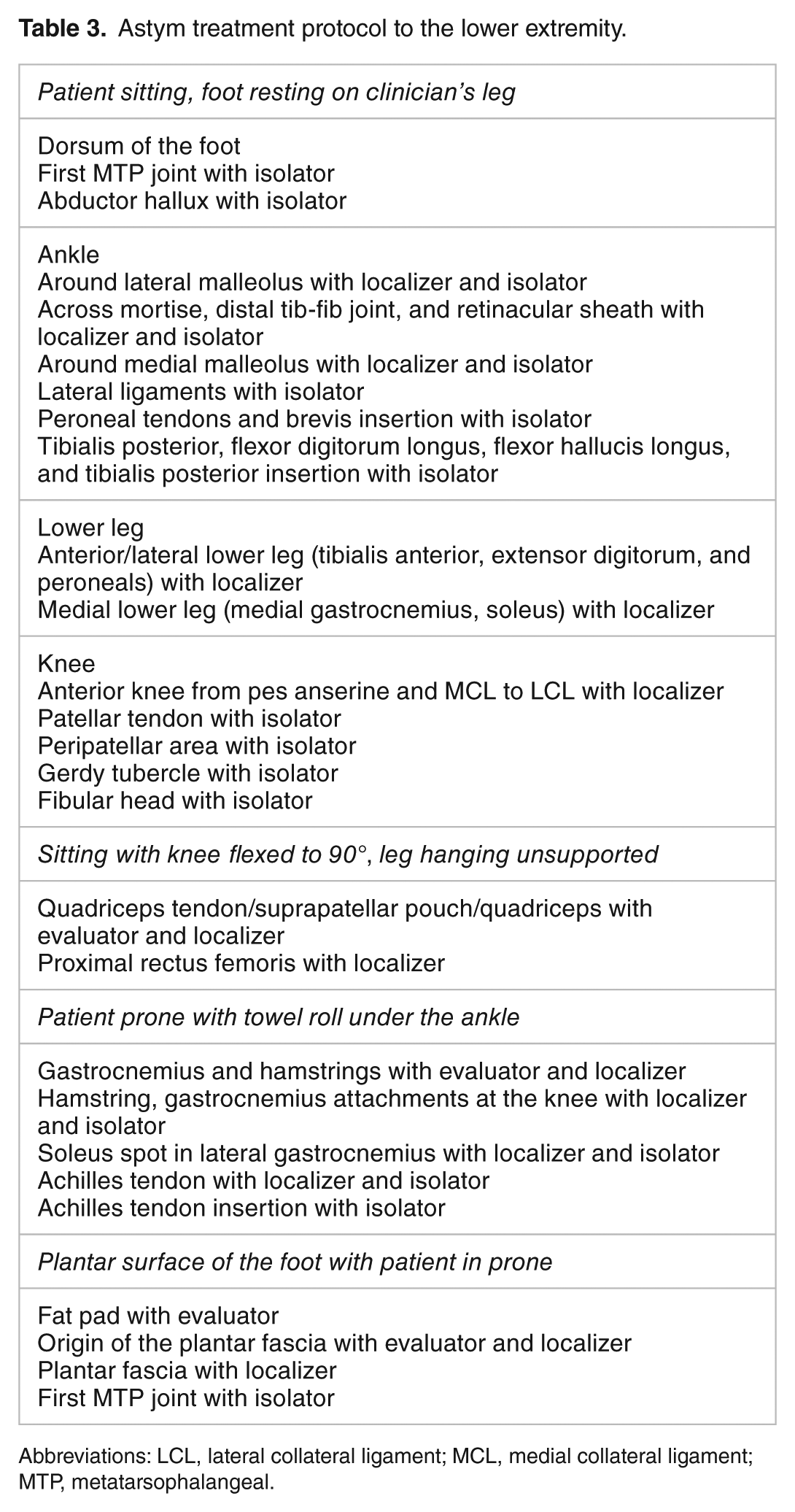
Abbreviations: LCL, lateral collateral ligament; MCL, medial collateral ligament; MTP, metatarsophalangeal.
On initiation of Astym therapy, moderate soft tissue texture was documented in ankle musculature, hamstrings, and Achilles tendon bilaterally. Tissue texture is a subjective clinician assessment that is defined as abnormal tissue consistency found in soft tissue structures during a stroke with an Astym instrument. 9 Typically, a healthy muscle has a smooth tissue texture. With injury, or in this case spasticity, collagenous tissue may form in directions that are incongruent with the direction of muscle fibers, creating an abnormal tissue texture that may be felt by the therapist through the instruments. The patient experienced and expressed some discomfort in areas of increased tissue texture during the first 3 treatments, but after that time, her sensitivity to Astym therapy decreased and she expressed few complaints regarding the intervention.
Following the Astym treatment at each session, the patient would receive manual stretching to bilateral hamstrings, gastrocnemius, hip adductors, and hip external rotators. Each stretch was completed in a slow, progressive motion to prevent activation of spasticity in the lower extremity musculature. After the conclusion of stretching, various activities were completed to focus on lower extremity strengthening, balance, functional training, and gait training (see Table 4).
Treatment activities following Astym therapy during course of care.

Outcomes
Following the 25 initial treatments of Astym therapy, the patient presented with improvements in flexibility, functional ability, and gait pattern. The patient’s flexibility improved to 10° past neutral in bilateral gastrocnemius, as well as to 0° neutral with hamstring flexibility bilaterally in 90/90 test position (see Table 1). In addition, PDMS-2 age equivalence scores improved in all categories (see Table 2). At the 25th treatment session, the patient was able to wean completely from the AFOs and was able to wear the foot orthoses full-time. The patient demonstrated decreased genu valgus collapse in bilateral knees during stance phase. In addition, she was able to initiate stance phase with foot-flat strike on the left foot but continued to demonstrate toe-touch strike on right foot. The patient no longer required a one-on-one aid in the classroom at school due to her demonstrated improvements in gait and function.
Following 36 treatments in a 9-month period of weekly Astym therapy, the patient exhibited further improvements in functional gait pattern. The patient was able to ambulate with improved stride length bilaterally with active ankle DF to obtain heel contact to initiate heel strike of gait pattern. At this time, the tissue texture during Astym treatments became reduced to minimal throughout the hamstrings, plantar surface of the feet, and gastrocnemius bilaterally. At discharge, no objective change was noted in spasticity of the lower extremities (+1 Modified Ashworth Scale).
Discussion
The purpose of the case report was to describe an episode of care involving Astym therapy in conjunction with traditional physical therapy methods in a child with spastic diplegic CP. The case report revealed that the use of Astym therapy in addition to a traditional therapeutic treatment protocol resulted in considerable gains in functional gait, lower extremity flexibility, and gross motor development in the patient. The 9-month treatment period also showed positive functional changes, such as elimination of AFO use and decreased need for aid support for school activities. These results suggest that Astym therapy can play an important role in a comprehensive physical therapy plan of care seeking to alleviate musculoskeletal performance limitations associated with CP.
Astym therapy has been shown to be beneficial in the treatment of musculoskeletal diagnoses such as hamstring tendinopathy, 7 lateral epicondylitis, 9 and Achilles tendinopathy, 8 as well as improving muscle strength. 6 The use of the procedure to address musculoskeletal problems associated with neurologic conditions is extremely limited in the research literature. To our knowledge, only one other case study has documented the use of Astym therapy in the treatment of a child with CP. Scheer et al 14 showed an improvement in lower extremity flexibility, discontinued use of AFOs, and improved activity tolerance in the 8-year-old patient following Astym therapy. The results of this case not only mirror those of Scheer et al 14 but also further document improvements in motor development as reported in the PDMS-2, improved functional gait resulting in reduction in use of assistive devices, and improved motor function achieving heel strike contact during gait.
Traditional physical therapy interventions for children with spastic diplegic CP include manual passive stretching, balance training, gait training, and functional strengthening exercises to address gross motor delays. In a systematic review by Pin et al, 15 passive stretching had minimal (<10°) effect on joint range of motion (ROM) in children with spastic CP. In this case study, when manual stretching followed Astym treatment, significant improvements in ROM occurred at the knee (50°-60°) and ankle (10°) joints due to muscle flexibility. Scholtes et al 16 noted that functional progressive resistive strengthening in children with CP resulted in improvements in strength of up to 14%, but no mobility changes were seen in the study subjects. The child in this case study demonstrated improved lower extremity motor function that allowed for initiation of bilateral active DF of her ankles, allowing her to ambulate with a slight heel strike, which consequently led to eliminating use of AFOs and improved mobility throughout her home, community, and school setting without assistance.
One factor that likely contributed to the success of Astym therapy in the patient in this case was program treatment compliance. The patient only missed one treatment during the 9-month episode of care. The Astym treatment was implemented at a quicker pace with reduced pressure for the first 3 visits due to the patient’s initial sensitivity to the intervention. As the patient’s tolerance improved, the pressure and the stroke speed were increased equivalent to that used traditionally in adults with musculoskeletal injuries. The patient and parents reported consistency in compliance with the prescribed home exercise program that involved stretching daily for the gastrocnemius, hamstring, and hip adductors. Also, both parents were supportive of the implementation of Astym therapy, although there was limited research supporting its use in neurologic conditions, which promoted a positive motivating factor for the child.
Limitations of this case study include the use of the PDMS-2 for assessment of the child. According to Wang et al, 17 the PDMS-2 is validated for use up to the age of 64 months. The child in this study turned 6 years old (72 months), only 12 days before the initial data were collected. Although previous research has reported the use of the PDMS-2 in children up to 7 years of age, such data have not yet been normalized. 18 Therefore, comparisons of the PDMS-2 results of this case with normative values should be made with caution. However, the scale was still able to provide a functional level in all categories for this child, as she had not yet achieved the maximum score allowed by the PDMS-2, and it allowed for a performance comparison over the course of treatment for this patient. Another limitation of the study is that Astym therapy was only conducted once a week, rather than the standard recommended frequency of 2 sessions per week for musculoskeletal injuries. Most of the studies regarding Astym therapy are based on receiving Astym treatments twice a week in addition to stretching and strengthening exercises.6–9,14 This can affect the ability to compare this study with others of the same nature. In addition, there were a few visits in which the physical therapist assistant treated the patient and a different Astym-certified physical therapist implemented the intervention, which could affect the consistency with application technique and therapeutic intervention. Finally, the positive treatment results noted in this case may have resulted from factors other than the Astym therapy, such as the other treatment interventions (stretching, gait training, muscle strengthening, etc) and patient maturation over the course of treatment.
Future research for the effects of Astym therapy on children with spastic diplegic CP should include the use of appropriate functional scales for the subject to guarantee proper normative values for data collection. Also, Astym treatments and therapeutic intervention should be conducted by the same therapist for every visit to assure consistency. It may also be beneficial to assess the progress of these patients once Astym therapy is discontinued, thereby determining the long-term treatment efficacy of Astym therapy. The results of this case, paired with those the case report of Scheer et al, 14 suggest that more research of a higher level of evidence is necessary to fully understand the effects of Astym therapy in treating the pediatric patient. Research that includes clinical randomized controlled trials should be conducted to better understand the clinical efficacy of Astym therapy when compared with other treatment methods in patient groups that comprise a greater number of subjects of different ages, sex, and neurologic classifications.
This case demonstrated the effects of Astym therapy on a child with spastic diplegic CP. Astym therapy treatments were implemented weekly for a total of 36 treatments and at discharge documented improvements in patient flexibility, gait, and functional ability, but no changes in spasticity as measured using the Modified Ashworth Scale. The objective improvements demonstrated by this patient after implementing Astym therapy further add to the reported clinical efficacy of the use of Astym therapy in treating pediatric patients with CP. 14 Implementation of Astym therapy as a part of a comprehensive physical therapy plan of care in individuals with spastic diplegic CP may result in improvements of patient flexibility, gait pattern, and motor function that can result in increased functional ability. Further clinical research of the use of Astym therapy in the pediatric neurologic patient is warranted.
Footnotes
Acknowledgements
The authors wish to recognize the contributions of Dr Ben Kivlan and Dr Tom Sevier in their expert review of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Primary article authors: MMM and RSV. Article review and approval: MMM, JMR and RSV. Primary Clinical Treatment and Data Collection: MMM and JMR.