
Abstract
Post-traumatic pituitary apoplexy is uncommon, most of which present with a sudden onset of severe headache and visual impairments associated with a dumbbell-shaped pituitary tumor. We experienced an unusual case of post-traumatic pituitary apoplexy with atypical clinical features. A 66-year-old man presented with mild cerebral contusion and an incidentally diagnosed intrasellar tumor after a fall accident with no loss of consciousness. The patients denied any symptoms before the accident. After 4 days, the left oculomotor nerve palsy developed and deteriorated associated with no severe headache. Repeated neuroimages suggested that pituitary apoplexy had occurred at admission and showed that the tumor compressed the left cavernous sinus. The patient underwent endonasal transsphenoidal surgery at 6 days after head injury, and the mass reduction improved the oculomotor nerve palsy completely within the following 14 days. The pathologic diagnosis was nonfunctioning pituitary adenoma with hemorrhage and necrosis.
Keywords
Introduction
Pituitary adenoma rarely causes oculomotor nerve palsy, and in such a case, pituitary apoplexy (PA) usually coincides. Risk factors for PA are variable: tumor-related (large size, invasion into the cavernous sinus), treatment-related (surgery, radiation, bromocriptine), and other (hypertension, diabetes mellitus, changes in the intracranial pressure, cerebral angiography, anticoagulant drugs, endocrinological loading tests, head trauma) factors were reported.1–3 Clinical features of post-traumatic PA are similar to those of other PAs. The main symptoms are a sudden onset of severe headache and visual impairments, and PA usually occurs in a dumbbell-shaped tumor irrespective of the trigger.4,5 To our knowledge, the authors report the first case of post-traumatic PA that occurred in an intrasellar pituitary adenoma, causing delayed onset of isolated oculomotor nerve palsy without headache.
Case Report
A 66-year-old man with previous diseases of hypertension and diabetes mellitus under neither antiplatelet nor anticoagulant therapies slipped and fell down a ladder, suffering head trauma. He had no loss of consciousness and denied any symptoms including headache and visual impairments before the accident as well as on admission. Admission computed tomography (CT) scan revealed the left frontal lobe contusion and an intrasellar pituitary incidentaloma (Figure 1). After 4 days, he noticed diplopia and ptosis of the left eye. On neurological examination, ptosis was present on the left side, and restriction of medial and upward movement of the left eye was observed. Bilateral pupils were equal in size and normally reacting to light. Visual acuity and field were normal. No periorbital swelling was observed. The findings were deteriorated to complete left oculomotor nerve palsy including complete ptosis and pupillary dilatation not reacting to light in 2 days. Repeated CTs and magnetic resonance images showed that there were no traumatic lesions causing the oculomotor nerve palsy, the left cavernous sinus was compressed by an intratumoral nonenhancing area suggesting hemorrhage, and tumor size was unchanged compared with the admission CT, but sphenoid sinus mucosa was progressively thickened after admission (Figures 2 and 3). Routine laboratory tests and basal endocrinological work-up showed no abnormalities. Although the patient had not experienced clinical symptoms such as headache, nausea, visual impairments, and hypopituitarism, we diagnosed that the oculomotor nerve palsy was due to post-traumatic PA. The patient underwent endonasal transsphenoidal surgery for the PA, and the tumor was almost totally removed except for a part of the pseudocapsule. Postoperatively, neither diabetes insipidus nor hypopituitarism occurred. The oculomotor nerve palsy gradually improved from the day after the surgery and completely resolved at 14 days postsurgery. The pathological examination demonstrated nonfunctioning pituitary adenoma with hemorrhage and necrosis.
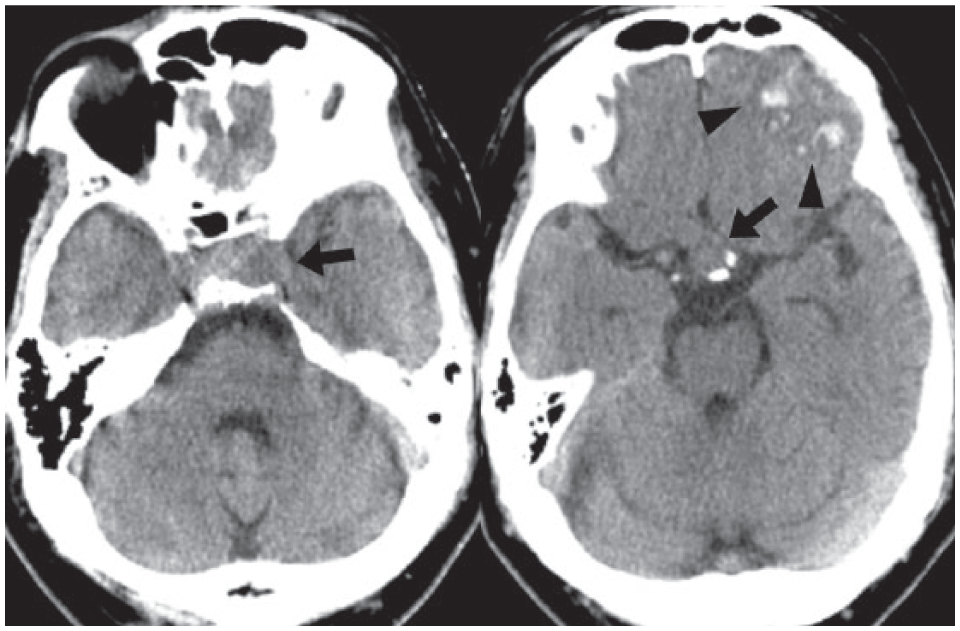
Admission computed tomography showing the left frontal contusion (arrowhead) and an intrasellar mass (arrow).
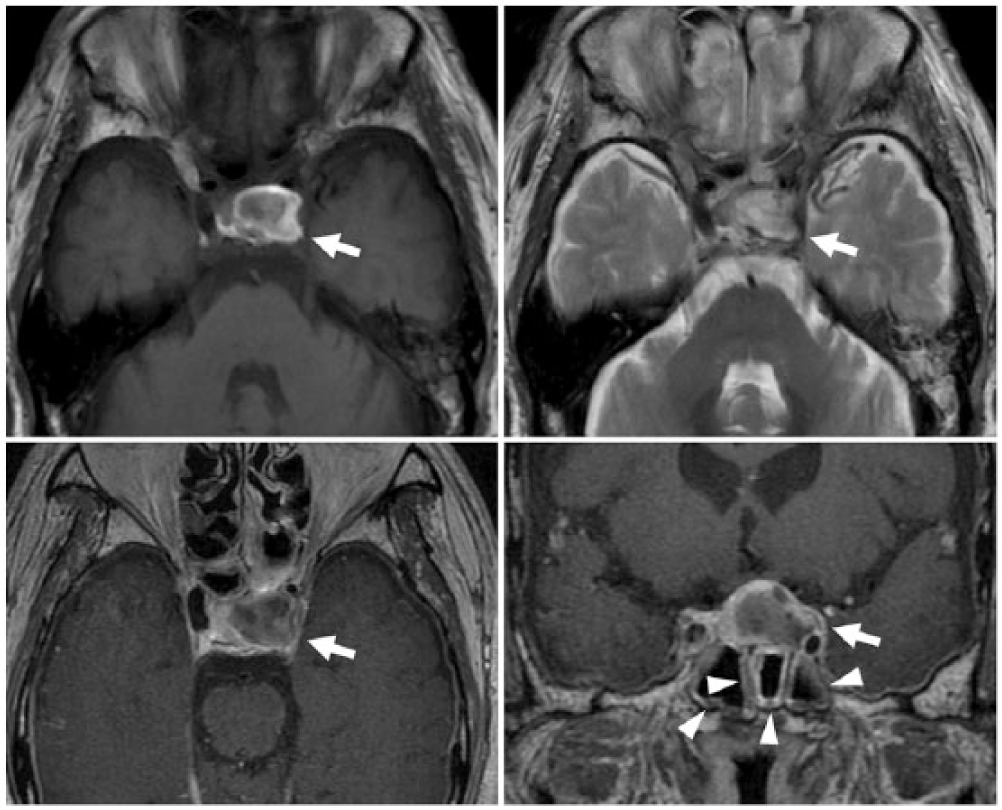
T1-weighted (upper left) and T2-weighted (upper right) axial images obtained at 4 days after admission, and contrast-enhanced T1-weighted axial (lower left) and coronal (lower right) images obtained at 5 days after admission. Magnetic resonance images show that there is no traumatic lesion causing an oculomotor nerve palsy but reveal hemorrhage in an intrasellar mass, which is compressing the left cavernous sinus (arrow), associated with the sphenoid sinus mucosa thickening (arrowhead).
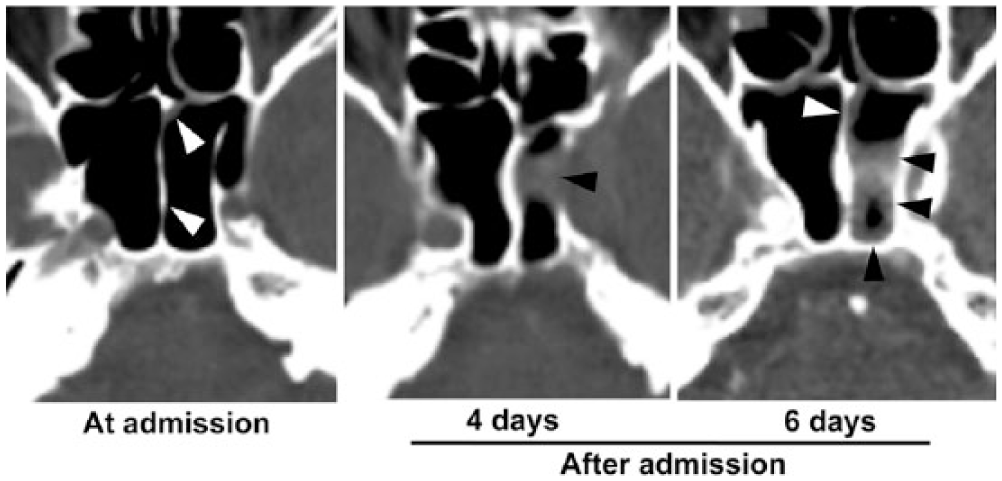
Repeated computed tomography showing that the sphenoid sinus mucosa thickening (arrowhead) is progressively aggravated from admission to 6 days after admission.
Discussion
The isolated oculomotor nerve palsy is rare, which is mainly caused by microvascular ischemia to the nerve and less commonly by trauma, tumors, or other causes.6,7 If patients had oculomotor nerve palsy after trauma, traumatic oculomotor nerve palsy should be ruled out. However, the prognosis of traumatic oculomotor nerve palsy is poor, and few full recoveries are observed even after several months. 8 In contrast, oculomotor nerve palsy due to PA is usually recovered completely and relatively quickly as in our case.9–13 The duration necessary for recovery of cranial nerve palsy is correlated with the length of time between the onset of symptoms and surgery,3,11 indicating need for early diagnosis and treatment. 10 Therefore, when patients with pituitary adenoma had oculomotor nerve palsy after trauma, it is crucial to keep it in mind that post-traumatic PA can cause oculomotor nerve palsy.
There are a few reports of post-traumatic PA. The main symptoms are severe headache at onset, visual impairments, disturbance of consciousness, and hypopituitarism.4,5 Most of the post-traumatic PAs occur in a dumbbell-shaped pituitary adenoma extending to the suprasellar region within 24 hours after head injury.4,5 It has been hypothesized that a traumatic rotational force produces a shearing strain between intrasellar and suprasellar parts of tumor, resulting in PAs.4,5 Severe headache is considered to occur due to stretching of the hypophyseal capsule by an expanding mass and/or extension of the bleeding into the subarachnoid space. 1 As PA in this case occurred in an intrasellar tumor and was associated with no typical symptoms and signs, the diagnosis of PA was difficult.
One of the characteristic imaging findings of PA is sphenoid sinus mucosa thickening.14,15 Arita et al 13 reported that sphenoid sinus mucosa thickening occurred within 7 days after PA and continued for 3 months. The mechanism of sphenoid sinus mucosa thickening may be due to congestion of dural blood flow caused by increased pressure in the cavernous or circular sinus.13–15 In our case, admission CT failed to show the sphenoid sinus mucosa thickening. In addition to neuroimages suggesting intratumoral hemorrhage, however, the findings that sphenoid sinus mucosa was thickened progressively after admission enabled us to diagnose our case as a new onset of PA, which might be triggered by head trauma.
The mechanisms of how PA occurred in such an intrasellar tumor are speculative. In our case, head injury might cause contusion of pituitary adenoma by the surrounding bony structures, wall of cavernous sinus, and clinoid ligaments, followed by hemorrhage. As the tumor might become more edematous, the intrasellar pressure might increase and cause sphenoid sinus mucosa thickening, as well as the compression by the tumor onto the oculomotor nerve might increase, resulting in the oculomotor nerve palsy. However, because the pituitary mass or bleeding neither extended to the suprasellar space nor stimulated or stretched the hypophyseal capsule and the arachnoid membrane, severe headache might not occur.
In conclusion, for early diagnosis and treatment, the possible association of isolated oculomotor nerve palsy and PA should be kept in mind even though pituitary adenoma is small and mainly exists in the intrasellar space, and the symptoms develop without severe headache in a delayed fashion after a relatively minor head trauma.
Footnotes
Peer review:
Four peer reviewers contributed to the peer review report. Reviewers’ reports totaled 419 words, excluding any confidential comments to the academic editor.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
TI, FM, and HS conceived and designed the experiments. TI wrote the first draft of the manuscript. TI, GM, and HS contributed to the writing of the manuscript. TI and HS jointly developed the structure and arguments for the paper. All authors analyzed the data, agree with manuscript results and conclusions, made critical revisions and approved final version, reviewed, and approved the final manuscript.
Disclosures and Ethics
As a requirement of publication, author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality, and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest.