
Abstract
It is well known that some disorders can cause concomitant kidney dysfunction with lung involvement. These syndromes, characterized by the simultaneous presence of intra-alveolar hemorrhage and acute glomerulonephritis, are caused by numerous and variable disorders. The most frequent are the antineutrophil cytoplasmic antibodies (ANCA)-associated vasculitis and Goodpasture syndrome. A quick discerning of the underlying causes and initiation of adequate treatment is crucial to prevent acute respiratory failure and irreversible loss of renal function. We reported the case of a 33-year-old man having hemorrhagic alveolitis presenting a picture consistent with Goodpasture syndrome in the absence of anti-glomerular basement membrane (anti-GBM) antibodies or ANCA at lab test and a review of literature. This case highlights the need to consider the chances of falsely seronegative cases of anti-GBM disease, as well as the importance of using all available assay routine tests. These cases would appear indeed more common than before if just taken into consideration their existence. Several reports have shown false seronegatives especially in patients with relapses, in smokers, and in patients with predominantly pulmonary symptoms.
Introduction
It is well known that some disorders can cause concomitant kidney dysfunction with lung involvement. 1 These syndromes are characterized by the simultaneous presence of intra-alveolar hemorrhage and acute glomerulonephritis. They do not represent a single entity but are caused by several disorders. The most frequent disorders are the antineutrophil cytoplasmic antibodies (ANCA)-associated vasculitis and Goodpasture syndrome. 2 Failure to diagnose and treat the right condition can result in a life-threatening illness, acute respiratory failure, and/or acute renal failure. 3 Here, we reported the case of a patient with hemorrhagic alveolitis presenting a picture consistent with Goodpasture syndrome, but in the absence of positive serum. We have obtained fully informed, voluntary, and written consent from the patient to publish this report.
Case Report
A 33-year-old man was admitted to the hospital for the severe anemia, unresponsive to hemotransfusions and increasing doses of erythropoietin. He had membranoproliferative glomerulonephritis diagnosed through renal biopsy 5 years ago and treated with steroids and immunosuppressants. The diagnosis of glomerulonephritis was made on the basis of persistent proteinuria and microhematuria. Renal biopsy revealed a picture of membranoproliferative glomerulonephritis with glomerular sclerosis (a total of 9 out of 16 glomeruli were entirely sclerosed). Seven glomeruli showed a mesangiocapillary global proliferation. The results did not indicate fibrinoid necrosis, vascular thrombosis, or extracapillary proliferation. The Congo red staining for amyloid was negative. The immunofluorescence (IF) results showed tiny granular deposits; semilinear membrane for immunoglobulin G (IgG) and, to a lesser quantity, to C3; negative immunoglobulin A (IgA), immunoglobulin M (IgM), C1q, and κ and λ light chains. A modest accumulation of intravascular fibrinogen was observed.
The patient was treated first by bolus of azathioprine and successively replaced by mycophenolate; neither was tolerated by the patient. Consequently, he remained under steroid therapy only. A rapid reduction in proteinuria and disappearance of microhematuria were observed. However, the following year, the patient presented a bilateral aseptic necrosis of the femoral head.
In the past 5 years, the patient stopped also the steroids and revealed a slow worsening renal function (mean serum creatinine: 2.5 mg/dL), proteinuria (1.5-2 g/24 h), and anemia, successfully treated with darbepoetin alfa, until he was promptly admitted to the emergency room and hospitalized for the detection of severe anemia (hemoglobin: 6 g/dL) associated with severe asthenia and dyspnea even for minor efforts. Before admission, the patient has not taken corticosteroids or other immunosuppressive drugs. Hemoglobin values increased after hemotransfusion of 2 units of packed red blood cells. A colonoscopy and gastroscopy revealed no significant alterations. The peripheral smear did not show any schistocytes, and both direct and indirect Coombs tested negative. A dose of G6PDH appeared within the normal range. The haptoglobin was reduced and lactate dehydrogenase increased slightly, but both direct and indirect bilirubin levels fall in the normal range. Autoimmunity was normal with the exception of a persistent slight reduction in C3 that the patient has maintained during the past 6 years (Table 1).
Clinical features of patient on admission.
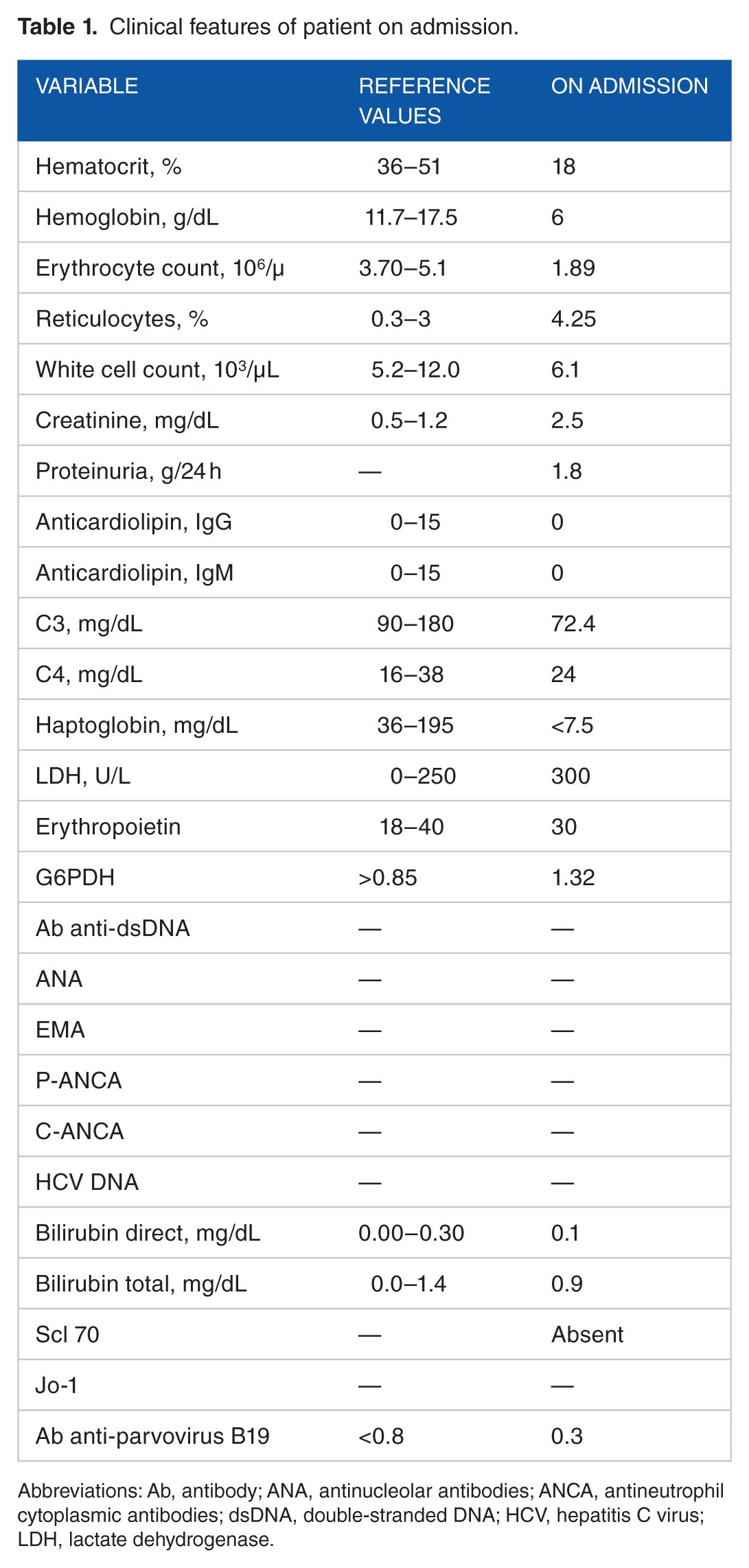
Abbreviations: Ab, antibody; ANA, antinucleolar antibodies; ANCA, antineutrophil cytoplasmic antibodies; dsDNA, double-stranded DNA; HCV, hepatitis C virus; LDH, lactate dehydrogenase.
Complement consumption led to the base pathology, and no additional elements were observed from the clinical picture or test results. Antinucleolar antibodies were also evaluated (jo-1, Scl 70). The most common infectious agents were tested through serology, urine, and blood cultures, but the analyses excluded ongoing infections. It was then decided to administer 8000 IU of erythropoietin alfa 3 times a week.
On the third day of admission, hemoglobin levels decreased by 7 g/dL, so we proceeded with the infusion of a new unit of packed red blood cells. A full-abdomen ultrasound scan showed no blood abdominal collections or significant changes, just kidney size reduction such as in chronic kidney disease. On the same day, chest X-ray imaging revealed bronchopneumonia bilaterally spread in the middle lobe. After 4 days of hospitalization, the patient presented hemoptysis with bright red blood and clots when coughing for several days, symptoms which had not absolutely been observed the previous days. This prompted an urgent chest computed tomographic (CT) scan, documented as “multilobar alterations extended to both lungs with ground-glass appearance and intralobular involvement, as well as intra-acinar, with thickening of the interlobular septa but without distortion and rails and interlobular fissures. The ground-glass appearance seemed to spare the sub pleural zones” (Figure 1, Panel A). Diffusion lung CO (DLCO) analysis showed an increase in DLCO (157%) associated with reduction in alveolar volume. The patient presented intra-alveolar hemorrhage consistent with Goodpasture syndrome. We administered therapy with methylprednisolone, 2 boluses of 500 mg for the first 2 days, then 250 mg for 3 days, and, after that, the steroid therapy was continued with prednisone 1 mg/kg/d (subsequently reduced after discharge) and associated with a dose of 75 mg of azathioprine per day, and low-flow oxygen therapy to be taken periodically during the day. Given the clinical picture and the strong suspicion of kidney-lung syndrome, the search of anti-glomerular basement membrane (anti-GBM) antibodies was immediately requested to the analysis laboratories, before starting immunosuppressive therapy. Given the high percentage of false-negative serum cases of Goodpasture syndrome in the literature, extensive workup was done and the examination was performed in both IF and chemiluminescence. Antibodies came out negative in both cases, as well as C-ANCA and P-ANCA. The patient also underwent a transnasal endoscopy, which signaled the presence of bleeding striae in the first tracheal rings, requiring a further bronchoscopy. The results, performed 2 days later, revealed no lesions visible at tracheal level or in both bronchial trees, explored up to the fourth-order branches. The liquid recovered from a bronchoalveolar lavage was blood, a condition that could be associated with the suspected diagnosis of Goodpasture syndrome despite negative antibodies, and renal biopsy performed years ago had not shown the characteristic fibrinoid necrosis of Goodpasture disease.

Panel A: computed tomographic (CT) scan on admission showing multilobar alterations extended to both lungs with ground-glass appearance and intralobular involvement, as well as intra-acinar, with thickening of the interlobular septa but without distortion and rails and interlobular fissures. The ground-glass appearance seemed to spare the sub pleural zones. Panel B: CT scan 20 days after diagnosis of hemorrhagic alveolitis: the widespread areas of increased density with ground-glass appearance appeared reduced in both lungs. The thickening of the bronchial walls and interlobular septa persisted though.
On immunosuppressive therapy, there was noticeable improvement in the clinical picture and test results. The fatigue and dyspnea were gradually reduced. The oxygen saturation progressed satisfactorily. The patient did not require further transfusions, and after a few days, he no longer needed peripheral oxygen saturation constantly maintained at around 98% in the ambient air.
Despite improvement in the lung framework, there was a rapid deterioration of renal function: the initial filtrate of 17 mL/min according to Modification of Diet in Renal Disease formula reduced to 11 mL/min, with an increase in blood urea and in creatinine values, as well as in potassium and in phosphorus concentrations. The patient, informed about the need to start renal replacement therapy, freely requested to start peritoneal dialysis.
After 20 days of diagnosis of hemorrhagic alveolitis, the patient underwent a CT control chest (Figure 1, Panel B) that revealed considerable improvement. The widespread areas of increased density with ground-glass appearance appeared reduced in both lungs. The thickening of the bronchial walls and interlobular septa persisted though.
Spirometry and DLCO test showed a visible improvement of the clinical picture. Immunosuppressive therapy was gradually reduced until the patient was discharged.
The hemoglobin level was maintained with an average value of 11 g/dL with lower erythropoiesis-stimulating agent doses. The patient began automated peritoneal dialysis with moderate mental and physical well-being and no notable disorders.
About 1 month after suspension of immunosuppressive therapy, another dosage of Ab anti-GBM was required to re-evaluate the results, which have come out negative again.
Discussion and Review of Literature
Diffuse alveolar hemorrhage (DAH) represents a diagnostic challenge in acute respiratory failure. A quick discerning of the underlying causes of DAH and initiation of adequate treatment is crucial to prevent acute respiratory failure and irreversible loss of renal function. 1
The published literature concerning concomitant lung-kidney dysfunction describe only a few cases (Table 2). These syndromes are characterized by the simultaneous presence of diffuse intra-alveolar hemorrhage and acute glomerulonephritis.2,3 Not only caused by a single entity, but also by numerous and various diseases, among which the most common are ANCA-associated vasculitis and Goodpasture syndrome. 4 It is therefore essential to promptly identify the pathology responsible for the clinical picture and treat it as soon as possible because failure to do this can cause acute respiratory failure and/or acute renal failure, requiring hospitalization in intensive care units. This condition has a very high mortality rate that can reach as much as 25% to 50%. 5
Anti-GBM disease with an atypical serology, review of literature.

Abbreviations: ANCA, antineutrophil cytoplasm antibodies; anti-GBM, anti-glomerular basement membrane; ELISA, enzyme-linked immunosorbent assay.
Our patient presented with severe anemia which was then discovered to be caused by alveolar hemorrhage associated with decreased renal function already compromised by membranoproliferative glomerulonephritis. No microangiopathy was present; hemolysis indexes had slightly changed, but no values hemolytic anemia were found. All infection indexes were negative.
X-ray imaging was nonspecific; at first, the differential diagnosis was pulmonary edema, pulmonary hemorrhage, and acute respiratory distress syndrome. But chest CT scan and then bronchoscopy confirmed the presence of alveolar hemorrhage, supported also by DLCO test results. Renal ultrasonography revealed a framework consistent with a long-standing chronic injury.
Goodpasture disease is commonly associated with pulmonary hemorrhage, especially in young men. The severity of pulmonary hemorrhage varies widely, but it can be life-threatening. Lung irritants (for example, cigarette smoke, hydrocarbon vapors, cocaine) or pulmonary infections may precipitate the hemorrhage. 15 Our patient was a smoker. In anti-GBM disease, kidney injury is rather a crescent necrotizing glomerulonephritis, and lung injury is a bland noninflammatory alveolar hemorrhage.
Iron deficiency anemia can be due to lung bleeding; the serum complement levels are usually normal or slightly reduced, as in this case. Detection of autoantibodies is characteristic of anti-GBM disease (IgG typically, only occasionally IgA) directed to epitopes expressed on type IV collagen. Approximately 20% to 30% of patients may have also shown to have ANCA. 16
This patient presented proteinuria, hematuria, and hypocomplementemia and bronchoalveolar hemorrhage. All signs could support the diagnosis of anti-GBM disease despite negative antibodies.
Our diagnostic suspicion was also initially placed on hemolytic-uremic syndrome (HUS), an acute, potentially lethal pathological condition characterized by a triad of hemolytic anemia, acute kidney failure, and thrombocytopenia. However, the absence of thrombocytopenia, schistocytes, and signs of hemolysis ruled out this diagnosis.
The only thing that connects us to an autoimmune etiology is complement consumptions, already present in the patient for several years, but which was then accompanied by rapid deterioration of renal function that had remained stable over the past 4 years. Another important sign was the patient’s immediate response to immunosuppressive therapy. 11
In Goodpasture disease, C3 may not only be reduced but also stay within the normal range. The examination of the complement helped us to make a differential diagnosis. In fact, in our patient, only C3 was low, whereas C4 and CH50 were within the normal range. 17
In HUS, C3 values are low and those of C4 increase; in cryoglobulinemia with nephritis, C3 levels are normal and C4 levels are lower; and in systemic lupus erythematosus (SLE), C3 and C4 levels are reduced.
Patients with anti-GBM disease with exclusive lung involvement make rather rare cases; however, these have been characterized in the literature; the pathogenesis of this presentation is unknown. Some of these patients may have an underlying renal condition that is not specified unless a kidney biopsy is performed. It has been suggested that lung disease may precede renal symptoms in these patients, and that early aggressive treatment can therefore attenuate renal involvement. 18
The classical clinical presentation of hemoptysis accompanying glomerulonephritis is not consistent, so it is probably less frequent than a subtler mode of presentation or characterized by nonspecific symptoms such as weight loss, arthralgias and myalgias, fever, cough, dyspnea, and anemia. In fact, hemoptysis, alveolar bleeding, may miss up to a third of cases. In line with the classic presentation of rapidly progressive glomerulonephritis, there are clinical pictures of microscopic hematuria, proteinuria, cylindruria, and high blood pressure, which only evolve toward renal failure. 19
These events are accompanied by specific symptoms of each disorder such as skin changes, involvement of the upper airways (sinusitis, otitis), and the presence of disease.
Patients having microscopic polyangiitis with pneumatic-renal syndrome had fever (62%), arthralgias and myalgias (52%), upper airway symptoms (31%), and skin involvement (17%).2,20
A crucial element in differential diagnosis is serology: ANCA and Ab anti-GBM, Ab anti–double-stranded DNA, and anti-Sm in SLE; lupus anticoagulant and anticardiolipin Ab in antiphospholipid syndrome; cryoglobulins in cryoglobulinemia; and anticentromere/anti Scl 70 in systemic sclerosis. 15 Equally important is the study of coagulation and platelet counts, particularly in a differential diagnosis, and discoagulative with hemorrhagic diseases. Antibodies responsible of Goodpasture syndrome are directed against the first noncollagenous domain of the α3 chain of collagen type IV (α3 NC1-IV), expressed in basal membranes of glomeruli, renal tubules, cells, choroid plexus, and retinal capillary Bruch membrane. 21 In the kidneys, antibodies bind to the GBM and activate complement and some protease, causing damage to the glomerular structure with the consequent loss of protein and the formation of “crescents.” It is good to act prematurely because early diagnosis allows prompt therapy with a lower risk of evolution of the pathology. Goodpasture disease could even begin with a negative status nonetheless. Salama et al have indeed estimated that the serum anti-GBM negative can occur in 2% to 3% of the patients in England. One possible explanation for this phenomenon lies in the limitations of some laboratory techniques (enzyme-linked immunosorbent assay, IF, and immunoblot). 22
Another possible explanation is that smoke tends to produce antibodies that react with antigens or epitopes considered similar to those of a typical anti-GBM, which also react with NC1 region of collagen type IV. Ohlsson et al reported the cases of 4 young women with severe alveolar hemorrhage and renal involvement who had a prevalence of anti-GBM IgG4 antibodies that were not detected by routine laboratory tests. It was concluded that there are subtypes of anti-GBM Ab which are not identified through routine tests. 23
In addition, subjects with very low levels of anti-GBM antibodies are likely to develop isolated pulmonary hemorrhage when exposed to irritating precipitants. In anti-GBM disease, the development of pulmonary involvement requires no additional specific lung injury that increases the alveolar-capillary permeability as concomitant infections, fluid overload, high concentrations of inspired oxygen, volatile hydrocarbons, and cigarette smoke. The smoke factor is strongly correlated with the development of pulmonary hemorrhage in patients with anti-GBM disease. 24
Serisier et al evaluated 25 subjects, all smokers, who presented alveolar hemorrhage and minimal evidence of renal involvement. Such subjects may represent a subgroup with anti-GBM disease, early and relatively low levels of circulating antibodies that manifest pulmonary disease due to the direct effects of cigarette smoking on alveolar walls. 25 Smoking has been linked to recurrent disease and may have been the trigger in this case, and we also consider that our patient has stopped smoking immediately after the initial diagnosis. It is also possible that smoking could have stimulated the production of anti-GBM antibodies allowing direct contact between the alveolar basement membrane and the immune system. 26
Other environmental triggers that have been implicated in relapse include organic solvents, hydrocarbons, chlorine gas, and exposure to carbide. Some case reports have also suggested cocaine and urinary tract infection as a trigger for relapse.
Despite the negative status, our patient showed a pulmonary picture consistent with Goodpasture syndrome. What the biopsy detected 5 years earlier did not show the typical necrotizing vasculitis with the presence of crescents and IF linear deposition of IgG along the basement membrane, but nevertheless, the picture is consistent with membranoproliferative glomerulonephritis. It would be useless to run a new biopsy but, given the reduction in kidney size and the filtrate rates, it was deemed inappropriate, and although lung biopsy would definitely reveal the cause of the disease, the delicate condition of the patient made us postpone this procedure.
The immunity tests came out negative with a slight reduction in C3, which could be consistent with said syndrome. The patient was a smoker and this could unmask a disease with a low level of antibodies.
Conclusions
This case highlights the need to consider the chances of falsely seronegative cases of anti-GBM disease, as well as the importance of using all available assay routine tests. These cases would appear indeed more common than before if that were taken into consideration. Several reports have shown false seronegatives especially in patients with relapses, in smokers, and in patients with predominantly pulmonary symptoms. 10 Renal biopsy should be considered in a patient with DAH even with minimal renal involvement because an early diagnosis of anti-GBM disease means the start of a life-saving treatment. In these patients, early diagnosis of anti-GBM disease helps us raise awareness on the importance of quitting smoking and careful monitoring for recurrence.
Footnotes
Peer review:
Two peer reviewers contributed to the peer review report. Reviewers’ reports totaled 496 words, excluding any confidential comments to the academic editor.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
LZ and FR in the interpretation of data; in the conception and design of the study; interpretation of data; revising of the manuscript for intellectual content. VS, ER and GD in the drafting of the manuscript.