
Abstract
Foreign body ingestion is a common occurrence in the pediatric population and most ingestions resolve with little morbidity. Although radiopaque objects are easily identified on biplane radiographs, radiolucent objects may elude detection, delaying diagnosis. We report a case of a healthy 10-month-old infant who presented with a 5-day history of postprandial vomiting and imaging consistent with small bowel obstruction. On exploratory laparotomy, she was discovered to have a postpyloric foreign body requiring removal through an enterotomy.
Case
A 10-month-old, 6.5-kg, otherwise healthy female infant was brought by her parents to a community hospital with a 3-day history of vomiting. She was evaluated and discharged home the same day with antiemetics and antibiotics. After 2 days, she returned to the emergency department for progressive feeding intolerance, bilious emesis, decreased urine output, and absence of bowel movements. An abdominal computed tomographic (CT) scan was obtained and showed fluid-filled small bowel concerning for obstruction. The patient was transferred to our tertiary care children’s hospital for further evaluation and treatment.
An acute abdominal series showed a nonspecific bowel gas pattern with moderate distention of the stomach and duodenum near the duodenojejunal junction on the anteroposterior view along with air-fluid levels on the lateral view (Figure 1). A subsequent upper gastrointestinal (GI) series (Figure 2) confirmed prominent fluid-filled dilation of the proximal small bowel concerning for a mid small bowel obstruction, with notable gastroesophageal reflux. Subsequently a 10 French nasogastric (NG) tube was placed and 300 mL of green bilious fluid was evacuated over the course of several hours. Fluid resuscitation was initiated with a normal saline bolus. Laboratory investigations showed the following: white blood cells: 13.7 bil/L, hemoglobin: 12.9 g/dL, platelets: 395 bil/L, sodium: 131 mmol/L, potassium: 5.0 mmol/L, chloride: 91 mmol/L, bicarbonate: 24 mmol/L, blood urea nitrogen: 16 mg/dL, creatinine: 0.3 mg/dL, and glucose: 96 mg/dL. She was scheduled for an emergent exploratory laparotomy to evaluate and treat the small bowel obstruction.

Anteroposterior (left panel) and lateral (right panel) abdominal radiographs showing moderate stomach and duodenal distension with air-fluid levels.

Upper gastrointestinal series before (left panel) and after (right panel) contrast administration with evidence of air filled bowel loops and obstruction.
Preoperatively the infant was febrile and tachycardic, with movement causing agitation and crying. Her breathing was unlabored, and the remainder of her examination was unremarkable. Her parents denied any other medical history or prior anesthetic exposure.
The patient was taken to the operating room, anesthetized via rapid sequence induction, and intubated. During surgical exploration of the abdomen, a mobile, spherical object causing severe obstruction was identified approximately one-third of the way through the small bowel; the object could be manipulated within the bowel lumen but would not pass distally. Attempts were made to maneuver the object back into the stomach without success. The object was returned to its distal position and surgically removed through a small enterotomy. The foreign body was noted to be a 2.5-cm radiolucent spherical object consistent in appearance with a bouncy ball (Figures 3 and 4). The patient remained hemodynamically stable throughout the case and blood loss was minimal. After manipulation of the NG tube during the case, another 100 mL of fluid was evacuated from the stomach. The surgical incisions were closed and the patient emerged from anesthesia and was extubated uneventfully. By postoperative day 4, she had return of bowel function and was discharged home the following day.

Mobile object within the jejunal lumen being removed through an enterotomy.
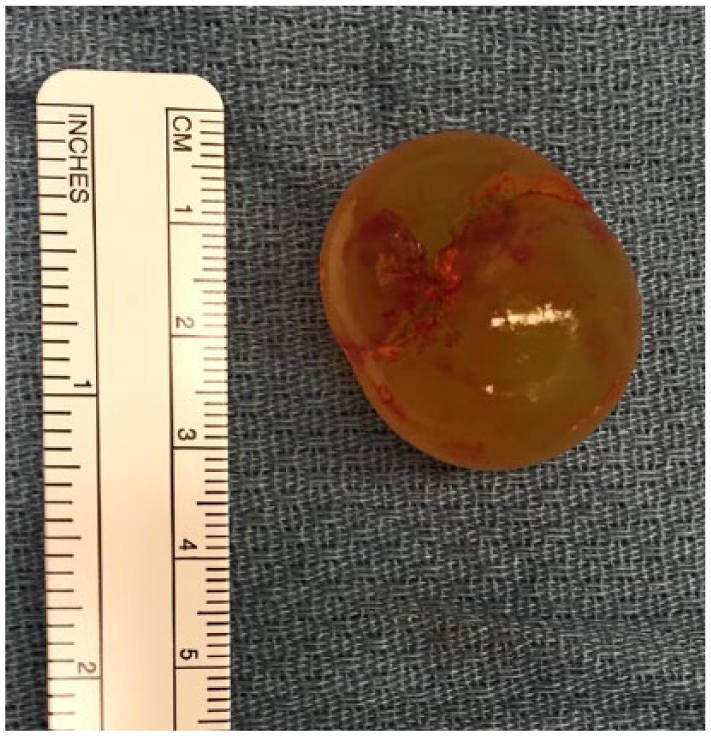
The postpyloric foreign body after removal: a 2.5-cm radiolucent spherical object consistent in appearance with a toy “bouncy” ball.
Discussion
Foreign body ingestion is a common occurrence in the pediatric population with potential to cause serious clinical consequences. Most of the ingestions in children (98%) are unintentional and up to 50% are asymptomatic. 1 Of the reported foreign body cases, 75% occur in children under 4 years of age.1,2 This underscores the importance for close supervision of small children and continuing education of parents. Other at-risk populations include patients with developmental delay or psychiatric conditions. 1 The ingested object may pass without harm or may cause complications such as mucosal injury, bleeding, obstruction, or organ perforation. 2 If the foreign body is small enough to pass through the pylorus, it will usually traverse the remainder of the digestive tract without complication. 3 Less than 1% require open surgical intervention. 4
Presentation may be delayed by several days in nonverbal children, with nonspecific signs necessitating a high level of suspicion as rare complications may develop. In this unique case, a large radiolucent (2.5 cm) object cleared the infant’s esophagus and pyloric sphincter but was unable to pass through the length of the small bowel, creating significant obstruction. Failure to recognize foreign body ingestion can also lead to misdiagnosis, as another patient being worked up for Crohn disease was found instead to have multiple pieces of plastic wrap from a food label retained in the bowel. 5
Although radiopaque objects are readily identified by x-ray, ingested radiolucent objects may remain undetected; thus, a foreign body cannot be ruled out by a normal radiograph. 6 Radiopaque materials include metallic objects, teeth, glass, and gravel. Food, chicken, or fish bones are radiolucent, and of intermediate lucency are plastic and wooden objects. Because barium esophagography poses an aspiration risk and may compromise subsequent endoscopy, it is advisable to consult with a gastroenterologist before completing the study. 7 Alternate imaging modalities to detect radiolucent objects include ultrasound, CT scan, or magnetic resonance imaging. In the setting of high clinical suspicion and a negative radiograph, proceeding to endoscopic evaluation may be of benefit. 8
Once the diagnosis of foreign body ingestion is made, the next decision is whether to remove the object or to manage conservatively. Ingested objects most commonly cause proximal obstruction, particularly at the level of the cricopharyngeal muscle in the esophagus; distal obstruction occurs in less than 10% of the cases. Although it is recommended that all esophageal foreign bodies be endoscopically removed, it is less clear for foreign bodies of the small bowel. Objects wider than 2.5 cm rarely pass the pylorus, especially in younger children, whereas objects more than 6 cm in length are unlikely to pass the duodenal sweep or ileocecal valve. 8
Objects at high risk for causing serious morbidity (Table 1) should be considered for early removal, particularly if still within endoscopic reach.1–3,9 Once in the stomach, most foreign bodies will pass within 4 to 6 days but may take as long as 4 weeks. 7 Children with foreign bodies obstructing the small bowel may present with vague symptoms such as vomiting, feeding intolerance, and obstipation (as in this case) and require surgical intervention. 2
High-risk objects and associated complications.

Although coins are the most common foreign body ingested, they rarely cause complications once past the esophagus. Intestinal foreign bodies of particular concern include objects that may change size, sharp objects, batteries, and magnets, which may require urgent intervention (Table 1).1,3
Water-storing gel beads may expand to several times their original size when submerged, with similar expansion on ingestion leading to bowel obstruction.4,10,11 One case report described whole bowel irrigation as successful treatment for a patient who ingested approximately 100 expanding water beads. 11 Another case report involved a single expanding water ball that required exploratory laparotomy and enterotomy. 4
If the ingested object’s advancing end is sharp, there is a higher risk of perforation. Still, many sharp objects pass through the small bowel without adverse complications. 7 The pylorus, ligament of Treitz, ileocecal valve, and rectosigmoid junction are at risk for perforation when sharp objects become affected in these anatomically narrowed areas.12,13 In patients with prior abdominal operations and resultant adhesions or strictures related to inflammatory bowel disease, a foreign body is more likely to become affected at these sites. Ingested toothpicks and bone have a high rate of perforation and commonly require surgical removal. 8 Sharp shell nuts and seeds more frequently cause intestinal perforation in young children. 14
Asymptomatic patients being managed conservatively for known sharp foreign body ingestion should be monitored as inpatients with daily abdominal radiographs. Surgical removal should be considered for symptomatic patients and those whose foreign bodies that have not advanced after 3 days. Intestinal perforation presents most frequently as abdominal pain; other symptoms include anorexia, nausea and vomiting, fever, and abdominal distension; less common symptoms include hemorrhage, bowel obstruction, and ureteric colic. 14
It is well established that button batteries within the esophagus require emergent removal as they can cause severe burns, tissue necrosis, and perforations due to the battery’s ability to generate an external current that results in lysis of adjacent tissue.2,9 This may result in delayed stricture and fistula formation, with aortoesophageal fistulas resulting in life-threatening exsanguination. Lithium ion batteries are especially dangerous because they conduct more current and produce hydroxide radicals that cause severe mucosal burns. 9 There is also increased risk with new batteries, those ≥20 mm in diameter, multiple battery ingestions, and age <5 years.
Once the battery has reached the stomach and beyond, the indications for removal become less convincing as it will typically pass through the GI tract without further complications. Progress through the intestines can be monitored with an abdominal radiograph every 3 to 4 days, as most are eliminated within 72 hours once past the duodenum. Even if the battery has passed into the small bowel, high-risk patients may still need to be evaluated for esophageal injury.8,15
Magnetic objects within the bowel are another special consideration, as the attractive forces between 2 or more magnets in adjacent loops of bowel can trap the bowel wall, causing mucosal injury that may progress to necrosis, fistula formation, perforation, and peritonitis. If there is evidence of multiple magnets, or a magnet co-ingested with a battery or other metallic object, the objects should be urgently removed. When conservative management is chosen, direct patient observation in a controlled setting is crucial to avoid serious morbidity.8,15
Removal of small bowel foreign bodies can be performed endoscopically or with open surgical procedure. 2 Endoscopy has been successfully performed with duodenal foreign bodies if there is no perforation, the object can be manipulated, it is located proximal to the inferior duodenal flexure, and it is less than 10-cm long. 16 It is rare to require exploratory laparotomy for ingested foreign body removal.
In conclusion, although some intestinal foreign bodies can be managed with observation, other high-risk objects may require urgent or emergent removal. Because patient presentation may range widely from nonspecific vomiting to life-threatening bowel obstruction and perforation, health care providers must maintain a high level of clinical suspicion for ingested foreign bodies.
Footnotes
Peer review:
Five peer reviewers contributed to the peer review report. Reviewers’ reports totaled 610 words, excluding any confidential comments to the academic editor.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
VB and HC provided care for the patient. VB wrote the first draft of the manuscript. VB, MV, and HC participated in manuscript development. All authors reviewed and approved the final manuscript.