
Abstract
Background:
Association between secundum Atrial Septal Defect (ASD) and mitral valve (MV) disease has been recognized for decades. Secundum ASD closure can reduce mitral regurgitation (MR) degree. However, in some patients, deterioration of MR after ASD closure has been observed. We aimed to identify the risk factors of MR deterioration after ASD closure.
Methods:
This was an observational retrospective cohort study. Data were collected from the registry and echocardiogram report. We evaluated all patients with ASD closure by surgery and transcatheterization without MR intervention from January 2012 until June 2021 at Dr. Sardjito General Hospital, Yogyakarta. We excluded patients with multiple ASD and ASD with severe MR requiring MV intervention. Risk factors for MR deterioration were evaluated using multivariate logistic regression.
Results:
A total of 242 patients who underwent post-secundum ASD closure were included. In multivariate analysis, ASD closure by surgery, large left atrial (LA) diameter (>40 mm), low left ventricular ejection fraction (LVEF; <55%), and MV regurgitation degree were significant risk factors for MR worsening after ASD closure, with OR of 2.103 (95% CI 1.124-3.937); 2.871 (95% CI 1.032-7.985); 5.531 (95% CI 1.368-22.366); and 2.490 (95% CI 1.339-4.630) respectively.
Conclusion:
ASD closure by surgery, large LA diameter (>40 mm), low LVEF (<55%), and MV regurgitation degree are independent significant risk factors for MR deterioration in post-secundum ASD closure patients. In adult ASD patients with reduced LV function, it is recommended to perform balloon testing and consider fenestrated closure, as low LVEF <55% has the highest risk of causing new or deteriorating MR.
Introduction
Atrial Septal Defect (ASD) is the most frequent congenital heart disease found in adults. 1 ASD is a congenital heart disease that causes Right Ventricle (RV) volume overload and decreased Left Ventricle (LV) blood volume. 2 These conditions affect the interventricular septum (IVS) position. Mitral Regurgitation (MR) was found in less than 10% of ASD patients. ASD closure induces right ventricle remodeling and could reverse left ventricle geometry, consequently worsening MR. ASD closure without MR intervention (repair or replacement) could improve the MR; therefore, in ASD patients with mild MR, isolated ASD closure could improve the MR.3,4 Here, worsening or new MR post-ASD closure is found in some cases.
A correlation between Secundum ASD and MV changes is already known. Several studies have shown a high incidence (37%–70%) of MV prolapse in ASD patients. 4 Changes in LV geometry in ASD show a correlation with the extent of MV prolapse. MV prolapse due to ASD is a risk factor for the development of MR in ASD patients. 5 RV chronic dilatation caused by RV volume overload shifts the position of IVS to the left, affecting the LV geometry, including mitral annulus, therefore, the MV prolapse could develop. ASD closure can restore LV volume and flow to normal, resulting in a stretched mitral annulus, which causes MV prolapse to repair, thus improving MR severity. 6
However, not all ASD closure may attenuate MR degree. Chronic RV dilatation resulting from RV volume overload can cause a shift in the position of the interventricular septum (IVS) to the left, leading to a “D-shaped” left ventricle (LV D shape), affecting the LV geometry including the mitral annulus, shortening of papillary muscle, and chordae tendineae. Closure of ASD restores normal volume distribution between RV and LV. A relatively small LV volume may not be adequately prepared to handle normal blood volume. ASD closure can cause stretching of the LV geometry, including the mitral annulus. This stretching can lead to new or worsened MR due to MV leaflet non-coaptation. 7 Therefore, this study aims to identify the risk factors for changes in MV characteristics after ASD closure. Hence, the need for MR intervention in patients with ASD closure could be decided based on evidence and careful evaluation of the individual patient’s condition.
Methods
Ethics approval and consent to participate
The Ethical Committee approved the study of the Faculty of Medicine, Public Health and Nursing, Universitas Gadjah Mada KE/FK1189/EC 2 November 2021. The research has been performed under the Declaration of Helsinki 2013.
Data collections
This study design is an observational retrospective cohort. Adult patients with secundum ASD are enrolled in the COngenital HeART Disease in Adults and Pulmonary Hypertension (COHARD-PH) registry, presented in Dr. Sardjito Hospital, Yogyakarta, Indonesia from July 2012 until July 2021. Patients’ baseline parameters, including demographic and clinical data, were gathered. We recorded pre-ASD closure data such as age at the closure intervention (surgery or transcatheter), gender, and atrial arrhythmia (eg, flutter or fibrillation). MR was evaluated using transthoracic echocardiography. We evaluated all patients with ASD closure by surgery and transcatheterization without MR intervention. We excluded the diagnosis of multiple or complex ASD and ASD patients with severe MR who require MV intervention.
Echocardiographic evaluation
Comprehensive echocardiography was conducted preoperatively and postoperatively. The grading of MR pre and post-ASD closure was classified quantitatively as none, mild, moderate, or severe. The classification mentioned follows the source from Grading of MR Severity by Echocardiography, as outlined in the Recommendations for Noninvasive Evaluation of Native Valvular Regurgitation, published in the Journal of the American College of Cardiology. 8 Deterioration of MR is defined as an increase of 2 or more degrees of MR after ASD closure. No deterioration of MR is defined as no increase in the degree of MR or an increase of only 1 degree of MR after ASD closure. ASD diameters (defined as large ASD if >2 cm), Tricuspid Regurgitation (TR) Velocity (high if >2.8 m/s), RV diameters (dilated if >40 mm), any LV D shape, any MV prolapse, LA diameter (dilated if > 40 mm), LVEF (low if <55%), Tricuspid annular plane systolic excursion (TAPSE, low if <17 mm), Left ventricular internal diameter end diastole (LVIDd, high if >52 mm), and tricuspid repair during the surgery. RV diameter was calculated by measuring the basal diameter at the end-diastolic in the apical 4-chamber view. The quantitative echocardiographic parameters with specific cut-off values are determined based on the guidelines provided in Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. 9 We evaluated the MR status after ASD closure within 6 months after ASD closure (depending on the existing data).
Statistical analysis
The data was subjected to observational retrospective cohort study analysis. The continuous data were displayed as mean and standard deviation (SD) or median and interquartile range (IQR) after being evaluated with the Shapiro Wilk or Kolmogorov Smirnov tests for the normality tests. A bivariate analysis was performed to assessed the independent predictors that significantly worsened MR progression. Depending on the type of data, the comparison between 2 groups were done using bivariate analysis Student T test or Chi-square test. The predictors with P value <.25 were considered to run a multivariate analysis with logistic regression. The P value <.05 were considered statistically significant. The statistical analysis was performed by using IBM SPSS 21 software package.
Results
From January 2012 until June 2021, we registered 1040 patients with ASD during this study; 878 patients were secundum ASD. Of the 358 patients underwent ASD closure, 180 were closure by surgery and other 178 were closure by device. After data cleaning, 242 patients post ASD closure were divided into 2 groups. The first group consist of patients with no MR deterioration (n = 180), and the second with MR deterioration (n = 62), as shown in Figure 1.
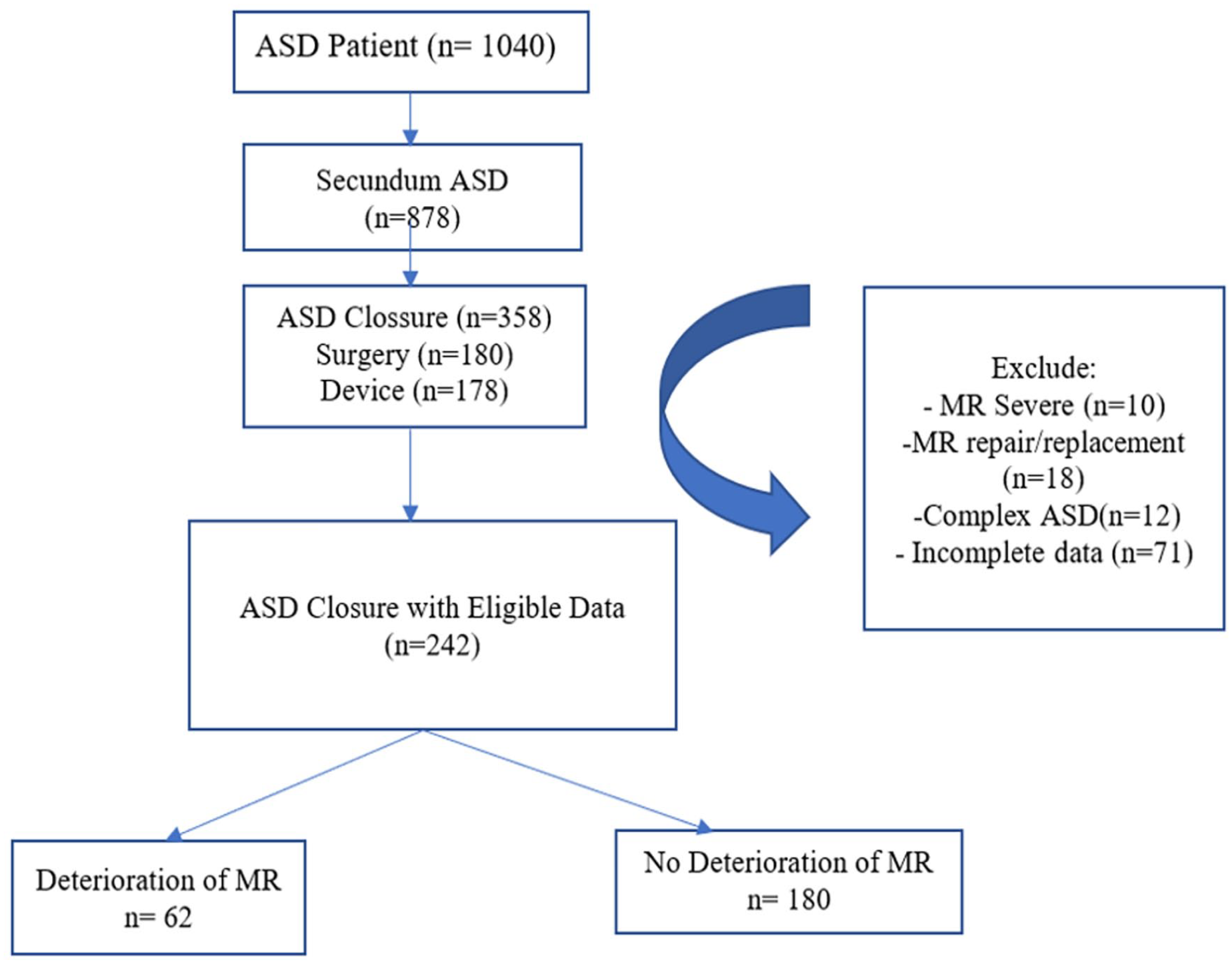
The flowchart of patient enrollment. Total subjects that eligible in this study were 242 and divided into groups with and without MR deterioration. No deterioration of MR defined as no increase degree of MR or an increase of only 1 degree of MR after ASD closure.
The clinical characteristic of the patients are shown in Table 1. We analyzed the variable that was suggested as a risk factors and confounding factor. On bivariate analysis (Table 2), large ASD diameter, large LA diameter, low LVEF, closure by surgery, and MV regurgitation included as a risk factors of MR deterioration with RR consecutively 1.566 (95% CI: 0.853-2.873), 1.885 (95% CI; 1.100-3.230), 4.355 (95% CI; 1.271-14.926), 1.587 (95% CI; 1.013-2.488), 2.115 (95% CI; 1.252-3.572) consecutively, and P value <.25. On the contrary, mitral valve prolapse are protective factor with RR 0.654 (95% CI: 0.365-1.172) and P-value .136.
Baseline characteristic of 242 adults patients with atrial septal defects.

Abbreviations: ASD, Atrial septal defect; LA, Left atrial; LV, Left ventricle; LVEF, Left ventricular ejection fraction; LVIDd, Left ventricular internal diameter end diastole; MR, Mitral regurgitation; RV, Right ventricle; TAPSE, Tricuspid annular plane systolic excursion; TR V, Tricuspid regurgitation velocity.
Bivariate analysis.

Abbreviations: ASD, Atrial septal defect; LA, Left atrial; LV, Left ventricle; LVEF, Left ventricular ejection fraction; LVIDd, Left ventricular internal diameter end diastole; RV, Right ventricle; TAPSE, Tricuspid annular plane systolic excursion; TR V, Tricuspid regurgitation velocity.
Sex as confounding factors (Table 3) suspected did not show significant relationship with MR deterioration (P-value .839). Risk factors with a P-value below .25 will proceed to multivariate logistic regression analysis. This study identified closure by surgery, LA diameter >40 mm, Low LVEF (<55%), and MV regurgitation were significant risk factors of MR deterioration after ASD closure patients, with OR consecutively 2.103 (95% CI 1.124-3.937) P-value .02; 2.871 (95% CI 1.032-7.985) P-value .043; 5.531 (95% CI 1.368-22.366); and OR 2.490 (95% CI 1.339-4.630), as shown in Table 4.
Confounding factor bivariate analysis.

Multivariate analysis logistic regression.

Abbreviations: LA, Left atrial; LVEF, Left ventricular ejection fraction; MV, Mitral valve.
Discussion
The correlation between atrial septal defect (ASD) and mitral regurgitation (MR) has been studied and described previously.3,10-13 However, to our knowledge, the study to examine MR changes and its risk factors remains limited. In this study, we examined 242 post-ASD closure patients. We analyzed several variables that have been proposed as risk factors for MV deterioration after ASD closure.
The first significant risk factor in our study is ASD closure by surgery. In our study, closure by surgery parameter is a significant predictor of MR deterioration ASD closure with OR 2.103 (95% CI 1.124-3.937), and P-value .02. In this study, 31.2% of patients undergoing surgery were experiencing MR worsening, compared to patients who underwent transcatheter closure (19.7%). In contrast, another study from Toyono, et al (2008) showed improvement of MR in (3 of 5) patients with ASD closured by surgery without MV surgery (P < .05). 10 In this study, from 125 patients who underwent surgery, 42 (33.6 %) patients had tricuspid repair (eg, tricuspid annuloplasty and De Vega procedures). This is similar to Park et al (2011) study that identified an association between tricuspid valve repair and deterioration of MR in older age (OR 1.058; 95% CI 1.025-1.092, P = .0005). 11 Corrective procedures for TR can pull on the mitral annulus and may cause new onset or MR exacerbation. Therefore, compared to transcatheter closure, surgery had worse remodeling conditions.
The second significant risk factor in our study is the large LA diameter. A large LA diameter is a significant risk factor for MR deterioration, with a cut-off >40 mm increasing the risk by 2.871 times than small LA diameter (<40 mm), with a P-value of .043. It is evident in 45% of ASD patients with deterioration of MR. This finding is similar to Nishimura, et al (2017) who proposed LA dilatation (>40 mm) as an aggravating factor of MR after ASD closure with P = .007. 3 Large LA size indicates MR chronicity prior to surgery. As the LA is dilated, the posterior wall extends behind the posterior basal wall of the left ventricle, and the posterior annulus is displaced into the crest of the left ventricular inlet. Therefore, the posterior mitral leaflet will be retracted to the posterior wall of the left ventricle. Dilatation and retraction of the mitral annular of the posterior mitral leaflet can lead to poor coaptation of the mitral leaflet and result in MR deterioration. 14
Another significant risk factor in this study is low LVEF. The accepted cut off value for low LVEF was <55%. A low LVEF indicates reduced pumping ability of the left ventricle. This can lead to an accumulation of blood in left ventricle which could result in diastolic dysfunction and increase the end-diastolic volume of left ventricle. 15 In our study, this parameter presents in 6 (60%) patients with MR deterioration after ASD closure, with the highest OR of 5.531 (95% CI 1.368-22.366) among all parameters in multivariate analysis. The study of left ventricular dysfunction after ASD closure is well established13,16, however the study on MR aggravation caused by ASD closure in low LVEF pre-operative patients is still limited. In this study, both univariate and multivariate analyses demonstated significant results of low LVEF as independent risk factor for MR worsening after ASD closure with P values of .011 and .016, respectively. Closure of an ASD may result to an abundant volume of left ventricular preload, potentially overburden the ventricle while its pumping function is already compromised. Therefore, can lead to left atrial volume overload. 17 The combination of left ventricular dysfunction, increased left atrial volume, and altered hemodynamics after ASD closure can collectively contribute to the deterioration or new onset of mitral regurgitation.
In our population, the degree of MR is one of the risk factors in deterioration of MR in ASD closure patients. MV regurgitation has been attributed to abnormal left ventricle geometry in response to right ventricular dilatation. 13 Our study identified that this parameter had OR 2.490 (95% CI 1.339-4.630) with a P value of .004. This finding supported the data from Lee, et al. (2019) who showed significant changes in degree of MR after surgery (P < .001). 12 Another previous study reported that 82 of 286 (29%) adult ASD patients who underwent surgery showed deterioration or new onset of MR, including 18 patients whose MR degree increased by grade 2 or more. 11 Moreover, Yoshida et al. reported 16.2% and 10.8% of patients experienced an increased degree of MR one grade and 2 or more grades after ASD closure, respectively. 18
Conclusion
ASD closure by surgery, Large LA diameter (>40 mm), low LVEF (<55%), and MV regurgitation degree are the independent significant risk factors of MR deterioration in post-secundum ASD closure patients. In adult ASD patients with reduced LV function, it is recommended to perform balloon testing and consider fenestrated closure, as low LVEF <55% has the highest risk of causing new or deteriorating MR.
Footnotes
Acknowledgements
We are very grateful to the patients and their families for participation in this research study. Authors express gratitude to the following persons: Muhammad Reyhan Hadwiono, MD, Andreas Hartanto Santoso, MD, Abdul Majid Halim, MD, for their contribution in data management and collection. We also express gratitude to Erik Christopher and Athanasius Wrin Hudoyo, MD, PhD who corrected the manuscript grammar. We acknowledge Dr.Sardjito Hospital for patient registration support.
Author Contribution
The study was conceived by GS, IA, CEC, and LKD. GS prepared the manuscript, CEC performed data analysis and write manuscript & LKD provided critical revisions for important intellectual content. All project-related tasks were facilitated by GS, IA, and LKD. Each author has reviewed and approved the text and agreed to be responsible for all parts of the work, including ensuring that any concerns about the accuracy or integrity of any portion of the work are thoroughly investigated and resolved
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Universitas Gadjah Mada (Rekognisi Tugas Akhir [RTA] 2021 to LKD number: 3190/UN1/DITLIT/DIT-LIT/PT/2021).