
Abstract
The clinical features of severe hypothyroidism vary in presentation, ranging from subclinical symptoms to multiorgan failure referred to as myxedema coma. The cornerstone treatments of myxedema coma include aggressive thyroid hormone replacement combined with excellent supportive care in the intensive care unit. We report a rare case of a 56-year-old female with history of hypothyroidism treated with levothyroxine, who developed myxedema coma post-pericardial window surgery for a large pericardial effusion. She was supported with substantial doses of vasopressors and inotropes for shock. In addition, she was initiated on lung-protection ventilation for acute respiratory distress syndrome. After the diagnosis of myxedema coma was made, she was started on intravenous levothyroxine and hydrocortisone with great sustained clinical response. This case illustrated myxedema coma as an unusual cause of shock in post-operative patients with past medical history of hypothyroidism.
Keywords
Introduction
Hypothyroidism is an established cause of pericardial effusion, which can decompensate and lead to life-threatening cardiac tamponade. 1 Hypothyroidism related pericardial effusion is thought due to increased permeability of the epicardial vessels and decreased lymphatic drainage of albumin, leading to fluid accumulation in the pericardial space. 2 Although small effusion is a frequent occurrence, moderate and large effusion with tamponade physiology can also occur and is associated with severe form of the disease, such as myxedema coma. 3 Myxedema coma is a rare and life-threatening condition of decompensated hypothyroidism and has more than 50% mortality rate if left untreated. 4 It is characterized by collapse of metabolism and development of shock due to critical thyroid hormone deficiency. 5 Factors that precipitate this crisis include infections and discontinuation of thyroid supplements among other uncommon causes. 6
Myxedema coma is even more rare in the perioperative setting with only 8 reported cases in literature.7-14 Herein, we describe a case of acute onset myxedema coma as the etiology of shock post pericardial window procedure.
Case Presentation
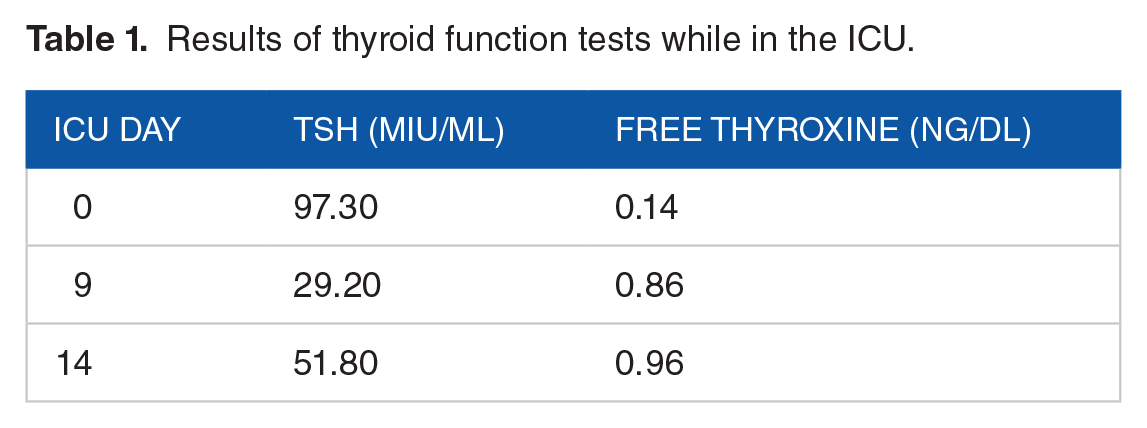
A 56-year-old female with past medical history of multiple strokes with no residual deficits, essential hypertension, obstructive sleep apnea, hypothyroidism on daily levothyroxine 150 mcg, chronic obstructive pulmonary disease on 3 L of home oxygen, and coronary artery disease with 6 stents, presented to the emergency department with 4 days of non-productive cough, shortness of breath and worsening substernal chest pain. Her vitals were: temperature 35°C, blood pressure 132/87 mmHg, heart rate 84 beats per minute, and oxygen saturation 97% on 5 L via nasal cannula. Arterial blood gas (ABG) was as follows: pH of 7.17, pCO2 92, pO2 69, and HCO3 33. Her physical exam was pertinent for wheezing in the bilateral lower lung lobes, regular heart rate and rhythm and non-pitting, edematous bilateral lower extremities. Electrocardiogram showed low-voltage, normal sinus rhythm with first degree block and PR interval at 210 ms (Figure 1). Her chest computed tomography angiogram showed an enlarged heart with a moderate sized pericardial effusion measuring 2 cm in diameter (Figure 2). Her pertinent positive labs included: NT-pro BNP 426 pg/mL, TSH 97.30 mIU/mL, and fT 40.14 ng/dL (Table 1).

EKG on admission showing sinus rhythm with first degree AV block and low voltage QRS.

CT scan showing pericardial effusion.
Results of thyroid function tests while in the ICU.
An emergent transthoracic echocardiogram (TTE) demonstrated left ventricular ejection fraction of 55% to 60%, and a large circumferential pericardial effusion was present without hemodynamic compromise (Figure 3). Given the patient’s worsening pulmonary symptoms and impaired gas exchange measured on ABG, cardiothoracic surgery decided to create pericardial window emergently in the operating room.
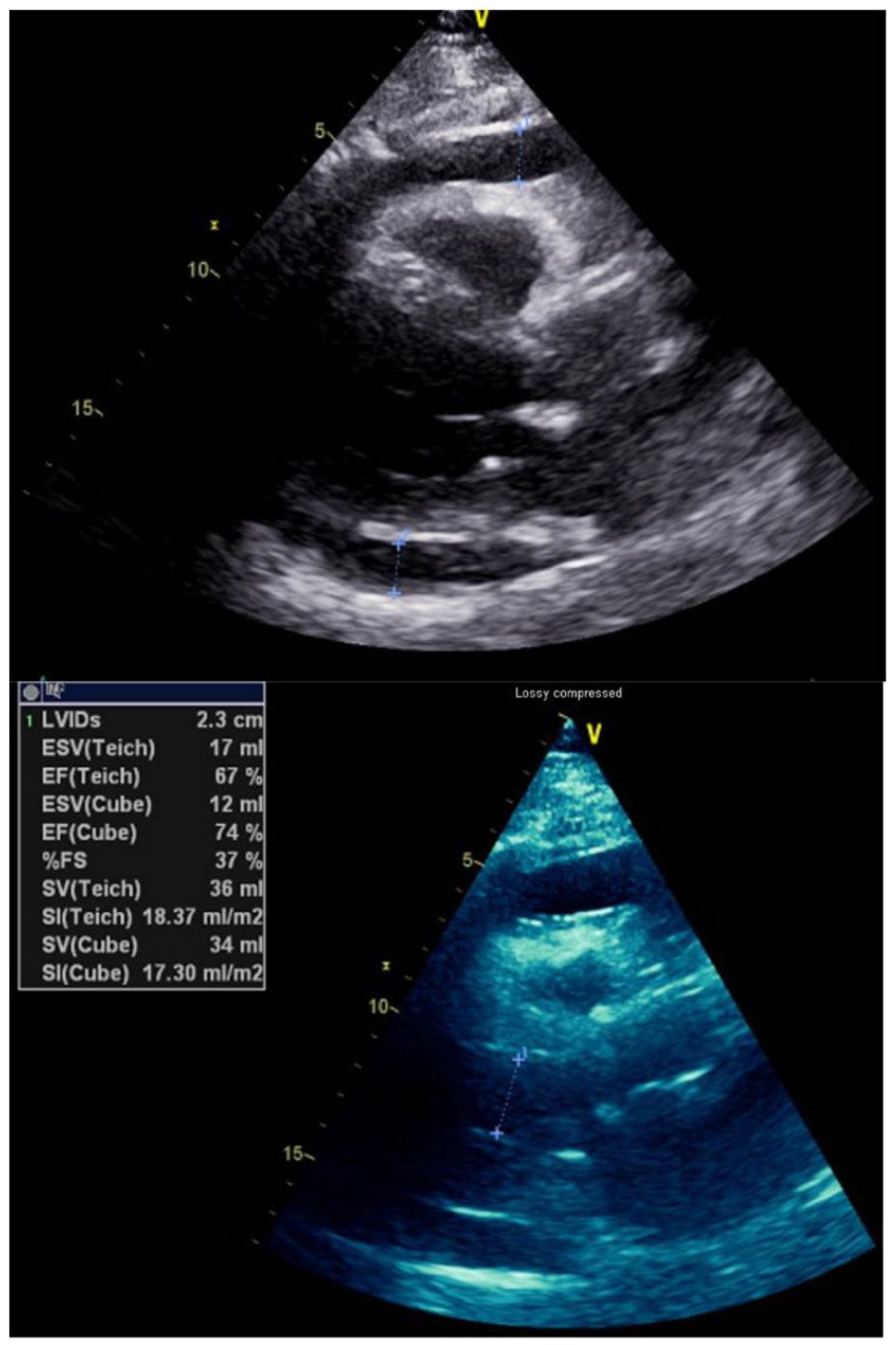
Transthoracic echocardiogram showing pericardial effusion circumferential to the heart.
Prior to induction, the patient did not require hemodynamic support with vasoactive medications. However, her respiratory status was severely compromised, on high flow nasal cannula at 100% FiO2 and 60 L/min, with sPO2 of 89%. An arterial line was placed for continuous hemodynamic monitoring, and the patient was induced with lidocaine, fentanyl, propofol, and rocuronium and intubated without difficulty. She remained hemodynamically stable throughout the procedure but required 100% FiO2 and PEEP of 10 to maintain her oxygen saturation in the low 90%. The patient’s intra-operative transesophageal echocardiogram (TEE), interpreted by her anesthesiologist, redemonstrated a large pericardial effusion with signs of early tamponade physiology. The surgeon performed the pericardial window procedure without difficulty and drained approximately 800cc of straw-colored fluid without evidence of hemorrhage or infection from the pericardium. Post-intervention TEE exam confirmed complete evacuation of the effusion and normal bi-ventricular functions. The surgeon placed a pericardial drain and the incision was closed uneventfully.
Our patient’s first few hours post-operatively in the intensive care unit were challenged with significant hemodynamic instability requiring multiple vasoactive medications including epinephrine, milrinone, vasopressin, and norepinephrine, and severe acute respiratory distress syndrome requiring 100% FiO2 and 15 PEEP. An emergent bedside TTE performed did not reveal any new shunt physiology or other structural cardiac abnormalities.
Postoperative vital signs were as follows: temperature was 36.1°C, blood pressure 89/55 mmHg with multiple vasoactive medications, heart rate of 59/minute, and saturation 90% with the above-mentioned ventilator setting. On exam, she was noted to have non-pitting peripheral edema in her face and periphery. Her preoperative laboratory findings were reviewed, and myxedema coma was thought to be the culprit for her decompensation. Endocrinology was consulted, and she was treated with intravenous T4 and corticosteroid. Over the next 48 hours, the patient made drastic clinical improvement with no vasopressor support and minimal ventilator setting. Of note, workup of her pericardial fluid was negative for rheumatological or viral etiologies. Our patient was eventually weaned off the ventilator and discharged home.
Discussion
A deficiency in thyroid hormone can disrupt the body’s metabolic processes and affect all organ systems. Myxedema coma is characterized as an extreme manifestation of hypothyroidism leading to decreased mental status, hypothermia and multiorgan failure. 15 It is extremely rare, with only a few reports in the literature, likely due to earlier diagnosis given the availability of thyroid hormone function tests. Myxedema coma is a complication of severe hypothyroidism occurring as a natural progression of the disease, even with adequate thyroid hormone replacement. It can also be secondarily precipitated by an acute stress event in a poorly controlled hypothyroid patient, such as infection, cold exposure, and surgery. 16
It was evident from our patient’s clinical profile that she had long-standing hypothyroidism. It was after she was subjected to a stressful situation, the pericardial window surgery, that led to her acute and rapid development of myxedema coma. In this disease state, low intracellular T3 led to hypothermia and suppression of cardiac function. 5 Decreased sensitivity to hypoxia and hypercapnia within the central nervous system contribute to respiratory failure. 5 In addition, altered vascular permeability from myxedema coma also played a role in her acute respiratory distress syndrome. Our patient’s acutely increased metabolic demand post-operatively was not met due to pre-operative severe hypothyroidism. 17 Therefore, shock and multiple organ failure ensued. Once the diagnosis was promptly and accurately identified, treatment consisted of thyroid and steroid replacement therapy produced significant clinical response highlighted by resolution of shock and organ failure.
Thyroid function test can show distinctly elevated TSH and low thyroxine and triiodothyronine levels. It can change drastically in patients undergoing major surgery. For the majority of patients, the decrease in postoperative free triiodothyronine and thyroxine concentrations bears no pathophysiologic consequences. For our patient, the severe hypothyroid state after cardiac surgery led to a life-threatening medical emergency. 18
Comprehensive support therapy, including mechanical ventilation, vasoactive medications, and intravenous fluid, are pivotal in preserving end-organ function. However, significant clinical improvement was not seen until hormone replacement was initiated. Our patient received intravenous 200 µg/day T4 and 100 mg Q8H hydrocortisone in the acute phase of her illness. A standard thyroid replacement medication and dosage remain controversial with the consensus of most endocrinologists recommending an initial dose of 200 to 500 µg/day of IV levothyroxine. 19 Lastly, myxedema coma is associated with adrenal insufficiency and the addition of steroid therapy is recommended in patients presenting with severe hypothyroidism during acute stress. 20
Conclusion
Hypothyroidism and pericardial effusion are commonly benign, yet they can progress to myxedema coma and cardiac tamponade in severe cases. We recommend performing thyroid testing in critically ill patients with hypothyroidism. If stress factors are identified in such patients, the diagnosis of myxedema coma in anyone with shock and multiple organ failure should be considered. Prompt treatment with thyroid hormone replacement and diligent supportive therapy following the diagnosis of myxedema coma can reduce mortality and morbidity.
Footnotes
Acknowledgements
None.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported (in whole or in part) by HCA Healthcare and/or an HCA Healthcare affiliated entity. The views expressed in this publication represent those of the author(s) and do not necessarily represent the official views of HCA Healthcare or any of its affiliated entities.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contribution
All authors drafted the article, revised the content, and approved the current version to be published.
Ethics Approval
Our institution did not require ethical approval for reporting individual cases or case series.
Informed Consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.