
Abstract
A 3-year-old boy was referred to our hospital for management of Kawasaki disease at 5 days of illness. Echocardiographic examination on admission suggested aneurysmal dilation of the right coronary artery and a possible aorta-left main trunk connection. However, detailed echocardiography at 12 days of illness revealed an abnormal bifurcation of the proximal right coronary artery and no real connection of the aorta-left main trunk, all of which indicated the presence of a single right coronary artery. These diagnoses were confirmed by selective coronary angiography, which was performed later. Considering the difficulties in diagnosing congenital coronary anomalies, which may increase the risk of future fatal events, knowing the disease entity of the congenital coronary arterial anomaly is important for the accurate evaluation of coronary arteries in patients with Kawasaki disease. To the best of our knowledge, this is the first case report of a patient with Kawasaki disease complicated by a single right coronary artery; however, following a search of the literature, we found a brief conference abstract written in Japanese relating to the same clinical condition.
Introduction
Kawasaki disease (KD) presents as systemic vasculitis of unknown origin. The main therapeutic goal in the treatment of KD is to avoid the development of coronary arterial lesions, such as coronary arterial dilation and aneurysm. Echocardiography is a key diagnostic and monitoring tool for the evaluation of the coronary arteries in KD. However, the evaluation of coronary arteries by echocardiography is sometimes difficult because children with KD are highly irritable and because their coronary artery system might have unknown congenital anomalies.1,2 Herein, we report a case of KD in which diagnosis was complicated by the presence of a single right coronary artery.
Case report
A boy aged 2 years and 11 months was referred to our hospital with a fever that had persisted for 5 days, acute non-purulent cervical lymphadenopathy, bilateral conjunctival congestion, changes in the color of the lips and oral cavity, polymorphous exanthema, changes in the peripheral extremities, acute nonpurulent cervical lymphadenopathy, and redness at the Bacille Calmette-Guérin (BCG) inoculation site. His past and family histories were unremarkable. His body temperature, heart rate, and blood pressure were 38.3°C, 132 bpm, and 94/56 mmHg, respectively. Rapid tests of throat swabs for group A Streptococcus and adenovirus yielded negative results. Systemic inflammation was indicated by a white blood cell count of 9000 cells/μL, with 57% neutrophils, and a C-reactive protein (CRP) level of 6.4 mg/dL. Liver enzyme levels were within normal ranges. Based on these findings, we confirmed the diagnosis of KD. Echocardiography on admission showed normal wall motion, no valvular regurgitation, and no pericardial effusion. Mild dilation (3.2 mm) at the origin of the right coronary artery and small aneurysmal dilation of the right coronary artery (4.6 mm) were suspected (Figure 1A). Although the left main trunk wall was not clearly visible (Figure 1B), there appeared to be an aortic-left main trunk connection with no coronary arterial lesion in the left coronary artery. Consequently, we administered immunoglobulin (2 g/kg) and oral aspirin.

Echocardiography on admission: (A) apparent right coronary aneurysm and (B) apparent aortic-left main trunk connection with no dilation of the left coronary arteries.
However, echocardiography at 12 days of illness failed to show the origin of the left main trunk but showed mild dilation of the right coronary artery (4.2 mm) and an abnormal bifurcation at the proximal right coronary artery (Figure 2, arrow). At this stage, a single right coronary artery was suspected. The patient became afebrile on day 11 of illness and was discharged on day 13 of illness. He received aspirin for 2 months.
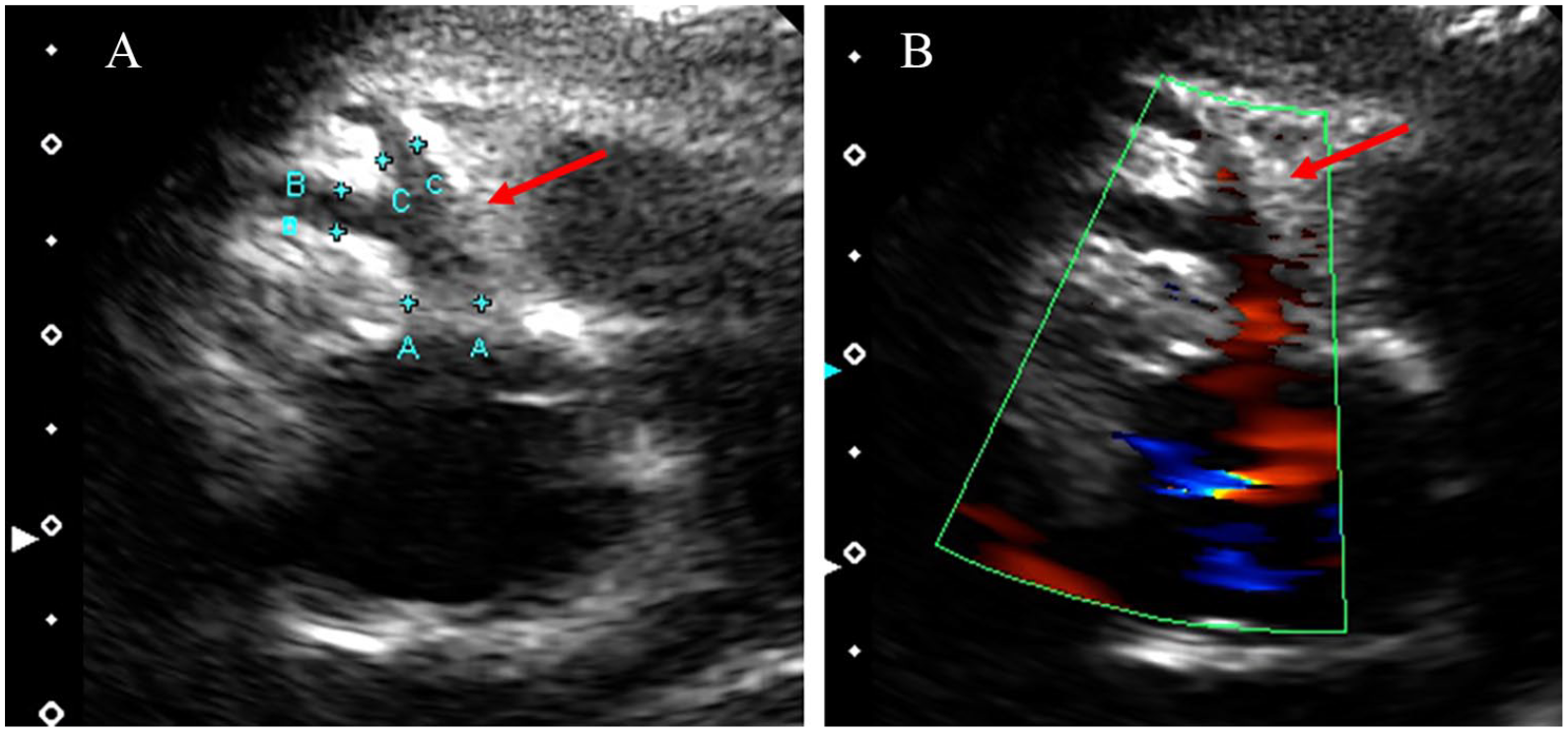
Echocardiography at 12 days of illness: (A and B) right coronary artery bifurcated at a very proximal position.
Aortography and selective coronary arteriography at 50 days of illness confirmed the diagnosis of a single right coronary artery with no dilation at the origin of the right coronary artery (3.2 mm) (Figure 3). The entire left coronary artery arises from the right coronary artery, and the transverse trunk passes anterior to the main pulmonary arteries. The coronary arterial pattern was classified as RII-A (the single coronary artery originates from the right sinus, and the transverse trunk passes anterior to the conus of the right ventricle or the main pulmonary artery) using the Lipton criteria. 3 Thereafter, no recurrence of KD or worsening of coronary arterial lesions was observed after the cessation of a two-month course of aspirin.

Selective right coronary angiography (A) anteroposterior and (B) lateral. The entire left coronary artery arises from the right coronary artery, and the transverse trunk (arrows) passes anterior to the main pulmonary arteries, classified as RII-A using the Lipton criteria. 3
Discussion
To the best of our knowledge, this is the first case report of a patient with Kawasaki disease complicated by a single right coronary artery; however, following a search of the literature, we found a brief conference abstract written in Japanese relating to Kawasaki disease complicated by a single right coronary artery. 4 In our patient, at the initial echocardiographic examination, there were 2 difficulties in accurately evaluating the coronary arteries: (1) no bifurcation of the right coronary artery was detected, and (2) it appeared as if there was an aorta-left main trunk connection in the ambiguous image. Given the difficulty of diagnosing coronary artery abnormalities, even with an aorta-left main trunk connection, this case highlights the importance of the knowledge that there could be congenital coronary anomalies in echocardiographic coronary evaluation.
Accurate diagnosis and evaluation of coronary arterial lesions, such as dilation and aneurysmal formation, are critically important for diagnosing KD, selecting the most appropriate acute KD therapies, and deciding the mode of follow-up. Coronary artery problems include KD-related coronary lesions and congenital coronary anomalies. However, the usual evaluation of coronary arteries is, in general, performed assuming that the coronary arteries do not have major congenital coronary abnormalities. Thus, without knowing the disease entity of congenital coronary artery anomalies, it would be quite difficult to accurately detect and interpret the existence of coronary artery anomalies. Figure 1 shows the original echocardiography image taken on admission, suggesting that the right coronary artery ran normally with a mild aneurysm formation and that there might be an aorta-left main trunk connection with no apparent dilation of the left main trunk.
Anomalous origin of the left coronary artery from the pulmonary artery (ALCAPA) is a congenital coronary anomaly that should be carefully ruled out because it cannot be completely excluded by echocardiography and because accurate diagnosis enables appropriate surgical repair and significantly improves prognosis. However, even in cases with a very clear appearance of an aorta-left main trunk connection on echocardiography, the aorta-left main trunk connection can be ruled out by angiography. 5 In the same way, one might expect our case to have an aorta-left main trunk connection in Figure 1 despite the absence of a real connection. We believe that the difficulty in detecting the connection, the ambiguous border of the left main trunk, and the awareness of the potential for a false diagnosis of the aorta-left main trunk connection could be key to correctly diagnosing the nonexistence of the aorta-left main trunk connection. Furthermore, in this case, another important point, the intention to pursue the distal coronary arteries, helped us detect the abnormal bifurcation of the right coronary artery (Figure 2). These findings support the echocardiographic diagnosis of single right coronary arteries and the absence of an aorta-left main trunk connection.
Single coronary arteries are rare, with a rate of 0.044%. 6 Moreover, there are other congenital coronary anomalies, 7 including abnormalities of the coronary orifice location, coronary arterial course, coronary vessels, and coronary artery terminations, as well as coronary ostial stenosis/atresia. Transthoracic echocardiographic screening revealed the incidence of any congenital coronary abnormality in 0.17% to 0.39% of asymptomatic subjects.8,9 Although those with congenital coronary anomalies are often asymptomatic and have a negative result on resting 12-lead electrocardiography, they have an increased risk of sudden cardiac death, which varies depending on the type of anomaly.10,11 Thus, congenital coronary anomalies, including single coronary arteries, should be recognized and evaluated to reduce the risk of a coronary event and avoid sudden cardiac death. The current patient has a single right coronary artery, which is associated with a higher risk of sudden death compared to having a single left coronary artery. 11 Despite the fact that there was no malignant pattern, such as a coronary artery between the 2 great arteries, we believe that this patient should be carefully monitored and evaluated using an exercise stress test because the long-term additional risk of KD and single coronary arteries remains unknown.
In conclusion, awareness of congenital coronary arterial anomalies (such as a single coronary artery) is important in the evaluation of coronary arteries in patients with KD. Computed tomography provides less invasive coronary arterial evaluation than angiography with limited radiation dose. 12 Thus, once such a lesion is suspected, further imaging evaluation such as angiography or computed tomography might be considered to definitely diagnose it and to appropriately manage the condition to reduce the risk of future coronary events.
Footnotes
Acknowledgements
We thank all the doctors and medical staff who were involved in the treatment of this patient.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
RN wrote the first draft of this manuscript. RN, HI, YI, MS, TM, ST, KM, and SM contributed to data collection and manuscript revision. YI, HI, and SM contributed to data interpretation and analysis. SM has made critical revisions and all authors approved the final manuscript. All authors reviewed and approved the final manuscript.
Ethical Approval
The requirement for ethical approval was waived by the ethical committee of the Saitama Medical Center of the Saitama Medical University.
Informed Consent
The parents of this infant gave written consent for the publication of this report.