
Abstract
Aortic valve replacement is the commonest cardiac surgical operation performed worldwide for infective endocarditis (IE). Long-term durability and avoidance of infection relapse are goals of the procedure. However, no detailed guidelines on prosthesis selection and surgical strategies guided by the comprehensive evaluation of the extension of the infection and its microbiological characteristics, clinical profile of the patient, and risk of infection recurrence are currently available. Conventional mechanical or stented xenografts are the preferred choice for localized aortic infection. However, in cases of complex IE with the involvement of the root or the aortomitral continuity, the use of homograft is suggested according to the surgeon and center experience. Homograft use should be counterbalanced against the risk of structural degeneration. Prosthetic bioroot or prosthetic valved conduit (mechanical and bioprosthetic) are also potentially suitable alternatives. Further development of preservation techniques enabling longer durability of allogenic substitutes is required. We evaluate the current evidence for the use of valve substitutes in aortic valve endocarditis and propose an evidence-based algorithm to guide the choice of therapy. We performed a systemic review to clarify the contemporary surgical management of aortic valve endocarditis.
Introduction
Aortic valve endocarditis (AVE) is the commonest infectious heart disease in adults, accounting for over half of 40 000 to 50 000 new cases of infective endocarditis (IE) annually in the United States alone. 1 IE is implicated in 20% of hospital deaths and up to 60% of patients who undergo surgery for prosthetic AVE develop complications due to the formation of root abscesses and valve dehiscence.1,2 Although infectious injury of one or more leaflets is the most common complication of native AVE, the extension of pathogens to other contiguous structures close to the aortic valve (AV) such as the aortic root, left ventricular outflow tract down to the mitral valve, called infectious aortopathy, is also present in approximately 64% of affected persons.3,4 Evidence to date suggests that the pattern of infectious disease in patients with aortic valve involvement is diverse, possibly reflecting the heterogeneity in age, sex, pathogens implicated, prosthetic valve endocarditis (PVE), alongside clinical and surgical features.1,2,5-7
Surgical treatment of aortic valve endocarditis today is generally performed using conventional mechanical and stented xenograft prosthesis or cryopreserved aortic homograft while aortic valve repair is limited to well-circumscribed infectious injuries.3,4,8-10 However, the literature does not provide sufficient data for a systematic approach to AVE operations due to the lack of randomized trials classified as Class Ia level A or B, which may guide the timing and choices of the ideal substitute for infectious aortic valve disease.8-13
We performed an analysis of several reports in which different surgical strategies were compared for the treatment of aortic valve endocarditis and its complications to overcome limitations of individual observational studies in detecting differences in clinical outcomes, beginning with our own experience of valve surgery. We subsequently discuss the current evidence for different surgical strategies and propose evidence-based algorithms to aid the decision-making process behind the most suitable substitute during aortic valve endocarditis operations.
The Clinical Manifestation and the Effect of Therapy
Anatomical consideration
In heart infections, the surgeon is confronted with the potentially complicated distortion of structures which may cause handling to be tricky. The aortic valve apparatus includes the valve leaflets, annulus, sinus of Valsalva with left and right coronary ostia, and sinotubular junction. These components are assembled in the aortic root which together constitute a sophisticated structure. The 3 aortic-valve leaflets, each semilunar in appearance, are located within a small dilatation of the proximal aorta linked with each cusp, called aortic sinuses or the sinuses of Valsalva. These are designated, in respect of the corresponding coronary ostia (left, right, and non-coronary sinuses). Each leaflet is connected to the wall of the aorta by the outward edges of its semicircular border, with the fixing extremity between each cusp named a commissure. 1.3% of the population worldwide have bicuspid aortic valves that typically consists of 2 unequally sized leaflets. 14 The aortic cusps insert on the circumference of the aortic annulus, is incongruous to the mitral annulus and the fibrous trigones.
Anatomically, the aorta is divided into the ascending aorta, which is approximately 5 cm in length with a diameter ranging between 20 to 37 mm, 15 aortic arch, thoracic aorta, and abdominal aorta. The ascending aorta includes the aortic root and the tubular portion that begins from the sinotubular junction in the aortic root and ends at the origin of the brachiocephalic or innominate artery. The competence of the aortic valve relies on the coordinated interaction of the aortic root apparatus. During diastole, the living dynamism of the aortic root prevents the valve leaflets from inverting into the left ventricle.
Methods
We designed a systematic review and conducted an electronic search of Pub Med, EMBASE, and Cochrane database from January 2001 to December 2019, using the terms “infective endocarditis,” “heart valve endocarditis,” “left side endocarditis,” “aortic valve endocarditis,” “heart valve prosthesis,” “allograft,” “autograft,” “aortic valve replacement,” and “aortic valve repair” was conducted. We assessed a large number of publications from 2001 16 (Table 1) and 2019 17 (Table 2) in patients who received the use of homograft, Ross operation, conventional mechanical, stented xenograft or stentless prosthesis or who received an aortic valve repair for infective aortic valve replacement. In detail, pertinent abstracts were reviewed and the related articles were examined. References for all selected studies were crosschecked. The lack of RCTs within this subject matter has refocused the present review on data from unmatched observational series, propensity-matched observational series, meta-analyses, registries, and editorials. Guidelines, professional society recommendations, registries, editorials, and prior systematic reviews were considered as additional references.
Observational studies and propensity matched comparing the allogenic and autologous substitute with conventional prosthesis.

# Propensity Score. * IVDU= intravenous drug user. Of total N = 436 Valve repair was performed in N = 45 ; χ Ao/Mitr-H = Cryopreserved mitro-aortic homograft replacement.
Systemic review, meta-analysis and registries reporting the use of aortic homograft, Ross operation, conventional prosthesis and aortic valve repair.
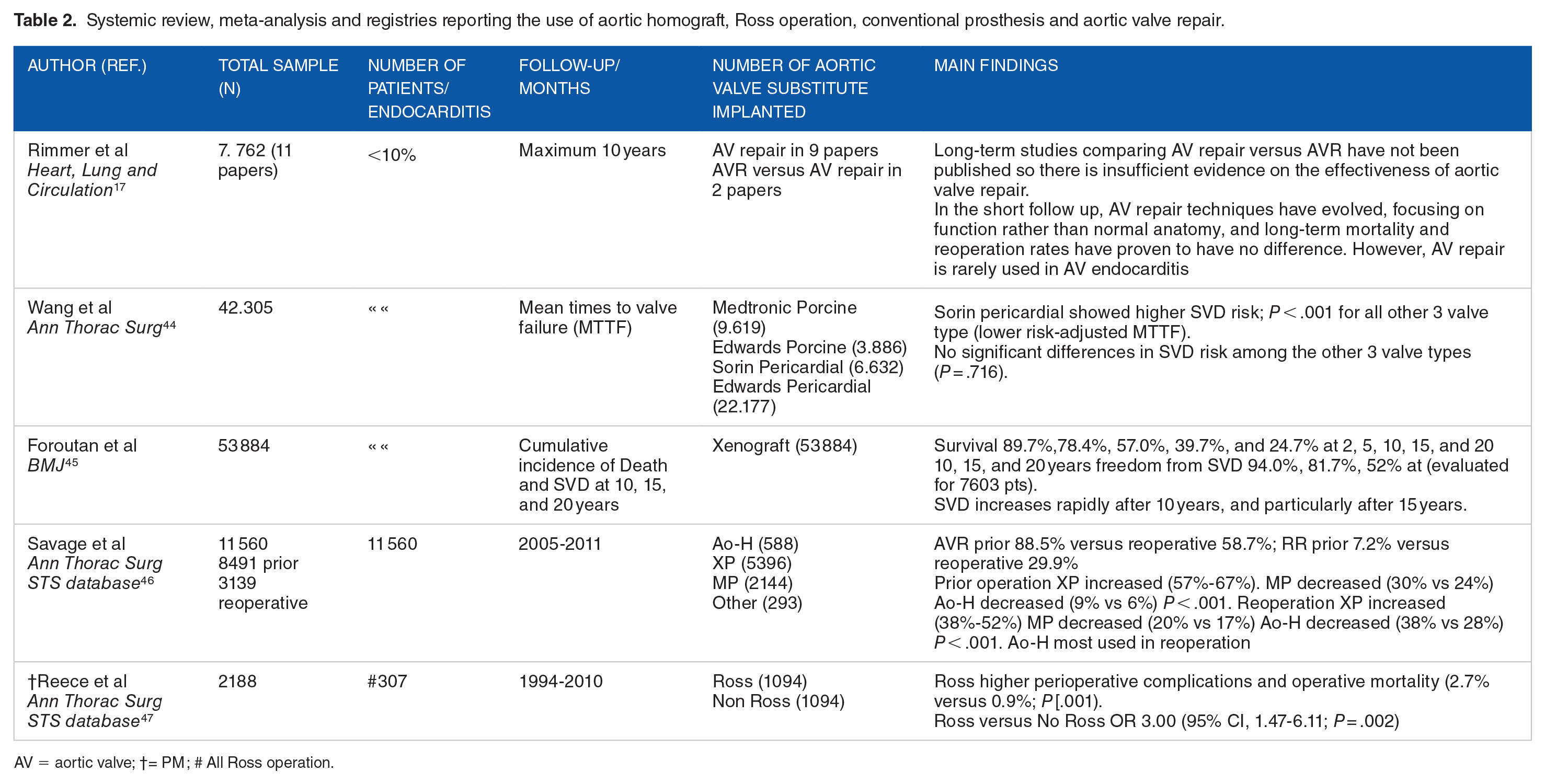
AV = aortic valve; †= PM ; # All Ross operation.
It is important to note that the weight of the evidence for the various substitutes for AVE was dissimilar. Unmatched observational series and propensity-matched series included around 4111 patients for xenograft prosthesis (XP), 2454 for aortic homograft (Ao-H), 665 for the mechanical prosthetic (MP), and a few hundred for Ross operations and aortic valve repairs (Tables 1 and 2; Figure 1).

PRISMA Diagram showing selection of observational studies, systematic reviews and meta-analysis included in study.
Pathophysiology
Microbiology
Although aortic-valve endocarditis is characterized predominantly by adhesion of pathogens to abnormal or damaged endothelium of leaflets and annulus alone, the involvement of the aortic root, ascending aorta and arch is possible. In fact, the normal endothelial lining of the heart is resistant to the adhesion of germs but and a defect in this resistance allows bacteria, especially gram-positive, to adhere to the damaged endothelium. The adhesion mechanism to the aortic endothelium is mediated by specific surface adhesins that are proteins dedicated in intercede with the attachment of proteins of the host extracellular matrix. This process is facilitated by fibrin and platelet microthrombi. 48
The particular aggressiveness of Gram-positive bacteria is also because they lack an external membrane but instead have a thick surrounding peptidoglycan; making them less sensitive to serum-induced killing. After the bacterial adhesion during colonization, bacterial proliferation cycles are associated with local thrombotic processes, recruitment of monocytes, and inflammation, leading to the formation of mature vegetation. 49 The production of a biofilm that is typical of many of the infectious microorganisms (including staphylococci, streptococci, and enterococci with other rarer pathogens, such as Candida species and Pseudomonas aeruginosa), allow bacterial incorporation into a polysaccharide extracellular slime-like matrix. The specificity of biofilms among other things favors cell-to-cell communication and synchronized gene expression that promotes the assembly and maturation of pathogens. Once arisen, the biofilm protects the bacteria from the host’s immune system, reduces antimicrobial efficacy, while shielding the organisms. The characteristics of the constituting biofilm are now recognized as a virulent trait in the development of infections related to the pathogenic staphylococcal species (Figure 2).

Show the percentage of cases of infective endocarditis caused by different microorganisms from a cohort of French population of 497 patients. From Selton-Suty et al, and the AEPEI Study Group. Clin Infect Dis 2012;54: 1230-39.
Clinical features
Patients with moderate-to-severe aortic regurgitation from AVE are often symptomatic and at imminent risk of clinical deterioration. The increasing severity of aortic regurgitation subjects an increased volume load on the left ventricle, which when continuously sustained over time, results in a cascade of ventricular dilatation, hypertrophy, neurohumoral activation, and finally, heart failure. In addition, the coupled mitral regurgitation exacerbating heart failure increases the mean left atrial pressure that consequently causes left atrial enlargement, atrial fibrillation, pulmonary congestion, and pulmonary hypertension.
The purpose of surgical correction for AVE is to restore the integrity of a competent aortic valve. There are 2 options for surgical correction of severe aortic regurgitation due to infectious disease of AV: in most cases, the surgical default is valve replacement but rarely, valve repair.
Clinical Evidence
Patients characteristics
During the 20th century, we noted a shift in the risk profile and demographic characteristics of the patients alongside the microbiology of infectious endocarditis. All these determinants relate to the development of antibiotic treatment, the decline of rheumatic heart disease, and medical advances. 50 Therefore, the category of patients undergoing surgical treatment of aortic endocarditis underwent a paradigm shift.51,52 Aortic valve endocarditis occurred mainly in young or middle-aged adults with underlying rheumatic heart disease or congenital heart disease, thus comprising a substantial proportion of patients affected in the pre-antibiotic era. The shift revealed other causes: prosthetic valve replacement, hemodialysis, indwelling venous catheters, immunosuppression and intravenous drug use (IV) have become the main risk factors. 52 In high-income countries, AVE occurs in older patients who are frailer with multiple comorbidities. From an epidemiological perspective, staphylococci recently became the most frequent causative pathogen, overtaking oral streptococci (Figures 2 and 3).53,54

Clinical evaluation and diagnosis flowchart of aortic valve endocarditis.
In the 21st century, epidemiological studies demonstrated an IE incidence increment of >25% and a further change in demographics. Advances in cardiology such as the emergence of cardiac implantable electronic devices (CIED) and transcatheter valve replacements are radically changing the management of patients. Transcatheter valve replacements, however, may result in higher rates of IE compared to surgically implanted prosthetic valves. 8
Management
Early suspicion is essential during the preoperative phase of aortic endocarditis as some concerning indications for surgery are missed by attending physicians in 1 out of 6 patients as outlined in a recent study. 55 Early recognition and diagnosis help the decision-making process for the multidisciplinary team to focus solely on the emergency surgical criteria and on the clinical guidelines to be tailored to the patients’ presenting complications (Figure 3).
Recent microbiological progress has helped facilitate this process through the association between infective endocarditis and the death of patients in the presence of Staphylococcus aureus bacteremia. Positive blood cultures with early time to positivity (TTP), which is a parameter normally available in automated blood culture systems, maybe an early indicator of the infectious load in patients with systemic infections. 56 Thus, discussions and decision-making within the heart team can help disseminate the best current knowledge to address the surgical treatment of aortic valve endocarditis before the patient’s condition worsens.
However, surgery is only part of the treatment as the heart team is also involved in the choices regarding anticoagulant therapy, optimal antibiotic treatment, and postoperative follow-up.57-63 Internal medicine and emergency physicians should use Duke’s Criteria 64 to initiate the referral to minimize delays the surgical intervention. Patients with heart failure symptoms can easily be managed with appropriate medical treatment. Some patients may present with evidence of severe acute regurgitation or obstruction, resistant pulmonary edema and/or cardiogenic shock which usually indicate a more aggressive and wide infective colonization of the heart structure (Figure 3).13,65,66
Sometimes, the time to reach a diagnosis is prolonged due to the difficulty in identifying a causative pathogen. Evidence for this clinical scenario is represented when the IE sustained by predominantly intracellular microorganisms, such as C. burnetii, Bartonella species, or T. whipplei, whereby exposure and the status of the immune response of the host become key determinants. 67 The difficulty of identifying the pathogen can result in a delay in surgical correction which increases the intraoperative risk in these severely compromised group.13,65,68,69 The TTP test provides reliable information in patients with S. aureus bacteremia, on the risk of IE and prognosis. For example, a short TTP is an independent predictor of death and is a great tool for the recognition of patients who require specific attention. 56
Patients with AVE should have a careful assessment of symptoms and undergo electrocardiography (primarily to evaluate cardiac rhythm) and transthoracic echocardiography to assess the morphology and severity of AV regurgitation, as well as left ventricular size and function. Patients should be offered transesophageal echocardiography if the diagnosis remains doubtful (Figure 4). 70

Shows an algorithm for the use of echocardiography in patients with suspected aortic valve endocarditis. To note that transthoracic echocardiography (TTE) is indicated as the initial investigation of choice for suspected AVE because it is accessible, quick, and safe. Patients who have a prosthetic valve or who previously received a cardiac device will usually require additional imaging with the use of transesophageal echocardiography (TOE). TOE must always be done even if TTE is diagnostic because TOE is an examination by image better for the detection of complications. In patients who have a negative TTE but a highly clinically suspected for aortic valve endocarditis, TOE is suggested and might need to be repeated at 7 to 10 days to confidently exclude the diagnosis. From Habib et al. Eur J Echocardiogr 2010; 11: 202-219.
There is a wide spectrum of neurological complications during infective endocarditis. Several studies recommend rapid and effective diagnostic and therapeutic interventions. Sixty percent of patients have symptoms identified as ischemic and hemorrhagic strokes, which often precede the diagnosis of infective endocarditis, thereby raising the dilemma of the risk of neurological injuries versus the timing of intervention.71-74 Possible events associated with the presence of infectious foci include silent cerebral embolism which is recurrent in 50% of patients, transient ischemic attack, mycotic aneurysm, and cerebral abscess; all of which deserve prompt investigation. 74 Another criterion for early intervention is the presence of vegetations due to S. aureus infection, which may be large, prominently mobile, and often involve patients with complex valve endocarditis and infected loci of pathogen located within the mitral valve. The localization of abscess is crucial to guide the surgery. In the experienced hands of diagnostic imaging experts, it helps provide a clear picture of the valve status (vegetations, valve function) and the risk of embolism (ie, mobile vegetation, evidence of previous septic embolism).65,71-74 Above all, the presence of vegetations from Staphylococcus aureus colonization > 10 mm is indicative of a progressive risk of embolic events requiring emergency surgery (Figure 3). Instead, in cases of established cerebral localization of septic emboli with hemorrhagic evolution, surgery should be postponed and CT scan or 18F-FDG PET/CT or SPECT/CT, as well as MR perfusion scans, should be performed to evaluate the progression of the lesion as per guidelines (Figures 3 and 4).65,74,75 Once the indication for surgery is established, the anesthetist should perform a thorough assessment to provide the best possible outcome with a degree of hemodynamic stability of the patient. 9 The final aim of this coordinated multidisciplinary approach should be to guarantee an early referral to specialized centers and to avoid temporizing surgical intervention, especially in complex and extensive endocarditis.2,9,65,76
Patients who have symptomatic aortic regurgitation and left ventricular dysfunction (ejection fraction, <60%), dilatation (left ventricular end-systolic dimension, >40 mm), or at risk for septic embolization and uncontrolled infection should be offered emergency or urgent surgery. 9 Likewise, asymptomatic patients without left ventricular dysfunction or dilatation but with large vegetation (>20 mm) especially in those located on the mitral valve should be considered for emergency surgery due to the higher risk of neurological complications. Asymptomatic patients with small lesions with no or mild aortic regurgitation should be observed until the development of symptoms or aortomitral regurgitation and considered for elective surgical correction of AVE. 9 Most studies, however, show a sizable proportion (25%-60%) of IE patients presenting with complex lesions and periannular abscess formation.2-4,9,20,21,65
The goal of the multidisciplinary team is to provide the best possible treatment for patients requiring difficult medical and surgical management. The involvement of the perfusionist may be essential especially in cases of extracorporeal circulation prior to surgery. In our experience, no didactic leadership is necessary, much less the one that identifies the principal actor in the cardiac surgeon. It is the patient who takes center stage and can be treated according to his/her status in medical or cardiology wards, however, in case of deterioration intensive care environments are recommended.
Evidence from trial and observational studies
At the time of writing, there were no randomized trials that compared the different substitutes in surgery for aortic valve due to infective endocarditis. Evidence from observational studies, however, strongly suggest that surgical intervention is valuable.3,4,9,10 One such study evaluated the impact of early surgery on long-term outcomes in 304 consecutive adult patients who active IE involving the aortic valve, Aortic Homografts (Ao-H) [n = 86 (28.3%)], conventional stented xenograft (XP) [n = 139 (45.7%)] and mechanical prostheses (MP) [n = 29 (26.0)]. 20 The patients who received an Ao-H had a higher incidence of prosthetic valve endocarditis (58.1% vs 28.8%, P = .002) and methicillin-resistant Staphylococcus infection (25.6% vs 12.1%, P = .002), compared to those who surgical correction was performed using conventional prostheses. After propensity-score analyses to adjust baseline characteristics, the choice of a homograft did not significantly affect early death (odds ratio 1.61; 95% confidence interval [CI], 0.73-3.40, P = .23), overall death (hazard ratio 1.10; 95% CI, 0.62-1.94, P = .75), or reinfection (hazard ratio 1.04; 95% CI, 0.49-2.18, P = .93).
In another report, 22 87 patients with surgical correction for prosthetic valve endocarditis (PVE) were studied. The choice of substitute was aortic homograft in 56 (64%) patients, mechanical prosthesis (MPs) in 20 (23%), and a bioprosthesis in 11 (13%), respectively. During a median follow-up period of 5.5 years, overall cumulative survival was 65% at 10 years without any statistically significant differences at 10 years survival between patients with homografts or conventional prosthesis (58% and 75%, respectively; P = .17). Surgical correction using Ao-H was independently associated with a reduced risk of infection relapse (P = .006) compared to conventional valves.
In a study from France, 39 aortic valve replacement for AVE was performed using xenograft prosthesis, mechanical prosthesis, and homograft in 167 consecutive patients who were followed-up for 5 years. A significant survival benefit was noted for patients who underwent AVR using MP as compared with those who received XP (5-year survival, HR; 2.39, 95% confidence interval (95% CI), 1.09-5.21; P = .029), which persisted after adjustment for baseline in patients <65 years old (HR 4.14 (1.27-13.45), P = .018) but not in patients >65 years old (HR: 1.45 (0.35-5.97), P = .60). When evaluating patients who received homografts and those who underwent surgical correction of AVE with mechanical prostheses, no differences were noted for 5-year mortality (HR 0.46, 95% CI (0.15-1.42), P = .18).
To the best of our knowledge, there are also currently no randomized trials comparing the use of Ao-H and MPs as a substitute in the setting of AV infection. However, data from observational studies including 138 patients (106 Ao-H; 32 MPs) suggest that the use of mechanical prostheses had comparable rates of midterm survival (66% vs 59.6%; P = .68) and freedom from recurrent infection with the use of homografts (P = .02). 40 Conversely, in a report from the Deutsches Herzzentrum Berlin, 1163 patients who underwent a primary or secondary operation for AVE between 1986 and 2007 were studied (follow-up mean 5.2 ± 0.4 years, maximum 18.4 years). 37 Of these, 221 patients received a homograft aortic root replacement for native valve endocarditis (NVE) (45%) in 99 cases and prosthetic valve endocarditis (PVE) (55%) in 122. The severity of lesions was noted by periannular abscess development in 189 patients (86%), and by aortoventricular dehiscence in 120 (63.5%) of recipients of Ao-H.
Among patients who underwent surgical treatment of NVE with homograft, the survival at 10 years was 47.3 ± 5.6% which was higher compared to those who had PVE because the latter developed a greater tendency toward abscess formation (P = .29). SVD was a complication that required reoperation in 8.6% of patients, more for those aged <40 years whereas reoperation for recurrent endocarditis was noted in 5.4% of homograft recipients. 37 The mortality rate due to reintervention at 1 year was not negligible at 16.1%.
The Ross operation may still be preferred in special circumstances, such as in young patients, women with childbearing potential, and other contraindications to lifelong anticoagulation therapy.8,77,78 The use of autograft for surgical correction of AVE is a complex surgical procedure that is indicated for extensive destruction of the leaflet and annulus. In such cases, the Ross operation may be a suitable alternative to the use of homograft due to the increased risk of prosthetic-valve deterioration also for its biomechanical behavior made favorable by the fact of being in the presence of living tissue.79,19,38,80,81-86 One randomized trial comparing autologous versus allogenic tissue in aortic valve surgery included 216 young adult patients (mean age 39 years), with follow-up duration exceeding a mean of 11 years, and reported a significantly better survival rate for patients undergoing Ross procedure than those whose AV replacement was managed with the use of a homograft (95% vs 78%; hazard ratio, 0.22; P = .006). 38 It highlighted the beneficial effect on long-term outcomes after the use of pulmonary artery (PA) in 43% of patients who had previous cardiac surgery. The survival rates at 13 years in patients who underwent the Ross procedure were equal to that of the general British population adjusted for age, sex, and failure with the use of bioprosthetic valves.
We reported an overall survival of 91.0 ± 4.0% at 16 years for the whole cohort of reinforced and non-reinforced Ross procedures, with a mean survival of 18.4 years (95% CI 18.0-18.81). 80 Freedom from Ross-related reintervention rate was 92.5 ± 4.3% at 15 years for the whole cohort (88.3 ± 5.4% (non-reinforced Ross) vs 96.7 ± 3.3% (reinforced Ross)). Mean freedom from reoperation was 18.2 years (95% CI 17.7-18.7) in the nonreinforced group and 15.6 years (95% CI 15.1-16.2) in the reinforced group (P = .233).
Complication
Relapse of infection
Relapse of infection is the primary concern in patients who have previously undergone a surgical operation for complex aortic valve infective endocarditis, which may be associated with extension into the mitro-aortic curtain and/or evidence of fistula formation into a cardiac chamber or pericardium.3,4,9,10,65,20,21,37 Surgeons at Harvard have pointed out its severity, reporting a high incidence among intravenous drug users and non-users.20,21 Many studies highlight the role of structural valve deterioration as a reason for aortic homograft and conventional stented xenograft versus mechanical prostheses36,33; however, the evidence has proven that concerns relating to SVD are inconsistent in the first decade after post-implantation of Ao-H compared to conventional valves.4,23,87,29,88,89 Furthermore, the extension to a single valve leaflet does not exclude the annular involvement which often requires radical debridement with complete clearance of necrotic tissue, vegetation, and foreign material.4,65,66,20,21,89,90 Unfortunately, the de facto “simplest solution” may not always lead to the best long-term results. The reoperation for a relapsing infection carries a higher mortality than the reoperation for structural valve deterioration or dysfunction of an aortic homograft inserted in aortic root position. Active endocarditis, often the cause of recurrence4,66,20,21,89 is a statistically significant univariable risk factor for increased early and late mortality as shown by studies with short20,21 and long-term follow-up (over 20 years).4,23,29,87-89 As far as PVE is concerned, the use of Ao-H appears indisputable, unlike NVE whereby the preference for conventional prosthesis and synthetic material is still predominant (Figure 5). 46
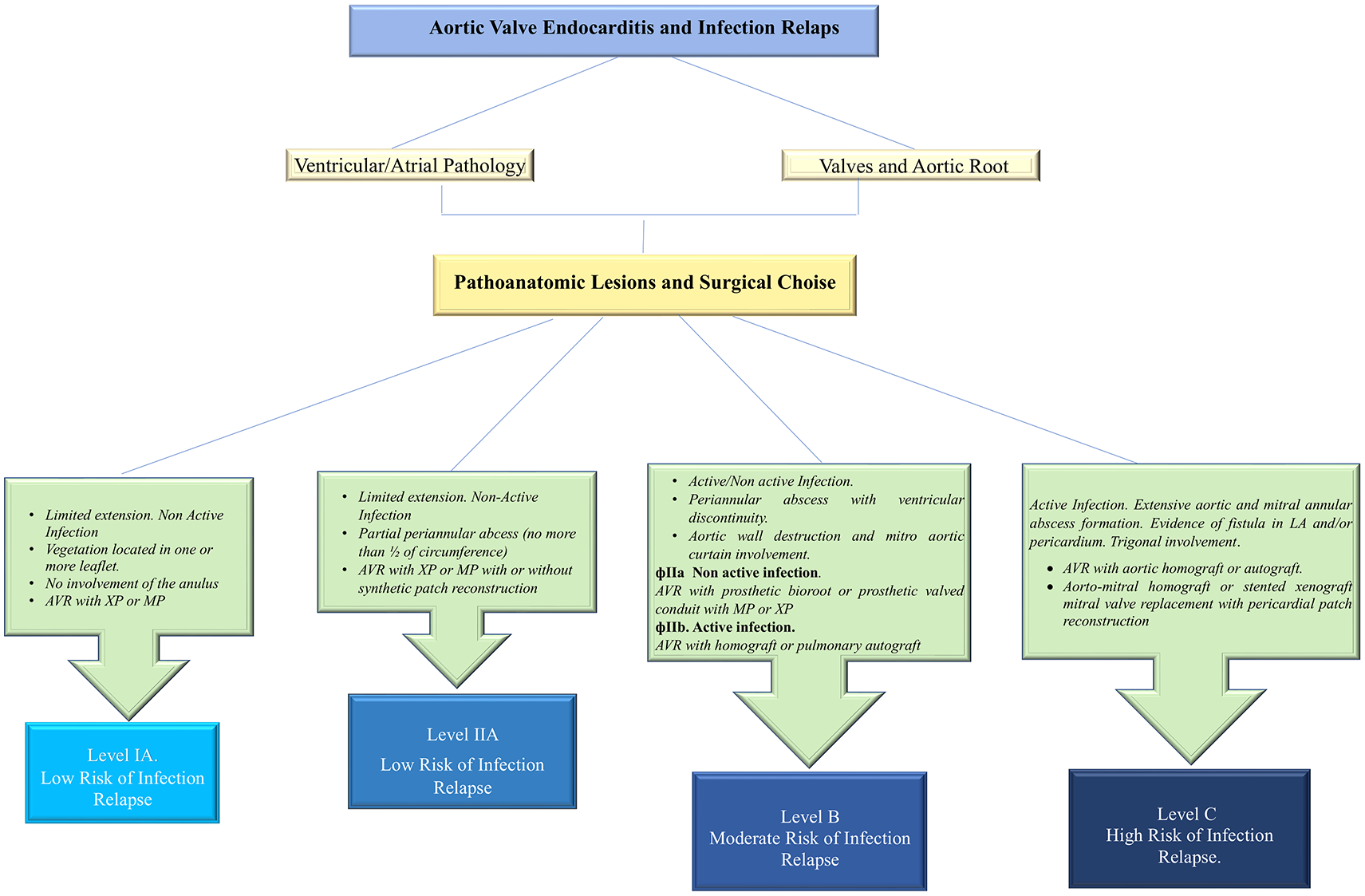
Algorithm to assess risk of infection relapse. Risk categories are identified on the basis of the anatomopathological characteristics of the infection, the magnitude of surgical demolition and reconstruction and the materials used.
Structural valve deterioration
The second surgical consideration when choosing the valve substitute in AVE is durability over time and the risk of a redo operation. This remains the watershed area for decision making with regards to the choice of a homograft compared to conventional stented xenograft or mechanical prosthesis. The homograft surgery itself is technically demanding with an intrahospital mortality of between 2% and 5.5% in elective surgery4,23,29,91 that is acceptable when compared with other prostheses 33 as reported in the literature. There is increased mortality in emergency surgery either for SVD or relapse of infection.4,33,91
The risk of reoperation for SVD of aortic homograft must be compared to the durability of a bioprosthetic valve as an alternative to allogenic tissue. Very recent meta-analyses including all types of available aortic stented/non-stented xenografts (porcine and pericardial) revealed that SVD commonly starts 8 years after surgery, with a greatly increased rate of SVD after 10 years which is comparable with the duration of the allogenic tissue.44,45 Likewise, the St Jude Toronto SPV stentless aortic bioprosthesis (St Jude Medical), although promising excellent results for hemodynamics and durability up to 5 years of implantation, demonstrated a high rate of SVD within 8 years due to the increased mechanical stress on the cusps and late dilatation of the sinotubular junction. 41 Second-generation porcine Hancock II valves (Medtronic) have long-term outcomes including actuarial survival rates without SVD at 10 years (95%), 15 years (75%), and 20 years (49%). 92 The Carpentier-Edwards Perimount (Edwards Lifesciences) pericardial valve in the aortic position showed an actuarial freedom from SVD at 15 and 20 years of 79% and 54%, respectively, with an expected valve durability (median survival time without SVD) of 19 years.25,93
Concerns arise from the use of new biological prostheses in the setting of aortic infective endocarditis due to the limited data available for long-term follow-up reported in the literature. Clinical and echocardiographic evidence have shown only medium-term results which therefore do not confer complete reliability for newer generation pericardial valves. Mitroflow bioprosthesis (models 12A/LX; LivaNova), have a mean time to SVD only of 3.8 ± 1.4 years. 30 St Jude Trifecta aortic bioprosthesis, showed 6-year actuarial freedom from SVD and freedom from reoperation of 95% and 96%, respectively, 94 although some reports of early Trifecta failure were described. 95 Only short-term effectiveness in durability for the surgical sutureless bioprosthetic LivaNova Perceval and Edwards Intuity valves are available.96,97 However, occasional reports of Perceval leaflet fluttering and early failure have also been described. 98
Discussion
Aortic-valve replacement is performed with either isolated mechanical or bioprosthetic or combined with aortic root replacement using a mechanical or biological conduit. It should be noted however, there are several drawbacks to aortic-valve replacement; lifelong anticoagulation treatment and the risk of thromboembolism with conventional mechanical prosthesis or the risk of prosthetic-valve deterioration and failure with the use of bioprosthetic valves; and the risk of relapse of infection with onset of prosthetic-valve endocarditis (PVE) for either. In addition, infection migration to involve the mitral valve through the mitro-aortic continuity may partially or completely affect leaflets with loss of anchoring to the annulus, worsening the hemodynamic compromise in a vicious spiral. As a result, there is compounding damage to the heart structures necessitating extirpative surgery. The objectives of aortic-valve repair are to obtain a proper line of coaptation of leaflets, to preserve the aortic annulus from the development of abscess and to limit the extension of root infection.2,8,9
There is a paucity of data available in the literature to allow a systematic approach to plan timing and choice of valves due to the lack of randomized studies categorized in Class Ia level of evidence (LOE) A or B.3,4,9-13,43,90,99-101 To date, only 1 randomized trial 99 has been published comparing patients who underwent early expedited surgery (within 48 hours) versus those who received medical therapy for severe left-sided IE (ie, large vegetations). The enrolled patients had no indications for emergency surgical correction of endocarditis, thereby resulting in a significantly lower in-hospital mortality or systemic embolization rate in the recipients who underwent surgery versus those who underwent conventional medical treatment (3% vs 23%). The results highlighted that, despite the increased intraoperative risk, early surgery in the case of IE with large vegetations resulted in a reduction of the composite endpoints of death from any cause and embolic events by effectively decreasing the risk of systemic embolism. The patients who underwent surgical correction for IE showed a hospital survival of 90%, and better outcomes within 30 days for NVE than for PVE (5.6% vs 13%) with similar long-term outcomes (35% vs 29%). 102 The infection sustained by Staphylococcus aureus conferred a significantly higher mortality compared with other pathogens. 99
Before the advent of advanced antibiotic therapy, aortic and/or mitral valve surgery was largely adopted for surgical correction of streptococcal infections. Aortic valve replacement with mechanical prosthesis may still be the preferred option even in patients with advancing age, combined or complex surgical procedure, or multiple comorbidities. 9 In such cases, aortic valve repair 35 or reconstruction 103 may be a suitable alternative to replacement. In particular, women of childbearing age who intend to pursue a family or people in general who have contraindications to anticoagulation should be counseled on the benefits aortic valve repair, reconstruction, or even the use of aortic homografts. 104 Pivotal series from centers with proven experience demonstrate good outcomes in terms of mortality (intraoperative from 2.5% to 5.5%) and durability (up to 23 years) when aortic homografts are used as valvular substitutes in endocarditis.23,29,105 More recently the investigators highlighted positive results at 27-year follow-up after surgery using aortic homografts, underlining the importance of allogenic tissue in infection of the heart with low incidence of reoperations for infection relapse (2.2%). 23 Other widely cited historical series favorably express the use of Ao-H in the set of infected fields.37,42 One of these studies reported 13 years’ experience with homografts in endocarditis, showing excellent clinical performance, long-term durability, and a low rate of reinfection with a late mortality rate of 7.9%. Patient survival after post-hospital discharge was 97% at 1 year and 91% at 10 years. 16 Similarly, homograft aortic root replacement in active infective endocarditis with periannular abscess formation showed favorable early and long-term results with significantly better survival in native valve endocarditis than prosthetic valve endocarditis. 37 One study showed similar risk during reoperation itself for mechanical valves, bioprosthetic, and homografts 105 unlike the findings of other studies.3,4,65,20,21
The use of aortic valve repair is limited and is preferable in native endocarditis caused by highly sensitive streptococci in which a small vegetation (<10 mm) is present on 1 leaflet of the aortic valve without the involvement of the annulus. 19 The goal of repairing the aortic valve is aimed at restoring an adequate area of coaptation of the leaflets in diastole with complete movement of the leaflets. The surgeon removes the vegetation (vegectomy) respecting the neckline on the leaflet and generally associating the use of a pericardial patch to reinforce the leaflet subjected to strong stress. This procedure can also be used in the simple perforation of the leaflets. However, the use of repair is not recommended in the presence of vegetation located near the commissures especially when fenestrations exist. Instead, the small vegetation located on the free edge of the leaflet can be removed by reinforcing it with the use of a Goretex CV5 suture. Referring to the Acar technique of replacing the anterior mitral valve leaflet using the autologous pericardium treated with glutaraldehyde, the Ozaki procedure 80 takes advantage of the same principle of using the autologous pericardial patch to replace the aortic valve leaflets. This technique is limited to the localization of infection on the aortic valve only without involvement of the ring. Aortic valve repair has a high rate of reoperation despite being limited to experienced surgeons. The heart team plays an important role here, to help counsel patients about the decision-making process. Specifically, the rate of re-intervention, be it transcatheter valve therapy (TVT) or reoperation should be highlighted.
Several observational studies have shown that extensive and radical surgery is necessary in a large number of patients with IE and with homografts or mechanical valves and xenografts were used in similar complex endocarditis5,16,20,21,65 (Figure 6). One study reported a rate of abscess formation between 9% and 60%, 89 which is higher than the mean frequency (25%-30%) reported by other international studies3,10,23,29,43,106 indicating the severity of the disease treated in this cohort. Surgeons at Harvard reported, in a large number of patients with complex valve endocarditis, the preferential use of mechanical valve prosthesis as a substitute for the infected aortic valve compared to the stented xenograft (40.5% vs 29.5%).20,21 This trend was also confirmed with the simultaneous involvement of the mitral valve using mechanical valves for surgical correction (38% vs 18.7%).20,21 These data seem to reinforce the tendency of some centers, which have long noted an association between mechanical valves and improved long-term survival.3,10

Aortic root abscess. Left: axial computed tomographic image showing the aortic root abscess. Right: a 3D volume rendered image of prosthetic valve endocarditis showing extensive root abscess.
Bucking this trend, we reported the use of homografts as a replacement for aortic and mitral valve diseased in 56.2% and 21% of patients who developed abscess formation.4,65,66,87,89,90 Sometimes in the presence of aggressive IE with extension to the aorto-mitral junction and mitral valve, we opted for a double homograft.4,89,107 In two-thirds of recipients, we performed a monobloc implant while one third received a separate bloc with partial mitral homograft insertion. 107 The technique of implantation has provided good results even in the presence of fragile tissue due to the presence of infection.4,89,107 We believe that endocarditis treatment should be guided by principles of avoidance of infection recurrence and functional valve outcomes. Although some reports3,20,21 praised the long-term outcomes of mechanical valves, subjecting patients to life-long anticoagulation which carries significant risks cannot be neglected. Additionally, the population normally afflicted by endocarditis is relatively young and often keen to return to an active lifestyle, making oral anticoagulation a potentially significant impairment to their quality of life. In female patients, anticoagulation effectively excludes their childbearing potential altogether.
Our propensity to utilize allogeneic tissues for extensive infections involving the heart structure, either in native or prosthetic valves, is supported by an innovative German study. 108 The authors have shown that Ao-H has antibacterial activity despite long-term conservation (5 years). Antibiotic combinations (gentamicin, vancomycin, metronidazole, piperacillin, flucloxacillin, tobramycin, meropenem, colistin, and the anti-fungal amphotericin-B) applied during cryopreserved aortic homograft (CAH) processing have a significant influence on their infection resistance. Homograft tissue of the ascending aorta revealed a significantly enhanced resistance against staphylococcal bacteria (S. epidermidis and S. aureus) with less bacterial contamination compared with homograft aortic valves. More effective resistance was noted against P. aeruginosa using flucloxacillin and E. coli using meropenem and colistin. 108 Application of antibiotics after thawing CAH led to a significant decrease in the recurrence of infections 109 that conventional prostheses or Dacron grafts have not yet clearly demonstrated, although the risk of vascular graft infection is reduced by pretreating the prostheses with antibiotics. 110 The antibiotic/fibrin combined compound had a net effect of the delayed release of antibiotics to aid early prevention of infection relapse. 110 Furthermore, new suggestions on effective concentrations of β-lactam antibiotics may enhance this action thus providing additional immunity to recurrence. 111 The favorable response of allogeneic tissue to antibiotics has been documented23,29 where 21% and 25% of recurrent endocarditis in Ao-H were successfully treated medically without surgical re-intervention.
Selection of the type of graft to use for active endocarditis should be driven by the resistance to infection, as re-do surgery in cases of re-infection is particularly challenging and carries significant risks. Particular attention to technical details is required when using Ao-H such as allograft friability and anastomotic failure caused by inappropriate mechanical stress. 112 Reinfection of synthetic prostheses or prosthetic materials, normally employed in cases of complex endocarditis when a homograft is not used, is even more daunting and technically demanding than in reinfection of an implanted homograft.4,23,29,66,88,89 In this context, the safety and effectiveness of Ao-H over conventional prosthesis on the recurrence of infection has been widely reported in several observational studies,4,23,29,43,101,113,114 albeit with a difference in resistance to infection found between the valve and aortic wall of Ao-H. 108 Between 2% and 5.3% of patients with relapse or recurrence of infection following aortic valve, endocarditis surgery occur within the first year.16,29 Recent reports showed a low recurrence of endocarditis in homograft even in complex cases with extensive injury of heart structure.24,29 The largest controlled series showed a rate of freedom from allograft infection at 10 years post-implantation of 88% in active endocarditis during implantation versus 95% in patients without a history of endocarditis.29,88
As a rule of thumb, endocarditis surgery should be dictated by 3 factors, the patient, the surgeons’ experience/center experience, and the extent of the infection. A highly experienced surgeon/center well versed in aortic valve repair techniques may offer a young patient with aortic valve endocarditis limited to a single leaflet and no annular involvement would be an ideal candidate for a repair procedure, however, an older patient on anti-epileptics with extensive annular involvement may be best treated with a homograft/bioprosthesis after debridement. The role of the heart team has to be emphasized with the 3 factors balanced out to specify the best possible outcome for each individual patient.
Conclusion
The major findings of this review noted that surgical correction of aortic valve endocarditis ranged around 55% per year and in high-income nations, most of the patients involved were >60 years. There is a general preference for biological prostheses18,26,31 as the primary intervention over mechanical prostheses27,115 and homografts or autograft.28,32,34,47 Aortic valve repair is indicated in selected cases and the use of the TAVR is not recommended in current guidelines.17,116-118 Homografts were more commonly used in NVE with extensive annular destruction or abscess formation, in extirpative heart surgery and prosthetic valve endocarditis. In the previous decade, allogenic tissue was used in 7% of primary interventions and up to 32% for secondary intervention. Historical series of patients receiving allogenic tissue for AVR showed a lower incidence of infection relapse at up to 25 years follow-up. The role of shared decision making amongst the heart team is crucial to establish the timing of surgery. It may play an even more decisive role in the coming years with an increased number of TVT procedures and implantable cardiac devices. Endocarditis has over the years changed its spots; perhaps it is time we change the tools at our disposal.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
All authors contributed equally to this article.