
Abstract
Left main coronary artery thrombus (LMCA-T) is a rare disease state and diagnosed with invasive coronary angiography (ICA). We present a case of LMCA-T diagnosed with coronary computed tomography angiography (CTA) and treated without ICA in a patient who presented to a hospital in the middle of war zone in Erbil, Iraqi Kurdistan. Coronary CTA performed 1 month later demonstrated resolution of the thrombus. Fractional flow reserve computed from computed tomography (FFR-CT; HeartFlow, Redwood City, CA) performed retrospectively confirmed that the clot was not hemodynamically significant at the time of diagnosis. This case demonstrates the diagnostic capabilities of coronary CTA and FFR-CT when ICA is not readily available.
Keywords
Case
A 40-year-old man with history of hyperlipidemia and cigarette consumption presented with shortness of breath and chest tightness. Physical examination was unremarkable. The patient refused invasive coronary angiography (ICA) but agreed to coronary computed tomography angiography (CTA). The coronary CTA demonstrated a hypodense (40 Hounsfield units [HU]) thrombus in the ostium of the left main coronary artery (LMCA) with less than 50% narrowing (Figures 1-4). The rest of the coronary arteries were without disease. He was treated as an outpatient with enoxaparin, aspirin, and statin medication. The patient was seen in the follow-up 1 month later and a repeat coronary CTA demonstrated resolution of the left main coronary artery thrombus (LMCA-T). Fractional flow reserve computed from computed tomography (FFR-CT) was performed on both studies retrospectively (Figure 5).

Oblique view of the left main coronary artery with hypodense thrombus in the ostium.
Oblique view of the left main coronary artery with resolution of the thrombus 1 month later.

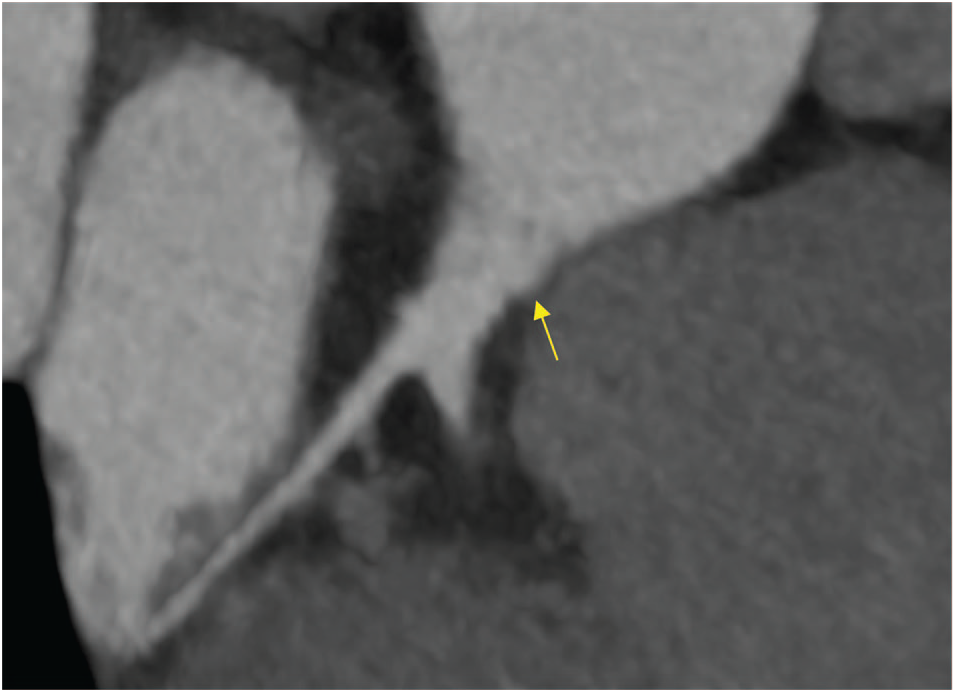
Cross sections of the left main coronary artery demonstrating a thrombus in the ostium. The image was obtained using curved multiplanar reformation. The blue dots represent the center line. Arrows point to the thrombus.

Cross sections of the left main coronary artery demonstrating resolution of the thrombus present 1 month previously. Arrows point to the location of the previous thrombus.

FFR-CT on presentation is shown on the left and that after treatment on the right. There was no change in vessel hemodynamics. FFR-CT indicates fractional flow reserve computed from computed tomography.
The CTA examination was performed using a Brilliance iCT 256-slice scanner (Philips Medical Systems, Eindhoven, The Netherlands). Images were acquired with retrospective electrocardiogram (ECG) gating during sinus rhythm at a rate of 72 beats per minute. Additional parameters include 128 × 0.625 mm2 detector collimation, 256 × 0.625 mm2 slice collimation, and 270 ms gantry rotation time. The tube voltage was 120 kV. Images were reconstructed in 5% increments from 0% to 95% of the R-R interval using a 512 × 512 matrix with a slice thickness of 0.6 mm. A medium soft-tissue convolution kernel was used.
Left main coronary artery thrombus is a high-risk condition that often presents with cardiogenic shock.1-3 Underlining risk factors for coronary artery disease prevail; however, an assortment of rarer conditions such as hypercoagulable state, embolization, autoimmune conditions, coronary aneurysm, spontaneous rupture in the young or athletic, thrombophilia, and cocaine have been reported. 2 Thrombi on coronary CTA should be considered in the appropriate clinical presentation, such as acute coronary syndromes. Intracoronary thrombus has a classically low attenuation (25-80 HU), 4 which overlaps to some degree with the attenuation range that defines low attenuating plaque (−30 to 30 HU). Thrombi, however, typically appear as a filling defect within the coronary lumen with contrast surrounding the defect.
Treatment has evolved from anticoagulation alone to thrombolytic therapy, antiplatelet therapy, percutaneous coronary intervention, bypass, thrombectomy, and left main stenting. Only very rare cases of LMCA-T have been reported by coronary CTA and no cases where invasive angiography was not performed and where treatment was initiated based solely on CTA findings were reported. Subsequent imaging documented resolution of thrombus and with nonobstructive findings confirmed with FFR-CT. 3
Coronary CTA is now available worldwide, even in remote locations such as Erbil, Iraqi Kurdistan. Advancements in CTA imaging offer excellent anatomical characterization and high spatial resolution with the ability to discern intracoronary thrombus as well as vulnerable plaque. The addition of FFR-CT provides unparalleled, noninvasive hemodynamic assessment to better aid clinical management in near real time. As illustrated in this case, follow-up imaging not only demonstrated successful dissolution of the left main thrombus but also restoration to normal physiology. Although LMCA-T was diagnosed and treated noninvasively in this case, we are not representing that this approach be applied to other presentations. Instead, this case provides a context in which advanced coronary imaging coupled with computation fluid dynamics–derived physiology can better inform the clinician and guide management decisions. This case additionally highlights the possibilities of physiological measures such as FFR-CT to accurately predict the need for revascularization. 3
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
All authors contributed and reviewed the content of this manuscript.