
Abstract
Background:
Rotational atherectomy (RA) has been used in percutaneous coronary intervention (PCI) for 30 years. With advances in technology, this observational study looks at how rates of RA have changed over the past decade in Australia in relation to PCI and coronary artery bypass graft (CABG) rates.
Methods:
Retrospective analysis of RA, PCI, and CABG rates per Australian state from Australian Government Department of Human Services’ data on Medicare items from 2007 to 2017 was carried out.
Results:
There were 149 RA procedures in 2007, increasing to 452 in 2017. Rotational atherectomy accounted for 0.67% of PCI procedures in 2007, increasing to 1.48% in 2018 (+0.81%, 95% confidence interval [CI] = [0.64%-0.91%]; P < .001). Most of this increase has come from procedures in New South Wales (441% increase). Australian PCI rate increased from 22 301 to 30 480. Rate of CABG decreased from 5418 to 5206.
Conclusions:
From 2007 to 2017, rates of RA trebled in Australia. This is despite stable rates of PCI and a fall in rates of CABG. There are several clinical explanations for this trend.
Keywords
Introduction
Rotational atherectomy (RA) has been practised by cardiologists for over 30 years. 1 The technique involves debulking atherosclerotic plaques in coronary arteries via an abrasive intraluminal burr. In the late 20th century, RA was employed regularly in percutaneous coronary intervention (PCI); 2 however, in the drug-eluting stent era, it fell out of favour. 3 Multiple trials had shown that routine use of RA had no benefit in angiographic outcome during routine PCI.4,5 Furthermore, it risked several complications, including but not limited to severe vessel spasm, coronary artery dissection, perforation, and no-reflow.6–10
Since these early trials, RA’s use has evolved: providing a necessary adjunct to modify both heavily calcified lesions and ostial side branch lesions prior to balloon expansion and stent deployment, 11 as well as offering a feasible alternative to surgery in high-risk patients. 12
Although still not indicated routinely, it is useful in tackling complex lesions when standard balloon dilatation fails, with the Australian Medicare Benefits Schedule (MBS) advising that RA be available for revascularisation of complex and heavily calcified coronary artery stenoses in patients for whom coronary artery bypass graft (CABG) surgery is contraindicated. 13
Rotational atherectomy involves an elliptically shaped burr with a distal tip coated in diamond chips that range in size from 20 to 30 µm diameter. This is rotated via an air motor at 140 000 to 200 000 r/min, resulting in differentially cut inelastic material.
While national registry data have been published in recent years from other parts of the world, including Japan (accounting for 3.2% of PCI procedures) and Europe (ranging from 0.8% to 3.1%), no such study has looked at the Australian cohort.8,14 Our aims were to calculate rates of RA in Australia over the past decade and to compare these with rates of PCI and CABG surgery.
Method
Australia’s MBS lists all outpatient and private hospital coronary catheterisation procedures. Rotational atherectomy has been available on the MBS since 2003. We analysed Australian Government Department of Human Services data on MBS items for coronary artery RA (code numbers 38309, 38312, 38315, 38318), PCI (code numbers 38300, 38303, 38306) and CABG (code numbers 38497, 38498, 38500, 38501, 38503, 38504) from January 2007 to December 2017 (http://medicarestatistics.humanservices.gov.au/statistics/mbs_item.jsp, full description of code numbers is available in Appendix 1). The study protocol was submitted to the following independent Ethics Committee: Central Coast’s Local Health District Research Governance Office. As no individual patient data were collected with the information freely available, the study received exemption from ethics approval.
Statistical analysis
The number of RA, PCI, and CABG procedures were counted for each year from each state in Australia. Microsoft Excel (Microsoft Corp, Redmond, WA, USA) and Stata Version 15 (StataCorp LP, College Station, TX, USA) were used to analyse data. Frequency polygons were used to present and compare graphically RA and PCI rates between 2007 and 2017. The Royston chi-square test for trend was used to test the null hypothesis of change in RA rates over time with 5% level of significance (P < .05). 15
Results
Rates of RA have trebled in Australia over the past 10 years from 149 procedures in 2007 to 452 in 2017 (Table 1). During the same period, PCI rates increased modestly from 22 301 to 30 480 procedures per year, and CABG rates fell during this period from 5418 procedures in 2007 to 5206 procedures in 2017, representing a 5.3% decline (Table 1).
Changes in rates of RA, PCI, and CABG procedures in Australia from 2007 to 2017.

Abbreviations: CABG, coronary artery bypass graft; PCI, percutaneous coronary intervention; RA, rotational atherectomy.
In 2017, RA was used in 1.48% of PCI procedures, significantly up from 0.67% of procedures in 2007 (+0.81%, 95% confidence interval [CI] = [0.64%-0.91%]); P < .001 (Figure 1). There is significant geographic variation between Australian states in RA uptake (Figure 2). Most of this increase has come from procedures in New South Wales (441% increase) and Queensland (219% increase). Despite being the second most populous state (6.3 million) with the fastest rate of population growth, 16 Victoria’s RA rates have plateaued.

RA rates as a proportion of PCI procedures performed from 2007 to 2017. PCI, percutaneous coronary intervention; RA, rotational atherectomy.

RA rates by Australian state from 2007 to 2017.
In relation to PCI procedures, there has been a significant proportional increase in trend of RA procedures seen in New South Wales, Queensland, South Australia, Western Australia, and Tasmania (Table 2, appendix 2).
Proportion of rotational atherectomy cases to percutaneous coronary interventional cases per state.
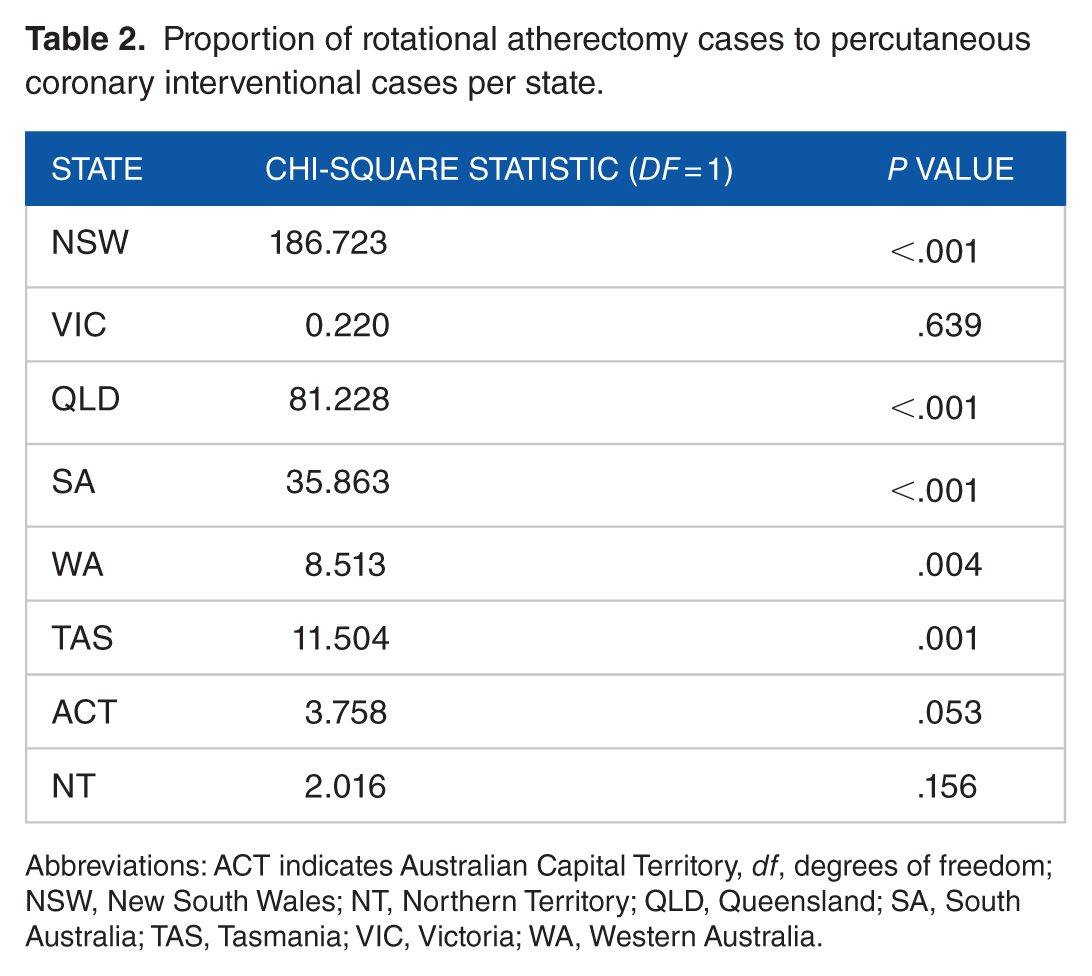
Abbreviations: ACT indicates Australian Capital Territory, df, degrees of freedom; NSW, New South Wales; NT, Northern Territory; QLD, Queensland; SA, South Australia; TAS, Tasmania; VIC, Victoria; WA, Western Australia.
In 2007, of the 149 RA procedures performed, 85% (127 procedures) underwent PCI with RA, with the remaining 15% (22 procedures) solely undergoing RA as stand-alone procedures. By 2017, the proportion undergoing PCI with RA had increased to 95% with the remaining 5% occurring as stand-alone procedures (Figure 3).

RA use as part of PCI versus as a stand-alone procedure in Australia from 2007 to 2017. PCI indicates percutaneous coronary intervention; RA: rotational atherectomy.
Discussion
Rotational atherectomy was commonly used as both a stand-alone procedure and later as a prelude to balloon dilation for modifying coronary artery plaques. 17 Up to 20% of interventional procedures involved the technique 30 years ago, but its use declined to around 1% with the evolution of easy-to-deploy drug-eluting stents, the lack of benefit in preventing re-stenosis, and the risk of serious ischaemic complication such as cardiogenic shock.18–20 Despite this, national registry data had shown that its use remained stable in the early 21st century, 3 as clinicians recognised that RA provided a necessary aide to PCI, with current American Heart Association’s (2011) guidelines stating that ‘rotational atherectomy is reasonable for fibrotic or heavily calcified lesions that might not be crossed by a balloon catheter or adequately dilated before stent implantation’. 21
Our findings show that rates of RA have increased significantly over the past decade in Australia against the trends seen in PCI or CABG rates. These results show that Australia sits in line with European countries such as the United Kingdom, Holland, and Portugal (comprising 1.3%, 1.4%, and 1.5%, respectively) for the rate of atherectomy procedures performed as a proportion of PCI.14,22 While an observational study suggested that rates of RA have increased in the United Kingdom over the past decade, little data are available on worldwide trends. 23 Given the risks of treating elderly cardiovascular patients with surgical intervention, 24 the proportional rise seen in RA might reflect a demographic shift: with an increased willingness to treat elderly, high-risk, patients with complex lesions via angiographic (vs surgical) means. Indeed, in the US cohort, CABG surgery rates had decreased by 5% annually from 2001 to 2009.14,25
It is unclear why such regional trends exist, with Australian demographic statistics showing little change over this time, with the population of New South Wales and Australia increasing from 6.8 and 20.9 million in 2007 to 7.8 and 24.6 million in 2017, respectively. 26
There are several clinical explanations for the upward trend seen in RA. First, with the use of intravascular ultrasound, there has been greater appreciation of heavily calcified plaques that are otherwise unsuitable for PCI. Mintz et al 27 found that coronary calcification was poorly appreciated at angiography, being seen in 38% of lesions, with this figure increasing to 73% if intravascular ultrasound was used. While no study has looked at intravascular ultrasound usage in Australia, as its use has increased, use of RA might also have increased. Second, complication rates have decreased with a Cochrane systematic review (2012) reporting that the incidence of post-procedure major adverse cardiac events as being similar between RA and angioplasty (relative risk (RR) = 1.27; 95% CI = [0.86-1.90]). 28 The reasons behind the improvements seen in complication rates are 3-fold, including (1) smaller catheters, (2) a radial artery approach (with a bleeding complication rate of 0.04% radially vs 1.3% femorally), and (3) modern perfusionists avoiding large burr sizes and excessive deceleration speeds (both of which can lead to increased complication rates).22,29–31 Third, recent studies have shown that RA use prior to drug-eluting stent deployment can reduce the risk of stent deployment failure.32,33 With the advent of new technologies, including orbital atherectomy (which is not currently available in Australia), 19 there is likely to be further interest in tackling complex lesions with atherectomy.
The main limitation of this observational study is that it is reliant on the MBS dataset (as discussed further in Appendix 1). It does not include patients who do not qualify for MBS, and this suggests the presence of selection bias. Furthermore, this dataset does not provide baseline characteristics of the population such as age, gender, or coronary artery calcium score, nor changes in complication rates. It is unclear from this study whether RA results in improved patient outcome.
Conclusions
Rates of RA have increased dramatically over the past decade in Australia and specifically New South Wales during a time when PCI rates have plateaued and CABG rates fallen. With increasing awareness of heavily calcified lesions, an ageing population, and improvements in technology, we predict RA use to increase further in the coming years.
Footnotes
Appendix 1
Australia’s Medicare Programme allows all ‘clinically relevant’ services (defined as being deemed necessary for the appropriate treatment of the patient) to be at least partially claimable as part of the MBS. While there is free treatment for public patients in public hospitals, all other services such as outpatient procedures and inpatient procedures are claimed. The list of the relevant codes for the claims listed in this study is shown below:
Appendix 2
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: BG reports receiving proctorship fees for the WATCHMAN™ device (Boston Scientific Corporation). No other potential conflict of interest relevant to this article was reported.
Author Contributions
PB devised the project and was a major contributor to writing the manuscript. MP was a major contributor to writing the manuscript. BG was a major contributor to writing the manuscript. MP analysed the data and contributed to the statistical analysis and results sections. GL oversaw the project’s development.