
Abstract
Background:
Patients with stable coronary artery disease (CAD) can be evaluated for myocardial viability by examining reverse redistribution of Thallium-201 (201TI) through cardiac scintigraphy. There is limited knowledge about association of a reverse redistribution with favorable cardiac outcomes. In this study, we hypothesized that higher left ventricular ejection fraction (LVEF), lower myocardial necrosis, fewer ischemic events, and less angina will be associated with reverse redistribution of 201TI imaging.
Methods:
Adult patients with stable CAD included in this study underwent exercise-redistribution Thallium single-photon emission computed tomography (SPECT) and were followed for one year. LVEF and regional wall motion abnormalities were evaluated with echocardiography, exercise duration by bicycle testing, and myocardial ischemia and viability by Thallium SPECT.
Results:
We studied 159 patients (87 men, 72 women, median age 60 years, range: 38-84) with well-developed collaterals. Those with reverse redistribution on SPECT (n = 61, 38.3%) had significantly better exercise tolerance (⩾85%; P < .001). Subjects with reverse redistribution had better LVEF (P < .001), wall motion parameters (P < .001), a lower degree of myocardial necrosis (P < .05), less angina during follow-up (P = .02), and fewer ischemic events whether treated with OMT or PCI (P < .001).
Conclusions:
Reverse redistribution of 201Tl on scintigraphic images is a predictor of myocardial viability. Evidence from our study suggests that optimally treated chronic CAD patients with reverse redistribution may have lower likelihood of future adverse cardiovascular events and better prognosis.
Revascularization is the recommended optimal approach for managing coronary artery disease (CAD) presenting with an acute coronary syndrome. 1 Optimal management of patients with stable CAD is, however, still controversial.2,3 Guidelines from the European Society of Cardiology (ESC) recommend a non-invasive assessment of myocardial viability in stable CAD, and decision making by a multi-disciplinary team.1,4 Some studies have suggested that medical therapy may be an optimal approach in management of specific patients with stable CAD who have viable myocardium and a well-developed collateral circulation, a condition that is often associated with a reverse redistribution pattern during Thallium-201 (201TI) myocardial perfusion imaging (MPI).3,5 Findings from functional tests that detect viable myocardium, such as reverse redistribution of 201TI during MPI will be helpful in determining management of coronary stenosis.
Stress-MPI is often employed to assess the functional significance of obstructive CAD. It is very useful in cases with a moderate pre-test probability of CAD and in accurately predicting presence of epicardial CAD. 1 Moreover, the left ventricular function may be preserved despite severe coronary stenosis or occlusions in the presence of an abundant collateral circulation. 6 It is unclear whether optimal medical therapy or coronary revascularization is appropriate in the management of these patients. The aim of our study was to evaluate the outcomes in patients with stable CAD and well-developed collateral circulation at angiography and reverse redistribution of 201TI in the territory of the culprit coronary artery.
Our hypothesis was that there will be greater preservation of left ventricular function, exercise tolerance and symptoms, and better long-term outcomes, regardless of assignment to PCI or OMT in patients with reverse redistribution.
Methods
Patients
Adult patients undergoing coronary angiography between January 2011 and December 2013 in the Department of Cardiology at the University Clinical Hospital in Mostar, Bosnia and Herzegovina were enrolled. A complete physical examination, routine laboratory tests, electrocardiogram (ECG), stress ECG and echocardiography, and 201TI SPECT were performed. Informed consent was explained and obtained from each patient. This study was approved by the University Clinical Hospital Institutional Review Board
Study Protocol
Echocardiography
Two-dimensional echocardiography was performed with a 2.5-MHz transducer (GE, Vivid 4). Four standard views of the left ventricle were obtained for each acquisition: parasternal long axis, short axis at mitral and papillary muscle levels, and apical four- and two-chamber views. Undigitized images were analyzed by two independent operators. Regional wall motion was evaluated at the chordal, papillary muscle, and apical levels. Wall motion and systolic thickening were graded semiquantitatively by use of a scoring system in which 1 = normal, 2 = hypokinesia, 3 = akinesia, and 4 = dyskinesia. Normal left ventricular ejection fraction (EF) was defined as ⩾50% estimated by 2-dimensional (2D) echocardiography. Left ventricular volumes at end diastole and end systole were computed using a standard Simpson’s method from the apical 2- and 4-chamber views to estimate LVEF.
SPECT imaging
All patients had a symptom-limited, multistep, dynamic bicycle stress test (“Ergo-fit300”). The initial workload was set at 25 W, and the exercise intensity was increased by 25W-steps each minute until the onset of symptoms or until 85% of the age-adjusted heart rate target was reached. At peak exercise, 111 MBq (3 mCi) of Tl-201-chloride was injected intravenously and the patient was encouraged to continue exercising for another minute. Within 10 minutes after completion of the exercise test SPECT imaging was performed using a large-field-of-view gamma camera (Anyscan S; Mediso Ltd. Hungary) equipped with a low-energy general purpose collimator centered on the 73- and 164-keV photopeaks each with a 20% window. Single-photon emission computed tomography (SPECT) was performed as a semi-circular 180° orbit starting from 45° right anterior oblique to 45° left posterior oblique at 6° steps (30 seconds duration of each step). Redistribution images were obtained 3 hours later with 40 seconds acquisition time per angle and tomographic images were stored in a 64 x 64 x 16 matrix. From the raw scintigraphic data, tomograms oriented along the three standard orthogonal views (transaxial, sagittal, and short-axis) were reconstructed using identical filtering. 7 Filtered backprojection with a Butterworth filter (order, 5; cutoff, 0.5 cm−1) was used. No attenuation correction was applied. The pattern of redistribution was evaluated by both visual and quantitative analysis comparing the stress and redistribution images. Reverse redistribution was defined as ⩾10% decrease in relative thallium-201 activity between stress and redistribution images and included either the worsening of a perfusion defect apparent on stress images or the appearance of a new defect on the redistribution images, see Figure 1.

SPECT heart with 201Tl/scintigraphic images of reverse redistribution: second, fourth and sixth order (redistribution): visible perfusion defect infero-apical segment 3 hours after the load. The first, third and fifth row (immediately after the load): no perfusion defect.
Quantitative 201Tl Analysis
Three-pixel-thick slices were reconstructed along the short, horizontal, and vertical long axes of the heart. Flood, center of rotation, and decay correction were applied during reconstruction. 201Tl images were visually interpreted (normal, moderate, frank, or complete defect) by an experienced observer, who was unaware of the clinical, echocardiographic, or angiographic characteristics of the patients. Regional 201Tl activity was measured in each myocardial sector, and it was expressed in each patient as a percent of the maximal 201Tl activity for each set of images. A 201Tl defect was defined when 201Tl activity measured <80% of maximal activity. Alignment and analysis of the two studies was visually made by two operators. Redistribution was defined when relative 201Tl activity at 3 hours imaging increased ⩾10% above the initial value. Persistent defects at 3 hours imaging were classified as mild to moderate when 201Tl activity was ⩾50% of maximal activity and severe when 201Tl activity was <50%. Segments with persistent and severe reduction of 201Tl activity were considered nonviable, whereas all other segments were considered viable.
Coronary angiography
Coronary angiography (transfemoral or transradial) was performed by the Judkin’s method (Shimadsu digital flat panel detector). 8 Collateral vessels were graded according to the Rentrop classification: 0, no filling of any collateral vessels; 1, filling of side branches of the artery to be perfused by collateral vessels without visualization of the epicardial segment; 2, partial filling of the epicardial artery by collateral vessels; and 3, complete filling of the epicardial artery by collateral vessels. All angiographies were evaluated by two cardiologists who were unaware of the other results. Patients in Rentrop grades 2 and 3 were classified as well-developed collateral circulation. 9
Patient Follow-Up
Patients were followed up for the occurrence of major adverse cardiac events (MACE): angina, myocardial infarction (MI) or death. MI was defined using American College of Cardiology/ESC criteria and angina was using Canadian Cardiovascular Society Grading System for Stable Angina. Decisions about revascularization were made by the cardiologist based on the results of diagnostic angiography only.
Statistical Analysis
Results were stored in a MS Access database. SAS software version 9.4 was used for statistical analysis. Descriptive analyses included calculation of frequency and percentage for categorical variables, median and interquartile range or means for continuous variables, as appropriate. To test differences between groups, chi-square test, Fisher’s exact test, and the independent t-test were used as appropriate. Multivariate survival analysis was conducted using Cox-Proportional hazards model accounting for demographic variables of age and sex. Adverse disease outcomes of angina, MI, death, and any or mixed adverse events were compared between patients with and without reverse redistribution. A P-value of <.05 was considered statistically significant.
Results
A total of 1722 patients underwent coronary angiography between January 2011 and December 2013. Of these, 1472 patients had significant CAD involving at least one major coronary artery, and 314 patients (21.3%) had well-developed collateral circulation to the culprit artery territory (Figure 2). In 258 of these patients with stable CAD, 201Tl MPI was performed; 221 patients (128 men, median age 62 years) had significant stenosis during angiography and 159 (87 men, median age 60 years) had well-developed collateral circulation in the culprit vessel territory, whereas 62 patients (41 men, median age 58 years) had no angiographically visible collateral circulation. There was insignificant CAD (<50% stenosis) in the remaining 37 patients (16 men, median age 56) (Figure 2).

Flowchart of inclusion and exclusion of patients, and patient characteristics.
Myocardial Scintigraphy
We investigated scintigraphic characteristics of myocardial segments with/without significantly narrowed epicardial arteries associated with/without well-developed collateral circulation in 258 patients. Patients with scintigraphic finding of reverse redistribution, as compared to patients with other positive scintigraphic findings were more likely to (a) have good collateralization (P < .001), (b) have >50% luminal occlusion (P < .001), (c) have EF ⩾50% (P < .001), (d) achieved ⩾85% of age-predicted heart rate during stress-testing (P < .001), and (e) had normal wall motion measured with echocardiography (Table 1).
Functionality of myocardial segments with reverse redistribution.

EF: ejection fraction.
Incident cardiovascular events—subgroup of 155 patients with significant stenosis, well-developed collateral circulation and positive scintigraphic findings (Table 2):
Cardiovascular events after 1 year follow-up according to scintigraphic findings.
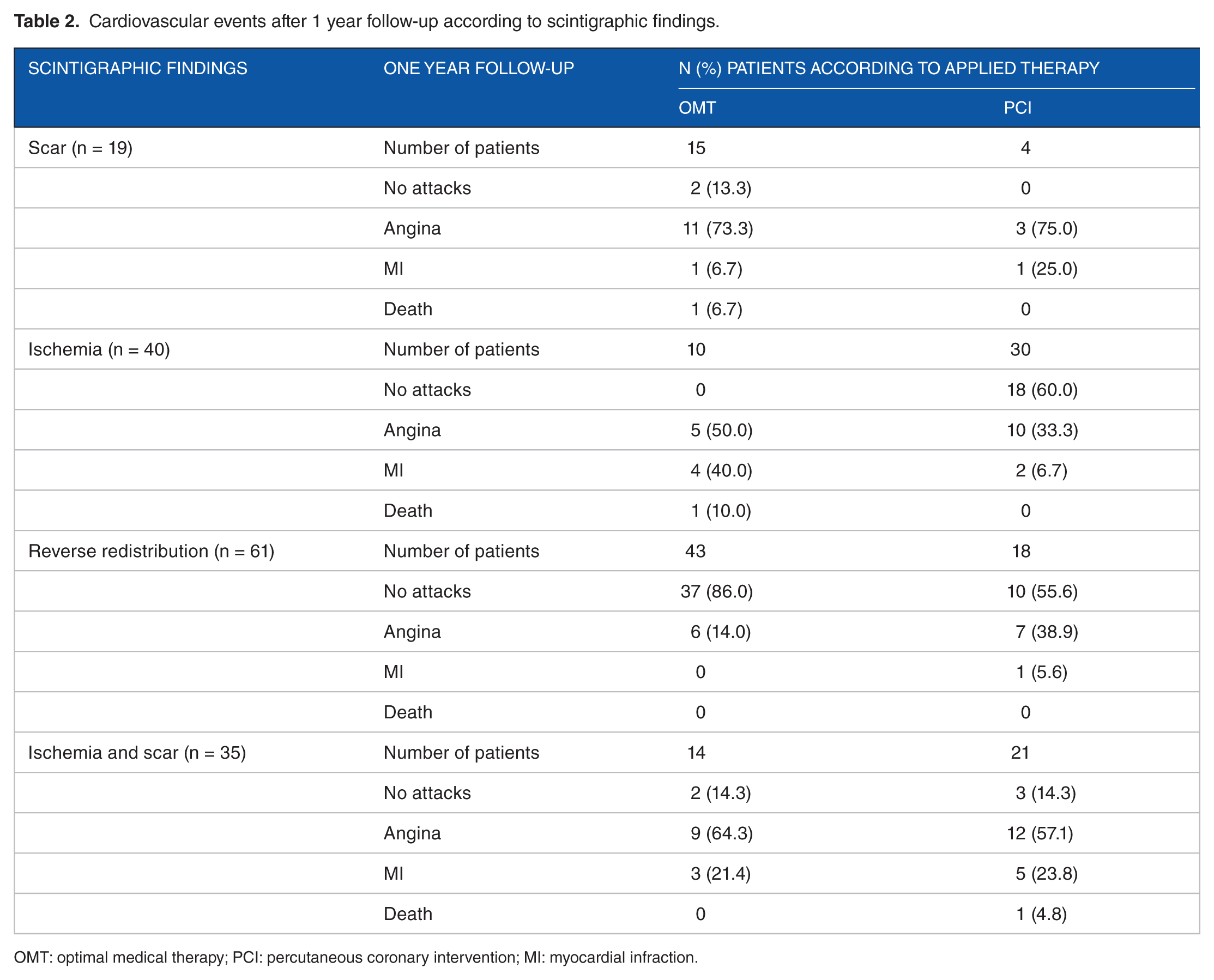
OMT: optimal medical therapy; PCI: percutaneous coronary intervention; MI: myocardial infraction.
In the subgroup of patients who were event-free at 1-year follow-up and had scintigraphic finding of a reversible defects (ischemia) PCI was the most commonly employed treatment modality (P < .001). On the other hand, in the subgroup of event-free patients who had reverse redistribution pattern during 201Tl MPI, OMT was the most common treatment (P = .02).
A subset of 159 patients with good collaterals was found by invasive cardiologists in this study. The functional collaterals (collaterals able to nourish the corresponding myocardial segment) defined by pattern of reverse redistribution of 201Tl in the corresponding myocardial segment were found on scintigraphy in 61 subjects (38.3%). The remaining myocardial segments in this category were scintigraphically presented as either ischemia or scarring indicating insufficient collaterals of the respective segments. Reverse redistribution pattern was associated with well-developed collateral circulation in all published papers.10–14 Of these 159 patients with significant narrowing of the coronary arteries and well-developed collaterals, 140 patients had viable myocardial segments (40 pts had scintigraphic ischemia, 61 reverse redistribution, 35 patients had mixed perfusion defects indicating ischemia with scarring and 4 patients had no scintigraphic visible perfusion defects). Twenty three out of 40 (46%) patients with angiographically proven significant stenosis and well-developed collateral vessels had EF over 50%, 17/40 (42%) patients had normal wall motion and 15/40 (37.5%) patients achieved more than 85% of age-adjusted ergometric load. PCI was performed in 30 patients and of those 18 were event free during 1-year of follow-up, 10 patients had recurrent angina and 2 patients had MI. Optimal medical therapy was applied in 10 patients and of those 5 patients had recurrent angina, 4 patients had a MI and 1 patient died. Of 61 patients, 47 did not have ischemia during 1-year follow-up. Of these, 37 patients had OMT and 10 patients had PCI. In the group treated conservatively (OMT), 6 patients during the 1-year mark had frequent attacks of angina while 7 pts in the PCI group had angina attacks. Survival analysis showed significant benefit over time among patients with presence of reverse redistribution (Table 3 and Figure 3). In scintigraphic findings, reverse redistribution showed 87% (95% CI: 72%-90%) benefit when compared to patients with scarring over time.
Hazard ratios for presence of reverse distribution.

MI: myocardial infarction; HR: hazard ratio; CI: confidence interval.
Models accounted for sex and age.

Survival curves showing survival probabilities over time (in days) among patients with the presence of reverse redistribution.
Discussion
Percutaneous coronary intervention (PCI) is the most commonly performed medical procedure in acute coronary syndrome.3,15,16 Currently, there is no consensus about providing optimal treatment for patients with chronic coronary heart disease. Our findings suggest that depending on clinical symptoms, patients’ functional status, and the anatomical complexity, stable CAD can have better prognosis in presence of reverse redistribution. In patients with stable CAD, it is common to have discordant findings between anatomical imaging of coronary vessels and their functional ability to maintain viable myocytes. In this regard, the ESC recommended postponing invasive treatment in patients with discrepancies between anatomical and functional characteristics of the coronary vessels, and it has recommended the use of non-invasive procedures to assess myocardial functionality with respect to culprit vessels within multi-disciplinary “Heart Team.”1,4 The “DEFER” and “FAME” studies have confirmed that the concept of avoiding unnecessary stent implantation using the above-mentioned functional method resulted in better outcomes.17-19 The “COURAGE” study showed that the OMT as initial form of treatment in patients with stable angina pectoris is equally effective in reducing the risk of death, MI or other major cardiovascular events as the combination of PCI plus medical treatment.5,20 When exploring scintigraphic characteristics of myocardial segments in the supply area of significantly stenosed coronary arteries, we found almost identical angiographic findings for different scintigraphic findings (reversible defect, irreversible defect, partially reversible defect, and reverse redistribution). Opposite was also true, for various coronarographic findings, we found very similar scintigraphic patterns. This fact suggests key difference between anatomical (angiography) and functional (scintigraphic) imaging. This is a starting point and a source of ideas on the possible inclusion of specific findings observed among the tools in the decision to proceed with the treatment of patients with CAD.
Results of diagnostic coronary angiography are anatomical data that illustrate the degree of narrowing of the coronary arteries, but it may not be precise since it is a visual assessment. On the other hand, functional scintigraphy images, the living cells regardless of the associated coronary anatomy and the goal of each method is to evaluate myocardial ischemia and not only the epicardial artery patency.21-23 In support of scintigraphy as a functional method, there is the fact that 201Tl is an analog of potassium which means that the mechanisms of movement and biodistribution in cells or tissues of both elements is identical and that the normal distribution of 201Tl in myocardial cells reflects healthy tissue and conversely, abnormal biodistribution reflects scarring or myocardial ischemia. 24
Scintigraphic viability of ischemic and partially ischemic (reversible and partially reversible defects) myocardial segments becomes obvious after revascularization procedures. Myocardial segments presenting with reverse redistribution of 201Tl exhibit good response to optimal medical therapy. Almost identically narrowed coronary epicardial arteries and well-developed collateral circulation that not only represent different scintigraphic characteristics related segments, but more importantly beyond the specific findings observed can expect better functional parameters. Results indicate better outcomes with PCI as compared to OMT in cases of scintigraphic findings of ischemia and angiographically proven significant stenosis despite well-developed collateral circulation. In the subgroup of patients with reverse redistribution on scintigraphic images, there was a significantly better exercise tolerance, EF, wall motion parameters, a lower degree of myocardial necrosis and a smaller number of ischemic attacks during one year follow-up. Results also suggest that OMT should be preferred over invasive therapeutic procedures in patients with scintigraphic finding of reverse redistribution regardless of coronary angiography. Research by Nudi et al also suggests that prognosis is better among patients with revascularization, but, they also emphasize the importance of focusing on necrosis, which is easier to define and irreversible, rather than viability, which is much more complex to define, and more prone to confusion. In addition, Nudi et al25-27 suggests that necrosis is much more stable, and obviously unlikely to benefit from revascularization.
In this case, the scintigraphic reverse redistribution pattern as an indicator of functional collaterals could serve as a new tool for making treatment decisions. Functional evaluation of myocardial segments by scintigraphic method describes functional significance as opposed to anatomical significance expressed in percent narrowing of the vascular lumen. Heart contractility and ejection ability can be preserved thanks to collateralized cardiac segments despite significant coronary artery stenosis. Results of our study indicate the need for scintigraphic evaluation of myocardial segments before making treatment decisions which is in line with the recommendation of the ESC.1,4
Conclusion
Scintigraphic pattern of reverse redistribution of 201Tl as an indicator of successful natural bypasses (collaterals) may be used as an additional help in the choice of therapy in patients with chronic coronary heart disease. In such cases, functional collateral vessels should perhaps be kept patent by not performing revascularization procedure. If functional parameters and quality of life in terms of absence of new ischemic attacks during the one year-follow-up in patients with such scintigraphic pattern indicate stability of CAD then, clinicians may expect better prognosis in their patients.
Footnotes
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Contributions
IJ conceptualized the study, supervised the project, and wrote the first draft of the manuscript. EF, DP, BS, AP, DH, MH, DR, DM, MV, and IV contributed to data collection, and revision of the manuscript. IJ, DM, MV, and IV contributed to further interpretation of the results. AS conducted the analysis and contributed to critical revision of the manuscript. All the authors have read and approved the final manuscript.