
Abstract
Background:
Intermittent claudication (IC) is traditionally managed with risk factor modification, best medical treatment (BMT), and exercise training. Comorbidities such as diabetes and ischemic heart disease affect both results of invasive treatment and health-related quality of life (HRQoL) negatively. It is unknown how chronic widespread pain (CWP) influences the results of invasive treatment. We evaluated the influence of CWP on HRQoL in patients undergoing invasive (open surgery or endovascular treatment) and noninvasive BMT of IC.
Methods:
A total of 242 patients with IC treated with invasive or noninvasive methods responded to the validated HRQoL questionnaires Short Form 36 Health Survey, EuroQoL 5-dimensions, and distribution of pain with the Epipain questionnaire at baseline and after 12 months.
Results:
Invasively treated patients without CWP improved in all primary outcome measures. Patients with CWP reported significant improvements in most of the HRQoL-related outcome measures after invasive treatment, but patients with CWP in the noninvasive treatment group did not improve in any HRQoL-related outcome measure.
Conclusions:
The presence of CWP not should be a cause to withhold invasive treatment in patients with IC.
Introduction
Intermittent claudication (IC) is a common disorder, with a prevalence of 6.5% in women and 7.2% in men aged 60 to 90 years in Sweden 1 and affecting 20 to 40 million individuals worldwide. 2 First-line management of IC traditionally consists of risk factor modification, best medical treatment (BMT), and exercise training. 3 Results of invasive IC treatment are better in patients with suprainguinal lesions than in those with infrainguinal. 4
Chronic pain (defined as pain with duration of 3 months or more) has a prevalence of 30% to 50% in the general population. 5 Regarding distribution of musculoskeletal pain in the body, a distinction is often made between chronic regional pain (CRP) and chronic widespread pain (CWP). Chronic regional pain is more common with a prevalence of 24%, whereas CWP occurs with a prevalence of 11%. 5
Among patients with peripheral arterial disease (PAD), the prevalence of CWP is almost 2 times higher than in the general population. 6 Invasive treatments of patients with PAD, IC, and critical limb ischemia lead to significant improvement in HRQoL. 7
Patients with IC caused by lesions in the superficial femoral artery (SFA) experience significant improvement in HRQoL, ankle-brachial index (ABI), and walking distance (WD) 12 months after primary endovascular stenting compared with patients treated conservatively with BMT. 6
It is unknown to what extent the presence of CWP influences the results of invasive treatment in patients with IC in terms of HRQoL, and how noninvasive treatment influences HRQoL in IC patients with and without CWP. At present, we do not know whether comorbidity such as CWP should be regarded as a reason to avoid or to recommend invasive treatment.
The aim of this study was to evaluate the impact of CWP on HRQoL in patients with IC subjected to conservative or invasive treatment, to improve patient selection for invasive treatment of IC.
Methods
Ethics
Informed consent was obtained in accordance with the ethical standards of the Helsinki Declaration of 1975, and the study was approved by the Ethics Committee at Lund University (ref. nos 2010/549 and 2016/827).
Patient characteristics
This was a 12-month retrospective follow-up study of 242 patients from 2 prospectively collected study cohorts.6,7 In total, 100 patients with infrainguinal IC prospectively randomized to either invasive treatment (stent treatment of lesions in the SFA; n = 48) or noninvasive treatment (BMT alone; n = 52) 6 were analyzed together with 142 IC patients from another prospective study originally consisting of 240 consecutive patients with symptomatic PAD planned for invasive treatment (open surgery or endovascular treatment). 7 Study designs have been reported in detail.6,7
Data collection/questionnaires
All study subjects, from both initial trials, responded to the same below described HRQoL questionnaires, and distribution of pain was assessed with the Epipain questionnaire concerning musculoskeletal pain at baseline and after 12 months. 5 Based on a key question on pain for 3 months or more, and a pain drawing with predefined body regions, patients with CWP were identified as those reporting pain in 2 contralateral body quadrants (right or left and above or below the waist) and the axial skeleton (spine or anterior chest) for 3 months or more. Those reporting pain for at least 3 months but not fulfilling CWP criteria were designated as having CRP. Those with no pain or pain duration less than 3 months were regarded as having no chronic pain (NCP). 7 Main outcome measure was HRQoL assessed with the generic instruments Short Form 36 Health Survey (SF-36) 8 and EuroQoL 5-dimensions (EQ5D), 9 and the PAD-specific Walking Impairment Questionnaire (WIQ). 10 The SF-36 rates HRQoL 0 to 100 (worst to best) in 8 domains; WIQ rates 0 to 100 (worst to best). 10 The HRQoL in patients fulfilling criteria for CWP was compared with NCP and CRP (together classified as non-CWP).
Secondary outcome measures were ABI and WD.
Statistics
The sample size was determined to study a clinically relevant difference between the groups regarding the primary outcome variable, HRQoL. With a significance level of 5%, a difference of 10 points in SF-36 could be detected with a power of at least 80%.
Patient characteristics including pain group category and results from the HRQoL questionnaires (commonly analyzed with parametric methods) were analyzed, using SPSS 20.0 (SPSS Inc., Chicago, IL, USA). The HRQoL data are reported as mean (SD). Student t test and paired t tests were used to evaluate differences in continuous variables, and the χ2 test was used to evaluate group differences in nominal variables, between baseline and follow-up regarding treatment modality and pain group affiliation.
Comparisons were performed at the 5% significance level based on 2-sided tests. Results are presented with 95% confidence intervals and P values.
Results
Baseline
A total of 242 patients with IC (78 due to suprainguinal lesions and 164 due to infrainguinal lesions) entered the study. At baseline, 75 patients (31%) reported CWP, 167 patients (69%) reported non-CWP (CRP: 132, NCP: 35). Characteristics and baseline demographics of all 242 patients are presented in Table 1.
Characteristics of 242 patients with intermittent claudication (IC) with or without chronic widespread pain (CWP).

Abbreviations: B, blood; HDL, high-density lipoprotein; LDL, low-density lipoprotein; P, plasma; S, serum.
Mean (SD) or No. (%).
In all, 185 patients were treated invasively, and 57 patients were treated conservatively with BMT alone (Table 2).
Baseline values of primary and secondary outcome measures in patients with intermittent claudication (IC) treated invasively (invasive group, n = 185) or with best medical treatment alone (noninvasive group, n = 57) regarding presence of chronic widespread pain (CWP) or not (non-CWP).
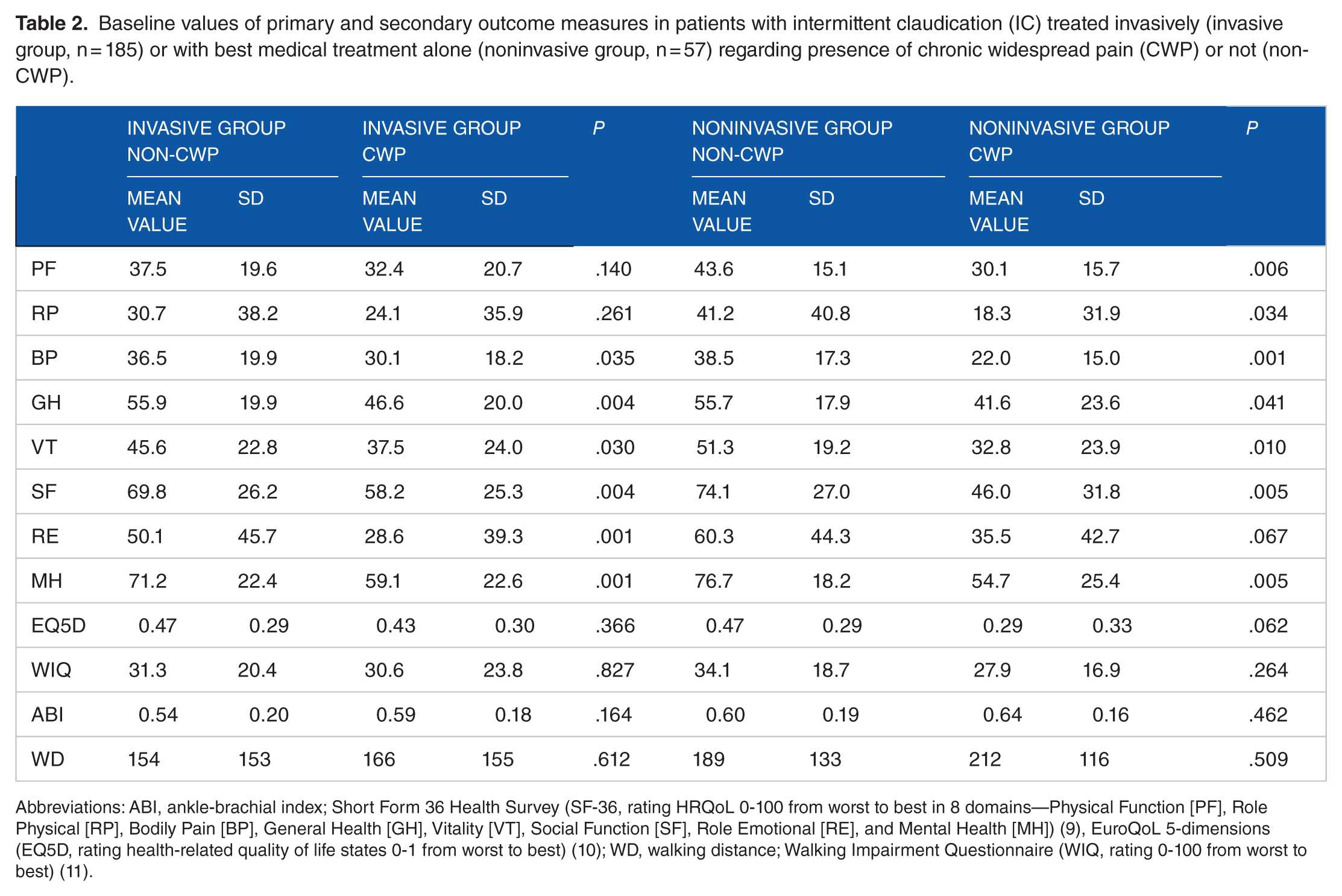
Abbreviations: ABI, ankle-brachial index; Short Form 36 Health Survey (SF-36, rating HRQoL 0-100 from worst to best in 8 domains—Physical Function [PF], Role Physical [RP], Bodily Pain [BP], General Health [GH], Vitality [VT], Social Function [SF], Role Emotional [RE], and Mental Health [MH]) (9), EuroQoL 5-dimensions (EQ5D, rating health-related quality of life states 0-1 from worst to best) (10); WD, walking distance; Walking Impairment Questionnaire (WIQ, rating 0-100 from worst to best) (11).
Among invasively treated patients, those with CWP reported significantly lower baseline values of SF-36; BP, GH, VT, SF, RE, and MH scores than patients without CWP, and corresponding differences were seen among noninvasively treated patients concerning baseline SF-36; PF, RP, BP, GH, VT, SF, and MH (Table 2), whereas no such differences were seen for EQ5D or WIQ.
12 months
After 12 months, patients in the invasively treated group without CWP at baseline improved in all outcome measures and those with CWP at baseline improved in all outcome measures except SF-36 domains GH and MH. Noninvasively treated patients without CWP at baseline improved in SF-36 domains PF, EQ5D, WIQ, ABI, and WD, whereas those with CWP at baseline showed unchanged scores in all outcome measures (Figure 1).

Changes between baseline and 12 months in primary outcome measures in patients with intermittent claudication (IC) treated invasively (invasive group, n = 185) or with best medical treatment alone (noninvasive group, n = 57) regarding presence of chronic widespread pain (CWP) or not (non-CWP) at baseline.
After 12 months, patients without CWP reported significantly higher values than those with CWP concerning all outcome measures except ABI and WD in both treatment groups (Table 3). Lesion characteristics in terms of supra- or infrainguinal localization did not influence the primary outcomes.
The 12-month values of primary and secondary outcome measures in patients with intermittent claudication (IC) treated invasively (invasive group, n = 185) or with best medical treatment alone (noninvasive group, n = 57) regarding presence of chronic widespread pain (CWP) or not (non-CWP) at baseline.

Abbreviations: ABI, ankle-brachial index; Short Form 36 Health Survey (SF-36, rating HRQoL 0-100 from worst to best in 8 domains—Physical Function [PF], Role Physical [RP], Bodily Pain [BP], General Health [GH], Vitality [VT], Social Function [SF], Role Emotional [RE], and Mental Health [MH]) (9), EuroQoL 5-dimensions (EQ5D, rating health-related quality of life states 0-1 from worst to best) (10); WD, walking distance; Walking Impairment Questionnaire (WIQ, rating 0-100 from worst to best) (11).
Discussion
This study evaluated the impact of CWP on treatment results in patients with IC. Patients with CWP showed significant lower values of HRQoL before treatment. Invasive treatment of IC resulted in significant improvement in both primary and secondary outcome measures after 12 months irrespectively of presence of CWP at baseline or not. After intervention, patients with CWP still scored significantly lower in almost all outcome measures compared with patients without CWP. Noninvasively treated patients without CWP improved significantly in several outcome measures (SF 36 domain PF, EQ5D, WIQ, ABI, and WD), whereas noninvasively treatment in patients with CWP had a less successful outcome, without improvement in any outcome measure.
Invasive treatment improved HRQoL in patients with IC and concomitant CWP but to a lower level compared with those without CWP. This is consistent with results previously reported in patients with PAD of all severities. 7 The present finding of lack of impact on HRQoL in noninvasively treated patients with IC and concomitant CWP has previously not been demonstrated. Other comorbid conditions such as diabetes, ischemic heart disease, and chronic obstructive pulmonary disease are known to affect both results of invasive treatment and HRQoL negatively in patients with PAD 11 and might therefore be considered as contraindications for intervention in some cases. The risk of bias caused by the fact that our results are based on patients from 2 originally separated small study cohorts merged together constitutes a limitation of our study. However, categorization of pain groups and evaluations of HRQoL were performed identically in all patients reported. The high number of comparisons made in the study increases the risk of rejecting a true null hypothesis, and caution is necessary when interpreting the actual significance of P values.
The prevalence of CWP in patients with IC was high (28%) compared with 11% in the general population. 5 A high proportion of CWP has also been seen in other chronic painful conditions such as rheumatoid arthritis, osteoarthritis, endometriosis, and ulcerative colitis. 12 It is not known whether this is due to a sensitization of the nervous system due to chronic nociceptive pain or if there is another common background or vulnerability explaining the coexistence of CWP with these disorders. As in this study, CWP adds to the burden of the disease with a lower self-reported HRQoL. 13 Interestingly, also patients with CWP improved in the invasively treated group but not in the noninvasively treated group, indicating that the presence of CWP not should be a cause to withhold invasive treatment.
Conclusions
Invasively treated patients without CWP improved in all outcome measures and invasively treated patients with CWP reported significant improvements in most of the HRQoL-related outcome measures, whereas patients with CWP in the noninvasive treatment group did not improve in any HRQoL-related outcome measure at all. In conclusion, the presence of CWP should not be a cause to withhold invasive treatment in patients with IC.
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The 2 original studies were supported by a grant from Stig and Ragna Gorthons Foundation, Helsingborg; the Ernhold Lundström Foundation; Research Funds at Skåne University Hospital; the Albert Påhlsson Foundation; the Hulda Ahlmroth Foundation; and from the Swedish state under the LUA/ALF agreement.
Declaration Of Conflicting Interests:
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: A.G., S.B., and H.P. have nothing to disclose. H.L. has received compensation according to a proctoring and training agreement with Covidien AB and William Cook Europe ApS; however, these companies had no involvement in any part of this study.
Author Contributions
HL performed conception and research design, data analysis and data interpretation, wrote manuscript and acted as corresponding author.SB supervised concept and helped in data interpretation.
SB, AG, HP performed critical manuscript evaluation. All the authors reviewed and approved the final manuscript.