
Abstract
Background:
Rheumatoid arthritis (RA) disease activity, associated comorbidities, and therapy-related side effects impair the physical, social, and emotional dimensions of the patient’s health. Presently, the ongoing COVID-19 pandemic has been associated with a broad range of psychosocial disorders in various populations. Patients with RA are especially vulnerable to such effects.
Objectives:
Detect the prevalence of recent COVID-19 infection among patients with RA, assess depression and anxiety in these patients and their associated factors during the COVID-19 pandemic and their potential relation to disease activity.
Design and Methods:
This is a cross-sectional study conducted on 120 adult Egyptian patients diagnosed with RA during the COVID-19 pandemic. The prevalence of recent COVID-19 infection among the patients was evaluated. The patients underwent psychological assessment using the Hamilton Depression Rating Scale (Ham-D) and the Hamilton Anxiety Rating Scale (Ham-A) to measure levels of depression and anxiety levels. The RA disease activity was assessed using Disease Activity Score (DAS) Das-28-ESR.
Results:
This study encompasses a total of 120 RA patients. The prevalence of patients with a recent history of COVID-19 infection was 40.8%. Both groups exhibited significantly elevated mean scores on the Das-28-ESR scale and also scored higher on measures of depression and anxiety. Interestingly, the COVID-19 group exhibited a higher percentage of unmarried individuals, had educational attainment below the university level, and were unemployed. Patients with recent COVID-19 had significantly lower numbers of children, higher disease duration, higher Das-28-ESR scores, and elevated depression and anxiety scores. The statistical analysis revealed that the COVID-19 infection and disease duration were significant predictors of depression and anxiety. The results also exhibited that the depression score was positively correlated with age and DAS scores.
Conclusions:
It was observed that patients diagnosed with RA revealed a higher prevalence of COVID-19 infection. The occurrence of depression and anxiety was observed to be widespread among patients diagnosed with RA and, more significantly, prevalent in RA patients who had a recent COVID-19 and had a higher level of disease activity. The occurrence of COVID-19 and disease duration were identified as factors that can anticipate the development of depression and anxiety.
Introduction
Rheumatoid arthritis (RA) is an autoimmune condition causing long-term symmetrical small-joint inflammation, progressing to larger joints. It also affects the eyes, skin, kidneys, lungs, and heart. 1 Rheumatoid arthritis disease activity, therapy-related side effects, and associated comorbidities impair the physical, social, and emotional dimensions of the patient’s health.2,3
Despite underestimating psychological health issues,4,5 rheumatic patients have elevated rates of anxiety and depression.4-7 Research shows a prevalence of RA-associated depression ranging from 6% to 66% and anxiety ranging from 2.5% to 70%.8-11
The new Coronavirus Disease 2019 (COVID-19) unprecedentedly evolved and challenged health care systems with a specific impact on patients with long-term conditions. 12 Rheumatoid arthritis patients were affected by the partial or total closure of outpatient clinics that was applied during the pandemic and negatively affected disease management 13 and aggravated the RA-related psychological burden, paralleled with the pandemic-associated psychological impact due to social distancing and the fear of contracting the disease. 14 In addition, the governmental authorities and the Centers for Disease Control and Prevention (CDC) have also highlighted that COVID-19 implies a threat to patients with long-term and autoimmune disorders. 15
Currently, there is a shortage of research examining the prevalence and impact of anxiety and depression related to COVID-19 among individuals in Egypt who have been diagnosed with RA. Hence, the primary objective of this study was to detect the prevalence of recent COVID-19 infections among patients with RA and evaluate the levels of anxiety and depression among individuals diagnosed with RA during the COVID-19 epidemic and to examine the potential association between these psychological states and the severity of the disease.
Patients and Methods
Study design
This study is a cross-sectional study conducted in the rheumatology outpatient clinics and rheumatology inpatient wards of El-Demerdash Hospital and Kobry Al-Kobba Hospital in Egypt from March 2021 to March 2022.
The prevalence of depression and anxiety among Egyptian patients with RA presenting to a university hospital was 15.29%. 16 Hence, to maintain the actual prevalence within a range of ±6.45% from the observed value, a sample size of at least 120 would be required, considering a 6.45% margin of error and a 95% confidence level while assuming a population proportion of 15.29%. The authors followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Guideline.
Study participants
Inclusion criteria: The study randomly selected 120 adult Egyptian participants with RA diagnosis according to the 2010 guidelines set forth by the American College of Rheumatology/European League Against Rheumatism (ACR/EULAR). 17 The patients may have a history of recovery from COVID-19, with a time frame not exceeding 3 months from the initial contraction of the infection.
The exclusion criteria: patients with other connective tissue diseases, severe psychological disorders, comorbid substance use disorder, intensive care unit (ICU) admission or ventilation due to COVID-19 infection, exceeding 3 months from starting condition of COVID-19, thyroid disorders or long-term disabling diseases. All participants provided written informed permission before the study began.
Procedures
Data collection
All patients received a comprehensive assessment of their medical history, including factors such as the age at which the RA first emerged, the disease duration, and any previous medical treatment received.
The patients were surveyed to identify the occurrence of recent COVID-19 infection in the patients, adhering to the COVID-19 case standards specified in Egypt’s Ministry of Health COVID-19 management protocol. 18 The participants were divided into 2 clear groups. The first group (namely group I) consisted of individuals with both RA disease and a recent recuperation from COVID-19 infection, occurring within 3 months from the point of contracting the virus. The second group (namely, group II) comprised RA patients who had not previously contracted COVID-19.
Psychiatric assessment
Depression severity was assessed using the validated Arabic version of Hamilton Depression Rating Scale (Ham-D). This scale consists of 17 elements, with 8 being assessed on a 5-point scale and 9 on a 3-point scale. Ratings between 0 and 7 correspond to a normal state, 8 to 13 signify mild depression, 14 to 18 indicate moderate depression, 19 to 22 suggest severe depression, and scores exceeding 23 represent severe depression.19,20
The severity of anxiety among the participants was evaluated using the validated Arabic version of Hamilton Anxiety Rating Scale (Ham-A). This scale comprises 14 items that assess both physical and psychological anxiety symptoms. Each item is ranked on a 5-point scale. The overall score can vary between 0 and 56, with a score of 17 or below suggesting mild anxiety, a score between 18 and 24 indicating mild to moderate anxiety, and a score of 25 to 30 pointing toward moderate to severe anxiety.21,22
Assessment of RA disease activity
The RA activity was assessed using the DAS-28-ESR score, which determines the RA disease activity in the 28 joints based on the erythrocyte segmentation rate. Data were computed using the website calculator (http://www.das-score.nl/das28). Categorization of patients was determined by their DAS-28-ESR score: patients were considered in remission if their score was ⩽2.6, classified as having low disease activity if the score was >2.6 to <3.2, categorized as having moderate activity if the score was >3.2 to ⩽5.1, and classified as having high activity if the score exceeded 5.1. 23
Statistical analysis
Data analysis was performed using SPSS version 28 (IBM, Armonk, New York, United States). Normality was evaluated for quantitative data using Kolmogorov-Smirnov test and direct data visualization methods. After conducting tests for normality, numerical data were summarized using means with standard deviations or medians with ranges. Numbers and percentages were used for categorical data. Quantitative data were compared to COVID-19 status using an independent t-test (for variables with normal distribution) or Mann-Whitney U test (for variables without normal distribution). The chi-square test was employed for categorical data comparisons. Pearson’s or Spearman’s correlation coefficients were used for conducting correlation analyses. In addition, a multivariate linear regression analysis was applied to predict depression and anxiety scores, and the corresponding regression coefficients were calculated at a 95% confidence level. All statistical tests were conducted as 2-sided tests, with statistical significance attributed to P values below .05.
Study outcome(s)
The primary outcome was the prevalence of recent COVID-19 infections among patients with RA and to assess the levels of anxiety and depression in this patient diagnosed with RA, while the secondary outcome was the features of patients with RA based on their COVID-19 status. The investigation of the relationship between depression and anxiety with both COVID-19 and disease activity and the identification of factors that could predict the presence of depression and anxiety in the patients under study.
Results
The demographic and clinical characteristics of the patients under study
The demographic information of the patients is presented in (Table 1). During the study period, 120 patients were eligible for the study. The patients’ mean age was 50 ± 6 years. Females predominated in this study were 89.2%. Most of the patients (76.7%) were married. More than half of the sample received a university education and were employed by 54.2% and 57.5%, respectively. The children ranged from 0 to 4, with a median of 2. The median disease duration was 6 years, from 1 to 19 years. The mean DAS score was 3.93 ± 0.92. The mean depression and anxiety scores were 13 ± 5 and 22 ± 6, respectively (Table 1).
General characteristics of the studied patients.

Abbreviation: DAS, Disease Activity Score.
Data were presented as mean ± standard deviation; Median (min-max) or number (percentage).
Patients’ characteristics according to the presence of COVID-19
Forty-nine patients (40.8%) had recently recovered from COVID-19 infection and constituted the COVID-19 group (Group I). The non-COVID-19 group included 71 patients (59.2%) (Group II). The COVID-19 group had a significantly higher percentage of unmarried patients (P = .003), patients with below university education (P = .015), and unemployed patients (P = .002). In addition, the COVID-19 group demonstrated significantly higher disease duration (P = .047), DAS score (P < .001), and depression and anxiety scores (P < .001 for each) (Table 2, Figure 1). In contrast, the number of children was significantly lower in the COVID-19 group (P = .03). No significant difference was observed regarding age (P = .479) or sex (P = .679) (Table 2).
Patients’ characteristics according to COVID 19 infection.
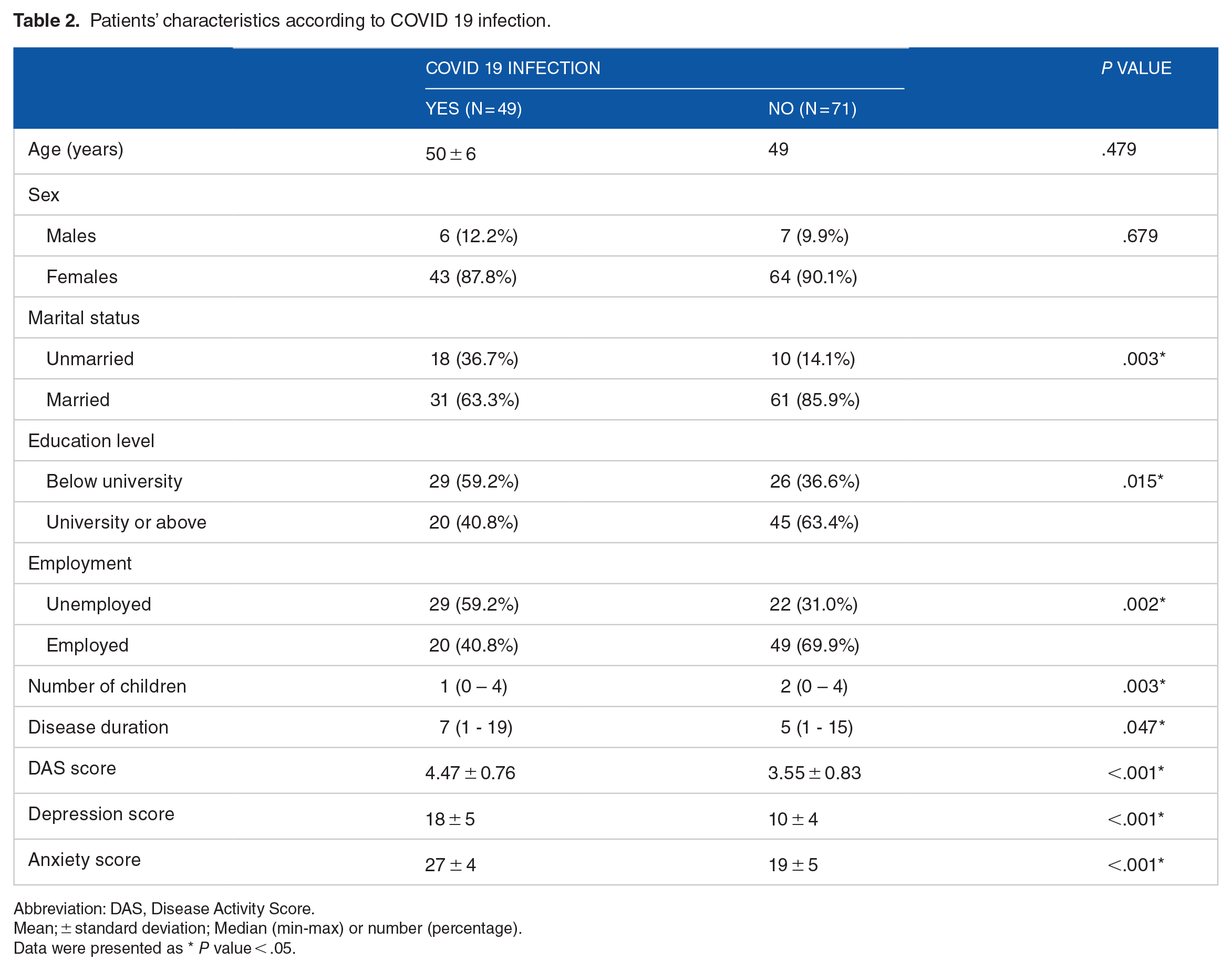
Abbreviation: DAS, Disease Activity Score.
Mean; ± standard deviation; Median (min-max) or number (percentage).
Data were presented as * P value < .05.

Depression and anxiety scores according to COVID 19 infection.
Correlation between depression and anxiety scores with other parameters
Depression score was positively correlated with age (r = .368, P < .001) and DAS score (r = .656, P < .001). Also, anxiety score was positively correlated with age (r = .393, P < .001) and DAS score (r = .633, P < .001) (Table 3, Figure 2).
Correlation between depression and anxiety scores with other parameters.

Abbreviation: DAS, Disease Activity Score.
r: Correlation coefficient * Significant.

Correlation between depression and anxiety scores with DAS score. DAS indicates Disease Activity Score.
Predictors of depression score
Multivariate linear regression analysis demonstrated that COVID-19 (B = 5.41, 95% CI: [4.13, 6.7], P < .001) and disease duration (B = 0.85, 95% CI: [0.66, 1.04], P < .001) were significant predictors of depression score (P < .001) (Table 4).
Multivariate linear regression analysis for the prediction of depression score.

Abbreviation: DAS, Disease Activity Score; B, regression coefficient; 95% CI, 95% confidence interval.
Significant.
Predictors of anxiety score
Multivariate linear regression analysis demonstrated that COVID-19 (B = 4.68, 95% CI: [2.93, 6.42], P < .001) and disease duration (B = 0.59, 95% CI: [0.33, 0.84], P < .001) were significant predictors of anxiety score (Table 5).
Multivariate linear regression analysis for prediction of anxiety score.
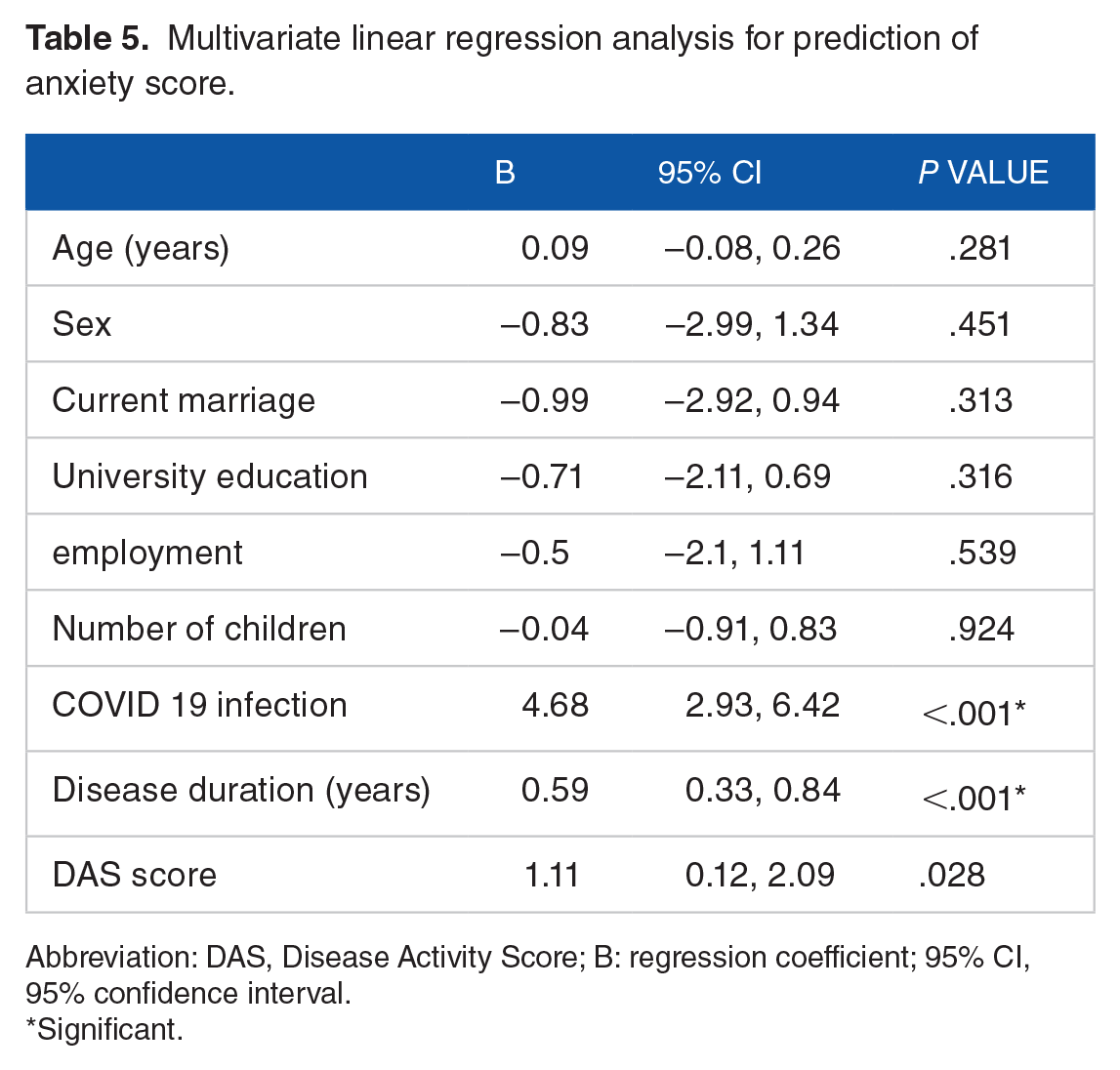
Abbreviation: DAS, Disease Activity Score; B: regression coefficient; 95% CI, 95% confidence interval.
Significant.
Discussion
The ongoing COVID-19 pandemic is associated with various psychosocial disorders in multiple populations.24-26 Patients with RA are vulnerable to psychological changes such as depression and anxiety that could result in pain persistence despite disease control with drugs.
This study included 120 RA patients recruited from Kobry Al-Kobba Hospital and El-Demerdash Hospital rheumatology outpatients and inpatient wards. These hospitals lie in the center of Cairo, the Egyptian capital, with a catchment area encompassing almost one-third of Greater Cairo and covering urban and rural areas. The prevalence of the patients who had a recent history of COVID-19 in this study was 40.8%. The significantly high incidence seen in this study can be attributed to the occurrence of at least 4 waves of COVID-19 over the study period. 27 Moreover, RA patients are more vulnerable to severe acute respiratory syndrome coronavirus disease 2 (SARS-CoV-2) infection. England et al 28 reported that COVID-19 risk is 25% higher in RA patients than in non-RA patients. This increased risk could be explained by the RA-associated immune dysregulation, the RA therapy, including disease-modifying antirheumatic drugs (DMARDs) and corticosteroids, and the frequently developed comorbidities associated with RA.29,30 The COVID-19 pandemic has not only brought about physical health risks due to the increased prevalence of long-term illnesses but has also had a detrimental impact on individuals’ mental well-being. 31
Concerning the sociodemographic and clinical features of the patients, the COVID-19 group exhibited a statistically significant increase in the proportion of unmarried individuals, patients with educational attainment below the university level, and unemployed patients. In addition, the COVID-19 group had fewer children but higher disease activity, as represented by the Das-28-ESR score and disease duration. These findings partially align with Batty et al, 32 who reported higher risks of COVID-19 in patients with disadvantaged education levels and occupations. Differences in compliance and adherence to the protective measures might explain the significant association between the COVID-19 occurrence and described patients’ sociodemographic parameters.
The studied groups differed significantly in the Das-28-ESR score, which aligns with the few available data in the literature. Evidence suggests that respiratory viral infection can result in a disease flare. 33 In addition, COVID-19 may worsen RA conditions.34,35 Direct SARS-CoV-2 infection affects the synovium, cortical bone, and skeletal muscle. Moreover, SARS-CoV-2-associated cytokines activation predisposes to inflammatory chondrolysis, 36 and these cytokines are involved in RA pathogenesis. Furthermore, social isolation with the stress of fearing the poor outcome in RA patients with SARS-CoV-2 infection could elucidate the causes of such differences. 34 It is worth noting that both groups had mean DAS-28-ESR values indicating moderate disease activity. This is not surprising since RA patients have been impacted during the pandemic by drug shortages, limited health care access, telemedicine, and social isolation. These factors could lead to accentuation of the disease activity. 34
This study demonstrated high mean depression and anxiety scores in the patients. Several studies from Egypt, India, Iran, and China showed high depression and anxiety levels in RA patients.11,37-39 In a review study, Gettings 40 analyzed the RA-associated psychological impact and assumed that disease-related disabilities, pain during disease activity, and other social difficulties plausibly explain the high anxiety and depression levels in RA patients.
The COVID-19 group revealed significantly higher depression and anxiety scores in this study. This finding is primarily due to the summated psychological burden of COVID-19 and the RA itself. The well-documented COVID-19-associated psychological disorders are further augmented in RA patients due to their accentuated fear caused by being more predisposed to infection-related poor outcomes and mortality.
These findings align with Mancuso et al, 41 who revealed higher anxiety and stress in rheumatic disease with COVID-19. In addition, social distancing and patient isolation lead to the loneliness that might exacerbate depression and anxiety. 34
This study revealed that depression and anxiety scores were positively correlated with age and Das-28-ESR score. In contrast, according to previous studies, depression and anxiety are associated with young age in RA patients.42,43 This discrepancy could be due to the differences in study cohorts and timing. Our study included patients who had a recent history of COVID-19 infection and was performed during the pandemic. As a result, old patients encountered higher fear and stress, being more susceptible to infection and infection-related poor outcomes. Several studies support the positive correlation between depression and anxiety scores with disease activity.42-44 Higher disease activity leads to higher disability and pain severity. Rheumatoid arthritis disease duration was a predictor of depression and anxiety in this study, which may be related to higher RA-related comorbidities and disabilities. This aligns with the findings of Tee et al’s 31 research in 2020, which indicated that factors contributing to negative mental health effects amidst the COVID-19 pandemic encompassed the coexistence of conditions like hypertension and asthma, along with the manifestation of distinct symptoms such as myalgia, cough, breathing difficulty, dizziness, and a sore throat.
This study adds to the evidence of the adverse clinical and psychological impact of COVID-19 on RA patients. Patients with RA should receive particular concern during global health crises such as the COVID-19 pandemic. Routine screening for the psychological well-being of RA patients, including depression and anxiety, is recommended, and preventing infection in such patients should be a high priority.
Online platforms and applications are harnessed by digital cognitive therapy to deliver therapeutic aid and interventions at a reasonable cost. This approach presents practicality, ease of use, and confidentiality, rendering it a viable choice for individuals coping with long-term illnesses amidst the pandemic.45,46
The stress and uncertainty of the pandemic can disturb sleep schedules, causing challenges in initiating or maintaining sleep. There is encouraging evidence that digital cognitive therapy, particularly Digital Cognitive Behavioral Therapy for Insomnia (dCBT-I), has exhibited positive outcomes in addressing insomnia. 47
Effectively managing anxiety and panic during the pandemic necessitates a comprehensive strategy. This entails using digital therapeutic alternatives, engaging in self-care practices such as mindfulness and relaxation routines, adhering to a consistent schedule, finding social support in virtual communities, and staying updated through trustworthy sources. Through the integration of a holistic method and the utilization of digital cognitive therapy, individuals grappling with long-term illnesses can adeptly handle their mental health, diminish anxiety and panic, and improve their overall well-being throughout these demanding periods, incorporating cognitive behavioral therapy (CBT) and mindfulness-based cognitive therapy (MBCT). 46
Strengths and Limitations
One notable quality of this study is its unique contribution to the existing literature, as it represents one of the limited numbers of studies that have examined the impact of COVID-19 on the psychological well-being of patients diagnosed RA.14,48 We acknowledge that our research is constrained by the absence of an evaluation of other variables and the absence of categorizing the COVID-19 group according to severity. Furthermore, the examination of various therapy modalities was not addressed. Nevertheless, these drawbacks should not undermine the value of this study. Doing more research to address the existing restrictions in the present work context is recommended.
Conclusions
The occurrence of COVID-19 infection is heightened among individuals with a diagnosis of RA. Depression and anxiety are frequently observed in individuals with RA, and these conditions are even more prevalent in those with both RA and recent COVID-19 infection. Furthermore, individuals with a history of COVID-19 in addition to RA tend to demonstrate increased disease activity. The occurrence of COVID-19 and disease duration have been identified as significant predictors of depression and anxiety in patients diagnosed with RA. These findings emphasize the importance of closely monitoring and addressing mental health concerns in RA patients, particularly those affected by COVID-19.