
Abstract
Introduction:
The estimated prevalence of gout in Western societies is 2.7% to 6.7%. In Australia, there have been increasing rates of hospitalisations for gout flares. Urate-lowering therapy (ULT) is effective in reducing urate burden, which can prevent gout flares and destructive arthropathy. This study assessed the representation rate of patients presenting to the Emergency Department (ED) with crystal arthropathy and the utilisation of ULT in the community for patients with a pre-existing history of gout.
Methods:
A retrospective review of electronic records of patients presenting to the ED from the Illawarra Shoalhaven Local Health District was performed. Patients included were coded as per the 10th revision of the International Classification of Diseases coding for crystal arthropathy
Results:
In all, 18.8% of all crystal arthropathy encounters to the ED were repeat presentations. Of the 70% of patients with a history of gout, only 30.8% were on ULT.
Discussion:
Despite evidence-based recommendations for a ‘treat-to-target’ approach, most patients with a previous history of gout were not on ULT. One in five encounters were re-presentations for crystal arthropathy. Effective adherence to treatment guidelines may reduce the number of repeat encounters for gout flare in the ED.
Introduction
Crystal arthropathy is the most common form of inflammatory arthritis affecting adults. Gout is caused by the chronic deposition of monosodium urate (MSU) crystals both in and around joints. This can lead to progressive joint damage and is also associated with an increased risk of developing cardiovascular disease.1,2 The prevalence of gout in Australia is estimated to be 0.8% based on self-reported surveys, although this is likely to be an under-representation of the actual prevalence.1,3 Gout poses a significant burden to the Australian health care system, estimated to cost $17.5 million in 2015, including $35 million in General Practice consultations and $ 8 million in Emergency Department (ED) presentations. 3 Data from the Australian Institute of Health and Welfare (AIHW) National Hospital Morbidity Database revealed that in 2017-2018, there were 7781 (31 per 100 000 population) admissions to a hospital with a principal diagnosis of gout. The hospitalisation rates were lower in 2008-2009 (20 per 100 000 population). 2 Gout admissions in the United Kingdom and New Zealand have also increased, which has also increased the burden on the healthcare system. Patients in New Zealand also had high rates of re-admisson for gout and suffered from comorbidities including diabetes mellitus (20-27%), hypertension (19-39%), renal disease (16-27%), heart failure (27.6%) and cardiovascular disease (39.1%). It has been established in literature previously that compliance with medications in gout is low and there is poor adherence to accepted guidelines, primarily through inadequate dosing of urate-lowering therapy (ULT) agents.5 -7 The American College of Rheumatology (ACR) recommends serum urate (SUA) targets of less than 0.36 µmol/L for non-tophaceous gout and less than 0.3 µmol/L for tophaceous gout.8,9 The British Society of Rheumatology (BSR) guidelines simply recommend titrating SUA to less than 0.3 µmol/L for all gout patients (regardless of the presence of tophi). 10
Our study aims to assess how many encounters to the ED were repeat presentations for acute gout during the study period and the utilisation of ULT in the community. Secondary outcomes analysed were the proportion of patients with a hospital record of aspirate-proven diagnosis of crystal arthropathy, the utilisation of pathology and imaging investigations, the number of joint aspirations performed, and the pharmacological management of acute gout.
Methods
We conducted a retrospective cohort study of patients who presented to the ED in the Illawarra Shoalhaven Health District, New South Wales. Inclusion criteria for this study were patients above the age of 18, discharged from the ED with an ICD (International Classification of Diseases) code of gout, crystal arthropathy, secondary gout, or drug-induced gout between January 1, 2015, and June 31, 2020. Exclusion criteria for this study were the absence of any documented notes, non-Australian residents, admitted as an inpatient for gout during that encounter, or if patients were discharged against medical advice. Ethics approval was obtained from the Low and Negligible Risk Ethics Committee at the Wollongong Hospital.
Clinical information was extracted from the electronic medical records at the hospital. Each encounter labelled with the aforementioned ICD codes was reviewed by the investigators to extract clinical information. Data extracted included age, sex, body mass index, smoking status, comorbidities, previous diagnosis of gout, previous ULT for gout, and whether they were known to a rheumatologist. Data were also collected on the diagnostic tests performed, including choice of imaging, joint aspirate, and blood tests. Finally, data were also collected on the pharmacological management of gout in the ED as well as whether patients were counselled on ULT. A gout flare or diagnosis of gout was confirmed based on the clinical interpretation stated on the discharge summary from the treating doctor. Statistical analysis involved descriptive statistics for baseline demographic variables.
From the initial review, there were 1111 individual encounters with the previously described ICD codes. Thirteen encounters were excluded from the study as three encounters were international citizens, one encounter was admitted to hospital, six encounters were incorrectly coded, two encounters did not have adequate documentation, and one encounter had discharged against medical advice.
Results
We collected data from 1098 separate ED encounters which included 912 individual patients. Baseline characteristics and comorbidities for the study population are available in Table 1. In our study cohort, 85.8% of the population was men and the mean age was 58.5 ± 16.5 years
Baseline characteristics and comorbidities of patients discharged from ED at ISLHD with crystal arthropathy.
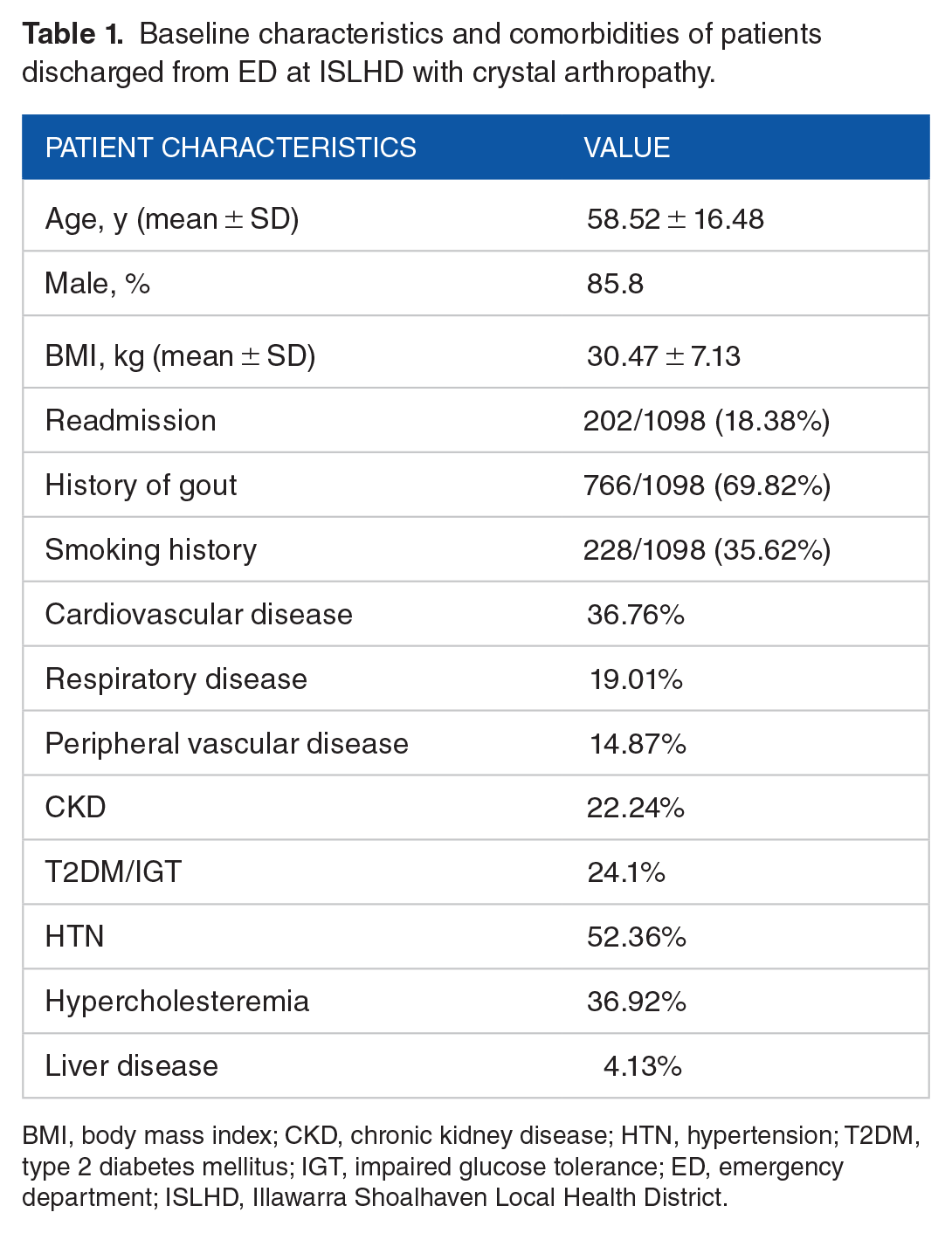
BMI, body mass index; CKD, chronic kidney disease; HTN, hypertension; T2DM, type 2 diabetes mellitus; IGT, impaired glucose tolerance; ED, emergency department; ISLHD, Illawarra Shoalhaven Local Health District.
From the clinical coding, the representation rate to ED for crystal arthropathy was 18.4%. In this cohort of patients, 69.8% of patients had a history of pre-existing gout, but only 30.8% had previously been prescribed ULT. Of those who had previously been prescribed ULT, 54.7% had documentation stating they were non-adherent to therapy. The mean dose of allopurinol and febuxostat was 209.5 ± 168.3 mg and 46.7 ± 39.3 mg, respectively.
Joint aspiration was performed in 9% of the patients in the ED during the same encounter, with the knee being the most frequently aspirated joint (Figure 1). Only 19% of patients had a joint aspirate at any point in time in the preceding ten years to confirm the presence of a crystal arthropathy. Most patients discharged had either a monoarticular presentation (82.7%) or an oligoarticular presentation (15.9%) as demonstrated in Figure 2. In addition, 5.6% of patients had documented tophi, and the average duration of time prior to presentation to ED was 3.9 ± 5.3 days. In 27.8% of encounters, an SUA level was performed, with hyperuricemia demonstrated in 30% of samples (average SUA of 0.45 µmol/L). Almost one in every two patients presenting to the ED had an imaging test performed, with 95.3% (430/451) undergoing a plain radiograph. From the imaging available for patients presenting to ED with acute gout, 6.2% (28/451) had evidence of erosive disease.

Aspirations performed in Emergency Department.

Characteristics of gout flares for patients presenting to the Emergency Department with gout.
Management
Acute management in the ED included prescribing analgesia (32.6% opiate-based medications) and medications for an acute gout flare (29% colchicine, 27.6% glucocorticoids, and 37.2% non-steroidal anti-inflammatory medications). In 80% of encounters, patients were discharged with a recommendation for further review with their general practitioner as an outpatient. Only 2% of patients were known to a rheumatologist from this cohort.
Discussion
Representation to ED
Approximately one in every five encounters in the ED was due to a representation of gout. Most patients with a history of gout were not actively on ULT, were not advised of the importance of commencing ULT and were discharged back to their General Practitioner BSR guidelines suggest that patient education and appropriate utilisation of ULT can reduce the risk of a gout flare in ED. This could be initiated through community care with general practitioners or through referral to a rheumatologist.
Acute and long-term management of gout
The European League Against Rheumatism (EULAR), ACR, and BSR guidelines recommend using allopurinol or febuxostat with a ‘treat-to-target’ approach using the SUA to deplete urate stores and therefore reduce the frequency of flares and formation of tophi (Figure 1). Day et al 11 developed a nomogram demonstrating the correlation between the pre-treatment SUA and the estimated required dose of allopurinol to reach the target SUA. Often, daily doses of allopurinol and febuxostat of more than 300 mg and 80 mg, respectively, are often required. 8 In our study, the mean dose of allopurinol and febuxostat was 209.5 ± 168.3 mg and 46.7 ± 39.3 mg, respectively
Despite these recommendations, our study demonstrated that 54.7% of patients with a previous diagnosis of gout were non-adherent with ULT. In addition, less than one in five patients with a diagnosis of gout had been prescribed ULT. Important reasons for discontinuation in therapy in the literature include lack of understanding of the role of ULT for both patients and clinicians, experiencing a flare of gout while on ULT, pill burden, side effects, and remembering to refill scripts.12,13 Experiencing a flare of gout during the first six months when first initiating ULT may incorrectly lead patients to feel they are intolerant to ULT or have failed treatment. Unfortunately, this is a common reason for poor adherence to treatment. 14 To minimise the risk of acute flares when initiating ULT, doses need to be slowly up-titrated until target SUA has been achieved. In addition, prophylaxis is required for six months (colchicine 0.5 mg twice daily or non-steroidal anti-inflammatory medications) after the SUA target is reached.15,16
The role of a joint aspiration in diagnosing gout
Current evidence-based guidelines, including the EULAR guidelines, recommend performing joint aspirations to identify MSU crystals and confirm a diagnosis of gout.9,17 Our study demonstrated that the primary management of gout in ED is inconsistent with these recommendations, as less than 1 in 10 (9%) had a joint aspirate performed. The most commonly aspirated joint in the ED was the knee (32%), followed by wrist (9%) and elbow (5.5%). Over the course of ten years in the same cohort of patients, 19% (122/1098) had proven urate crystals. It is important that an aspirate of the affected joint is performed to confirm the presence of urate crystals and exclude other pathology such as septic arthritis or inflammatory arthritis.
Conclusion
Our retrospective cohort study evaluated the representation rate for patients diagnosed with gout in the ED in the ISLHD. We observed that almost one in five encounters in the ED for crystal arthropathy were repeat presentations. In patients whom had a prior history of gout, 30.8% of patients had previously been prescribed ULT. However, 54.7% admitted to poor adherence to ULT. General practitioners have an essential role in providing ongoing care and management of gout and often may be the first to be able to initiate ULT and provide patient education. Refractory cases should be referred to a rheumatologist so that ULT can be titrated to the desired serum uric acid level. Patient education is critical in improving adherence to treatment and reducing the number of presentations and unnecessary investigations performed. Further education and strategies need to be implemented to improve patient outcomes and reduce the risk of complications associated with this treatable condition.
Footnotes
Author Contributions
AL - Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Writing – original draft, Writing – review and editing. AR - Data curation, Writing – review and editing. NB - Data curation, Writing – review and editing. JR - Supervision, Writing – review and editing.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
‘Data sharing is not applicable as no new data were generated or analysed during this study’. Data can be made available by contacting the corresponding author, and based on the request will be discussed with the ethics committee at the Wollongong Hospital.
Ethics Approval
Ethics approval was obtained from the Low and Negligible Risk Ethics Committee at the Wollongong Hospital.