
Abstract
Since its initial description in the late 19th century, sarcoidosis has been extensively studied. Although the general mechanism of immune activation is known, many details especially in the context of disease associations are still missing. One of such associations is the musculoskeletal complications that are widely variable in terms of presentation and response to treatment. Sarcoidosis can involve the joints leading to acute and, less commonly chronic, arthritis. While acute arthritis is mostly self-resolving in nature, chronic arthritis may lead to deformity and destruction of the joint. Sarcoidosis can also involve the muscles, leading to different pathologies primarily categorized according to the clinical presentation, despite the efforts to find a new classification based on imaging, histological, and clinical findings. The bones can be directly and indirectly affected. Different types of bone lesions have been described, although around half of these patients remain asymptomatic. Osteoporosis, increased risk of fractures, hypercalcemia, and hypercalciuria are examples of the indirect effect of sarcoidosis on the bones, possibly contributed to elevated levels of calcitriol. Nevertheless, sarcoidosis can be associated with small-vessel, medium-vessel, and large vessel vasculitis, although it is frequently difficult to differentiate between the co-existence of a pure vasculitis and sarcoidosis and sarcoid vasculitis.
Background
Sarcoidosis, first described in 1878, 1 is a multisystem granulomatous disorder characterized by the accumulation of CD4 lymphocytes and activated macrophages in affected organs, resulting in the formation of granulomas. 2 The lungs and the bilateral hilar lymph nodes are primarily affected, but the disease can affect other organs, such as the skin, joints, and eyes. 3 Sarcoidosis mainly affects young people, especially in the third and fourth decades of life, but children and elderly subjects may also be affected. 4 Because many cases remain asymptomatic, it is difficult to determine the real incidence and prevalence. 3 However, the prevalence is estimated at about 4.7 to 64 in 100 000, and the incidence is estimated at about 1.0 to 35.5 in 100 000 per year.5,6
Although the clear etiology of sarcoidosis is still unknown, specific antigenic stimuli processed by activated macrophages induce an altered immune response modulated by T cells and macrophages. 7 This altered response is caused by the upregulated expression and function of MHC-2 molecules and costimulatory molecules such as CD86, CD80, and intercellular adhesion molecule (ICAM). 8 The production of CXCR3 chemokines, such as CXCL10, allows the influx of CXCR3-positive T-helper 1 (Th1) cells into affected organs, 8 which are capable of producing interferon-γ, tumor necrosis factor-α (TNF-α), and interleukin 2. 8
When the antigen persists, the chronic immune response generated results in a progressive disease. 9 Consequently, epithelioid-cell-rich non-necrotizing granulomas trap remnants of causative agents. These epithelioid granulomas are derived from activated macrophages being surrounded by T-helper-inducer CD4+ lymphocytes and rare B cells. 9 Rarely, Langerhans cells with Schaumann and asteroid bodies can be found inside the granuloma. 9
Because of the activation of several immune cells and the release of chemokines, joint, bone, muscle, and vessel involvement is possible. As such, this article will review some reported musculoskeletal manifestations and complications of sarcoidosis along with pathophysiological links and treatment modalities.
Articular Involvement
As part of the nonspecific systemic symptoms of sarcoidosis, arthralgias can occur. Sarcoid arthritis is usually categorized into acute, which is the more common form, and chronic. 10
Acute arthritis
Acute arthritis may be self-limited oligoarthritis of the large joints resembling reactive arthritis 11 or occurs as part of the triad of Löfgren syndrome (LS) (Figure 1): symmetric hilar adenopathy, joint pain, and erythema nodosum. 12 It usually occurs in up to 40% of patients with sarcoidosis and can be the initial presentation of the disease. 13

A 45-year-old man with Löfgren syndrome (acute erythema nodosum, arthropathy, and bilateral hilar lymphadenopathy).
In most patients with LS, bilateral ankle involvement is noted. 14 Sarcoid monoarthritis is typically rare, except when occurring in the setting of gout and septic arthritis. 15
The presence of HLA-DRB1 and HLA-DRB1*03 alleles has been linked to better prognosis for patients with LS. 16 Bilateral hilar adenopathy is detected by chest radiographs in 90% of patients. 14 On the contrary, erythema nodosum only occurs in around 40% of patients and has been reported more commonly in Caucasians and women. 17 In most cases, LS self-resolves within few months. 17 Very rarely, relapse and joint destruction occur. 18
In sarcoid arthropathy, compared with LS, noncaseating granulomas are usually detected in synovial biopsy. 19
Imaging by ultrasound usually reveals joint swelling attributable to periarticular soft tissue swelling and tenosynovitis. 20 True joint synovitis or effusions can be rarely detected on Doppler. 20 Although not required for diagnosis, synovial fluid analysis might reveal mild inflammatory infiltrate with a predominance of mononuclear cells. 21 A histopathological examination may not demonstrate a granulomatous reaction. 21
As LS is a self-limiting process, nonsteroidal anti-inflammatory drugs are sufficient in most cases. 22 Nevertheless, 10 to 20 mg of prednisolone is also usually sufficient. 22 Most patients go into remission within a maximum of 6 months. 18
For granulomatous sarcoid arthropathy, local corticosteroid injection and hydroxychloroquine have demonstrated efficacy secondary to their immunomodulatory properties. 23
Chronic arthritis
Chronic arthritis usually occurs as part of multiple manifestations, including parenchymal lung involvement, lupus pernio, chronic uveitis, and tenosynovitis. 24 It mostly presents as persistent oligoarthritis or polyarthritis, along with occasional dactylitis. 14 In advanced cases, erosive changes or Jaccoud-type arthropathy (no joint destruction) may occur. 25 Chronic arthritis is relatively rare affecting around 0.2% of cases, at least 6 months after the disease onset. 26
The differential diagnosis of chronic sarcoid arthritis includes reactive arthritis and rheumatoid arthritis. Elevated rheumatoid factor and citrullinated peptide antibodies hint toward rheumatoid arthritis. In addition, synovial fluid analysis has a milder inflammatory component in sarcoid arthritis than rheumatoid arthritis or infectious arthritis, although sometimes a synovial biopsy might be needed to distinguish rheumatoid arthritis from sarcoid arthritis. 21
Imaging is not very specific for chronic arthropathy of sarcoidosis. For example, radiography might infrequently show signs of demineralization associated with soft tissue infiltration. 27 However, destructive arthropathies might lead to narrowing of the joint space and demineralization of the subchondral bone. 27 Similarly, magnetic resonance imaging (MRI) findings might depict those of tenosynovitis, such as the involvement of the extensor tendons of the fingers. 28
While synovial fluid analysis shows mononuclear and polymorphonuclear cells, synovial biopsy shows noncaseating granulomas. 26
Chronic arthritis has a poorer prognosis than acute arthritis. 24 Despite that the management is poorly studied, multiple pharmacological therapies have been tried (Table 1). Methotrexate has been found beneficial in few case-series.29,30 The TNF antagonists have not been efficacious on the long-term. 31 Other options include azathioprine, local corticosteroid injection, and hydroxychloroquine. 32
Literature review of the types and outcomes of pharmacological interventions used for treatment of chronic arthritis secondary to sarcoidosis.
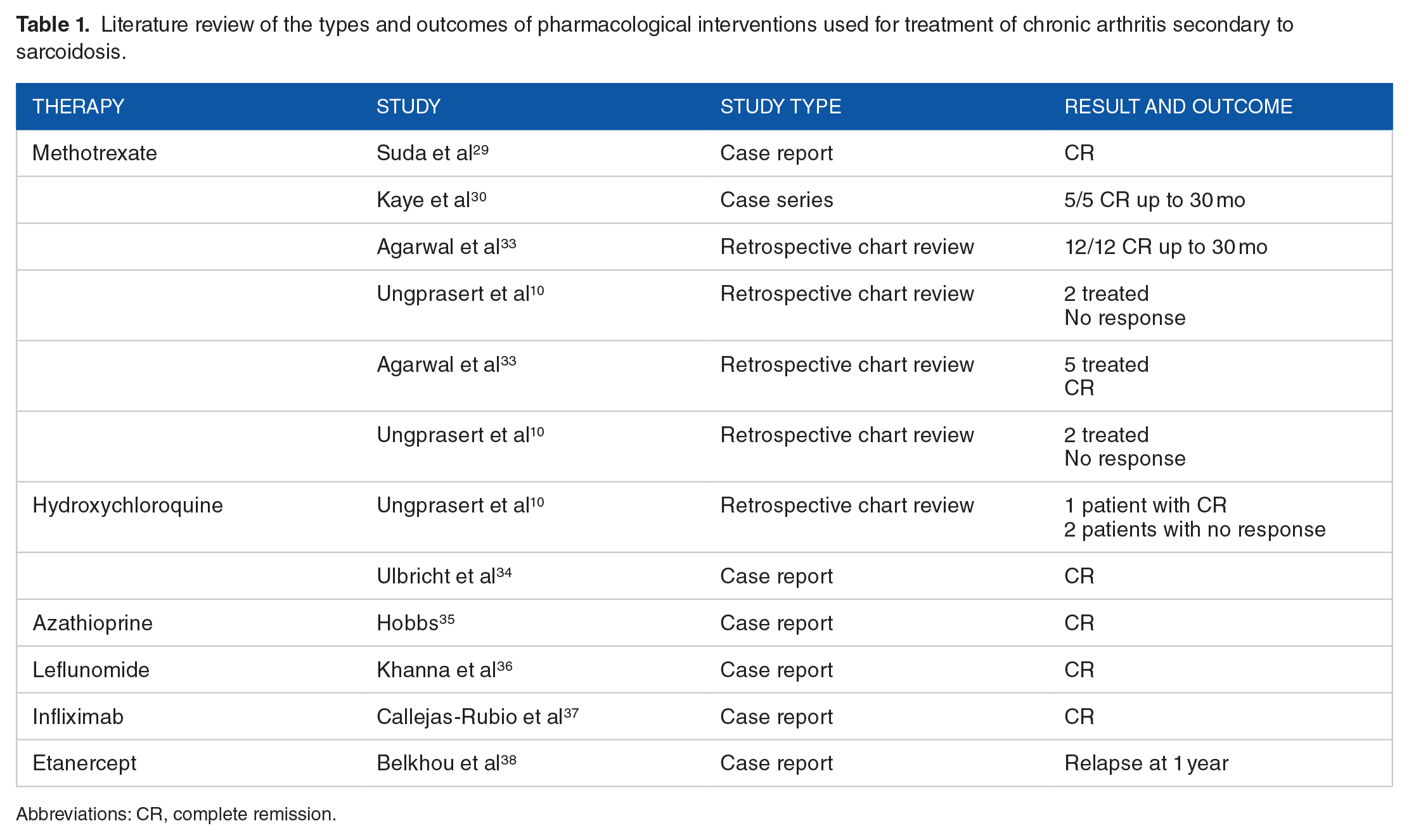
Abbreviations: CR, complete remission.
Muscular Involvement
The first published case of sarcoidosis of the skeletal muscles goes back to 1908. 39 Muscle involvement occurs in up to 80% of patients with sarcoidosis, although the involvement stays asymptomatic in most cases. 40 A muscle biopsy is helpful for diagnosis as it reveals noncaseating granuloma. 40 Classically, sarcoid muscular involvement has been classified into 4 main classifications: asymptomatic, nodular, acute myositis, and chronic (Table 2). 41 However, with a newly suggested classification based on clinical manifestations, electromyography (EMG), MRI, and pathology, muscle involvement in sarcoidosis suggests 4 patterns: nodular, smoldering, myopathic, and combined myopathic and neurogenic pattern. 42 Notably, more than 1 type can coexist in the same patient. 43
A summary of the symptomatic sarcoid muscular involvement.
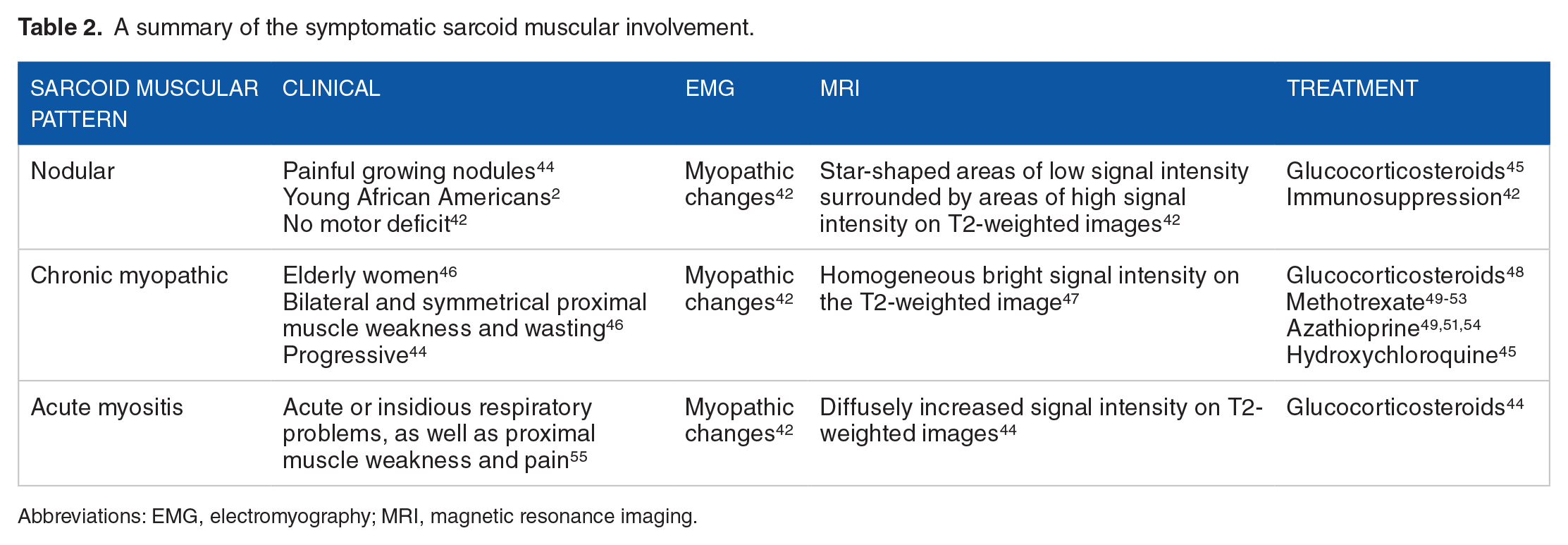
Abbreviations: EMG, electromyography; MRI, magnetic resonance imaging.
The nodular type
Nodular sarcoid myopathy presents as painful growing palpable nodules in the extremity muscles along with myalgia but without motor deficit. 42 Although not well studied, the nodular form has specific MRI and EMG findings (Table 2). As the course of the nodular type is relapsing-remitting, immunosuppression is commonly used for treatment. 42 The nodular type is the second least common type of sarcoid muscular involvement. 56
Chronic myopathic type
Chronic myopathy is the most common type of presentation of sarcoid muscular involvement. 46 As it presents with symmetrical weakness and atrophy of the proximal muscle groups,46,49 it can mimic muscular dystrophy. Muscle enzyme activity is usually insensitive. Gallium-67 (67Ga) scintigraphy can be helpful in identifying muscular involvement. 57 Patients with chronic sarcoid myopathy generally respond well to glucocorticosteroids. 57
Acute myositic type
This type of sarcoid muscular involvement is the rarest. 44 Usually, it presents with muscular swelling and pain. 58 Because nonspecific findings are noted on imaging, 59 laboratory and histopathological work-up is needed for diagnosis. Glucocorticosteroids are the mainstay of treatment. 58
Smoldering type
A newly described smoldering pattern of sarcoid muscular involvement refers to constant myalgia without nodules, motor deficits, or myotrophy. 42 The smoldering pattern less frequently affects African Americans and the MRI is usually normal. 42 Around 70% of patients with smoldering muscular sarcoid respond to glucocorticosteroids with no subsequent relapse. 42 Hydroxychloroquine is sometimes useful. 42
Osseous Involvement
The first case of sarcoid bone involvement goes back to 1903. 60 Bone involvement has been reported in 3% to 13% of patients with sarcoidosis.61,62 Around half of the patients with bone involvement stay asymptomatic. 63 Although peripheral involvement is most commonly reported, 15 recent radiological data are reporting more frequent axial involvement. 61
Bone lesions
Sarcoid bone lesions are usually divided into permeative or “moth-eaten” appearance, lytic lesions or bone cysts, and sclerotic lesions. 64 The “moth-eaten” pattern involves the cortex of the phalanges and is accompanied by soft tissue swelling. 62 Lytic lesions usually involve the cortex and medulla, most frequently of the middle and proximal phalanges 64 (Figure 2). Sclerotic lesions are seen in the spine and must be differentiated from metastatic lesions. 61 Although the exact etiology of these lesions has not yet been elucidated, certain factors could play a role65 -67 (Figure 3).

Radiograph of the bilateral hands in a 32-year-old man with mild pulmonary sarcoidosis.

In case the bone lesion occurs in the absence of typical pulmonary and extrapulmonary features of sarcoidosis, a bone biopsy is needed to demonstrate the presence of noncaseating granuloma. 64
Bone metabolism
Several factors could contribute to a low bone mass in patients with sarcoidosis. Diffuse skeletal granulomatosis and frequent use of glucocorticosteroids are principal contributing factors. 68 Besides, the overproduction of calcitriol (1,25(OH)2 D3) by the granulomas can decrease bone mineralization and promote fragility. 68 Therefore, clinicians should be cautious with supplementation with calcium and vitamin D. 69 The risk of fragility fractures among patients with sarcoidosis is increased in the distal forearm, being independent of glucocorticosteroid use. 70 Notably, there is no significant increase in fracture risk in vertebrae, proximal femora, and humerus. 70
Hypercalcemia and hypercalciuria
Hypercalcemia may be seen in up to 18% of patients with sarcoidosis, whereas hypercalciuria might be observed in around half of patients. 71 The increased production of calcitriol is the primary contributing factor for hypercalcemia. As calcitriol is produced by macrophages that have no alternative metabolic pathway activated under conditions of hypercalcemia, it is possible that hypercalcemia in patients with sarcoidosis is associated with a normal plasma level of calcitriol. 68 The administration of vitamin D2 is associated with a slight increase in serum level of both 25(OH)D3 and 1,25(OH)2D3, in contrast to healthy individuals who will have an enhanced level of 25(OH)D3. 72 Rarely, parathyroid hormone–related protein (PTHrP), produced by macrophages and giant cells, might contribute to hypercalcemia. 73 Importantly, urinary calcium output is associated with serum chitotriosidase activity, an important biomarker of the disease activity. 74
Sarcoid Vasculitis
Rarely, sarcoidosis may be complicated by systemic vasculitis that can affect small, medium, or large arteries, with granulomatous lesions seen on vessel biopsy. Necrotizing sarcoid granulomatosis (NSG) is characterized by sarcoid-like granuloma, vasculitis, and variable degrees of necrosis, in the absence of other contributing factors 75 (Figure 4).

Granulomas are surrounded by lymphocytes and plasma cells; irregular areas of necrosis are seen admixed with granulomas, but necrosis seems to be unassociated with granulomas.
Small-vessel vasculitis
Small-vessel sarcoid involvement usually affects the white population. 76 Leukocytoclastic vasculitis (LCV), a type of small-vessel vasculitis, might coexist with sarcoidosis.77 -81 Most of the reported cases of LCV-associated sarcoidosis are limited to cutaneous involvement, in particular petechiae, purpuric spots, and infiltrative erythema. Necrosis is limited in LCV, in comparison with NSG. 82 Glucocorticoids, with or without cyclophosphamide, are usually beneficial for treatment. 83
Medium-vessel vasculitis
Medium-sized vessels, along with pulmonary lymphatic capillaries, are usually associated with the pulmonary form of sarcoidosis. 84 In contrast to small-vessel involvement, medium-vessel sarcoid vasculitis presents with systemic symptoms that can include fever, arthritis, and cutaneous manifestations. 83 An example of medium/small-vessel vasculitis is granulomatosis with polyangiitis (GPA), which may be difficult to be differentiated from lung-necrotizing sarcoid granulomatosis, a variant of sarcoidosis with angiitis being a prominent feature. 85 For example, an isolated pulmonary involvement of GPA might be misdiagnosed as sarcoidosis. 86 In addition, granulomatous angiitis and/or microangiopathy can be present in up to 31% of sarcoid skin lesions. 83 Anti-neutrophil cytoplasmic antibody is usually negative in sarcoid vasculitis (NSG), and renal involvement is less common than in GPA. 87 Similarly, patients with sarcoid vasculitis have no upper airway disease, nephritis, or systemic vasculitis, which is the case in GPA. 88
Large-vessel vasculitis
Large-vessel vasculitis, namely Takayasu arteritis (TAK) and giant cell arteritis (GCA), can be very rarely induced by sarcoidosis and can also be very rarely associated with sarcoidosis. Therefore, it is important to differentiate between the coexistence of large-vessel vasculitis and sarcoidosis and the entity of sarcoid-induced vasculitis. For example, TAK can contribute to a granulomatous inflammation, which does not represent a true sarcoidosis. The association of TAK and sarcoidosis has been described in around 25 cases so far. 89 The prognosis has been good in most cases, with gucocorticoids being the mainstay of treatment. 89 Similarly, it is difficult to distinguish between large-vessel vasculitis and GCA. Age and vascular distribution can help in distinction. An age of disease onset above 50 with cranial symptoms secondary to involvement of extracranial branches of the carotid artery favors GCA. 90 An age less than 40 with symmetric bilateral hilar lymphadenopathy suggests sarcoidosis. 90 However, both conditions could coexist.
Conclusion
Sarcoidosis is a multisystem disease that can involve the musculoskeletal system, in particular the joints, muscles, bones, and vessels. In rare cases, musculoskeletal involvement can be the presenting clinical feature of sarcoidosis. Acute sarcoid arthritis is usually self-resolving, in contrast to chronic arthritis which has a higher risk of joint destruction. Both acute and chronic sarcoid arthropathies are associated with systemic manifestations. Acute arthritis can present in the picture of LS, whereas chronic arthritis is associated with multiple organ involvement. Symptomatic sarcoid muscular involvement has been classically divided into nodular, acute myositis, and chronic myopathic, although asymptomatic involvement is the most common. Although imaging can be helpful to determine the nodular and chronic myopathic type, the acute myositic type has nonsensitive findings. Glucocorticoids have been found to be beneficial in the treatment of the 3 types. Similar to muscular involvement, the osseous involvement of sarcoidosis remains asymptomatic in around half of the patients. Sarcoid bone lesions can be permeative, lytic, and sclerotic mostly depending on the location of the bones involved. As a result of the disease process and activation of osteoclasts, the bone density can decrease increasing the risk of fracture, in particular in the distal forearm. In addition, hypercalciuria may be present in up to half of the patients, but hypercalcemia in only around 18%. The vascular involvement of sarcoidosis is still infrequently studied. Although vasculitis can coexist and sometimes be induced by sarcoidosis, the pathophysiology and the clinical approach still need to be better deciphered.
Footnotes
Author Contributions
Each individual named as an author meets the journal’s criteria for authorship. Dr. GEH has substantial contributions to drafting the article and revising it critically for important intellectual content. Dr. IU has substantial contributions to analysis and interpretation of data as well as drafting the article and revising it critically for important intellectual content. Dr. ASJ has substantial contributions to article conception and design, substantial contributions to analysis and interpretation of data, and final approval of the version of the article to be published.
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.