
Abstract
Dropped head syndrome (DHS) is manifested as the inability to maintain the head in an upright posture. It has been associated with a wide spectrum of myopathies and neurological conditions. Isolated neck extensor myopathy (INEM) is one of many potential causes of DHS. This is a case report of a 72-year-old man who presented with degenerative cervical spondylosis and DHS for 2 years. He had previously failed to achieve a positive outcome to medication, cervical collar and exercise rehabilitation. However, he was able to regain his voluntary head control after a 4-month chiropractic program. It is believed that INEM is caused by isolated myopathic changes from chronic injury and overloading of the cervical muscles. Cervical spondylosis has been attributed as the cause of DHS secondary to denervation of the cervical extensors. While INEM associated with degenerative spondylosis is not medically treatable, manipulative therapies may be adopted before considering surgical intervention.
Keywords
Introduction
Dropped head syndrome (DHS) is a rare condition resulting from weakness of the cervical paraspinal muscles (neck extensors) causing an inability to hold the head in an upright position. 1 In contrast to other structural disorders, the dropped head is a functional deformity. In general, the head is able to be passively ranged or moved up by hands and the neck deformity resolves when lying supine.2,3 DHS can occur in isolation or in association with a variety of causal factors, including neurological, neuromuscular, muscular, metabolic and dystrophic causes. Isolated neck extensor myopathy (INEM) is a term coined to describe a specific type of head drop caused by non-inflammatory myopathy restricted to the cervical paraspinal muscles. 4 INEM associated with cervical spondylosis is scarcely reported. Cervical spondylosis is believed to cause neural and micro-circulatory compromise, leading to weakness of neck extensors. INEM is diagnosed when all the neuro-physiological tests reveal only myopathic changes of the neck extensors are present.
Case Report
A 72-year-old Chinese man with chronic nuchal pain complained of progressive difficulty in lifting the head over the last 2 years. He also developed difficulty walking due to the loss of horizontal gaze. Past history was notable for hypertension under control. The patient reported no history of trauma and no known neurological deficits. Prior workup by an orthopedic surgeon and a neurologist excluded the diagnosis of any cranial, neurological or autoimmune diseases. A muscle biopsy from the left trapezius muscle demonstrated nonspecific myopathic features. Cervical collar, oral non-steroidal anti-inflammatory medication and exercise rehabilitation were ineffective in correcting his posture for the past 1 year. The patient then sought chiropractic care for his condition.
Upon examination, the patient ambulated with a cane to maintain balance. Gaze was down at the floor, instead of forward. Pronounced head drop with neck flexion caused the chin to rest on the chest in standing or sitting. The center of gravity plumb line (COG PL, red dashed line) is considered a virtual gravity line of the entire body (Figure 1A). Measurements of cervical range of motion (ROM) showed restriction of active motions, where active versus passive extension ROM (normal range: 70°) was 10°/54°, and active versus passive rotation ROM (normal range: 90° to both sides) was 58°/72° each side. The head was able to be passively raised up by hands and the neck deformity resolved when lying supine. Pain intensity of the neck was rated 3-4/10 on an 11-point numeric pain rating scale, where 0 means no pain and 10 means the worst imaginable pain. Motor strength measurement of the cervical extensors with a handheld dynamometer was graded at 4+/5. The patient could maintain the head up with extreme effort only for a couple of minutes. EOS® radiographies (Figures 2A and 3A) revealed reverse lordosis 5 (CobbC2-C7 −16°), cervical disc space narrowing with grade 1 anterolisthesis at C3/4 and C4/5 levels (red arrows), and C5-C6 ankylosis (hollow arrow). COG-C7 sagittal vertical axis (SVACOG-C7) ⩾30 mm (red solid line) is regarded as occiput-trunk discordance 6 and SVAC2-C7 ⩾40 mm (purple solid line) is considered to be cervical sagittal imbalance. 7 Needle electromyography revealed myopathic changes in the cervical muscles. Clinical pictures and histological findings were consistent with INEM associated with cervical spondylosis.

Changes in the posture of the patient with dropped head syndrome: (A) before treatment, the patient was obliged to face downward, stretching the neck and showing a chin-on-chest deformity and (B) the patient regained horizontal gaze and compensatory sagittal balance after 4 months of chiropractic care. The center of gravity plumb line (dashed line) is considered the virtual gravity line of the entire body.

Sagittal EOS® radiographs of the cervical spine: (A) an initial radiograph before treatment revealed reverse lordosis (CobbC2-C7 −16°), interspace narrowing with grade 1 anterolisthesis at C3/4 and C4/5 levels (blue arrows), C5-C6 ankylosis (hollow arrow), and cervical sagittal imbalance (SVAC2-C7 62 mm) and (B) at 6-month follow-up, the repeat radiograph depicted partial improving cervical curvature and cervical parameters after treatment. SVACOG-C7 offset (red solid line, normal ⩽30 mm) reduced from 96 mm down to 74 mm and SVAC2-C7 (purple solid line, normal ⩽40 mm) from 62 mm to 49 mm.
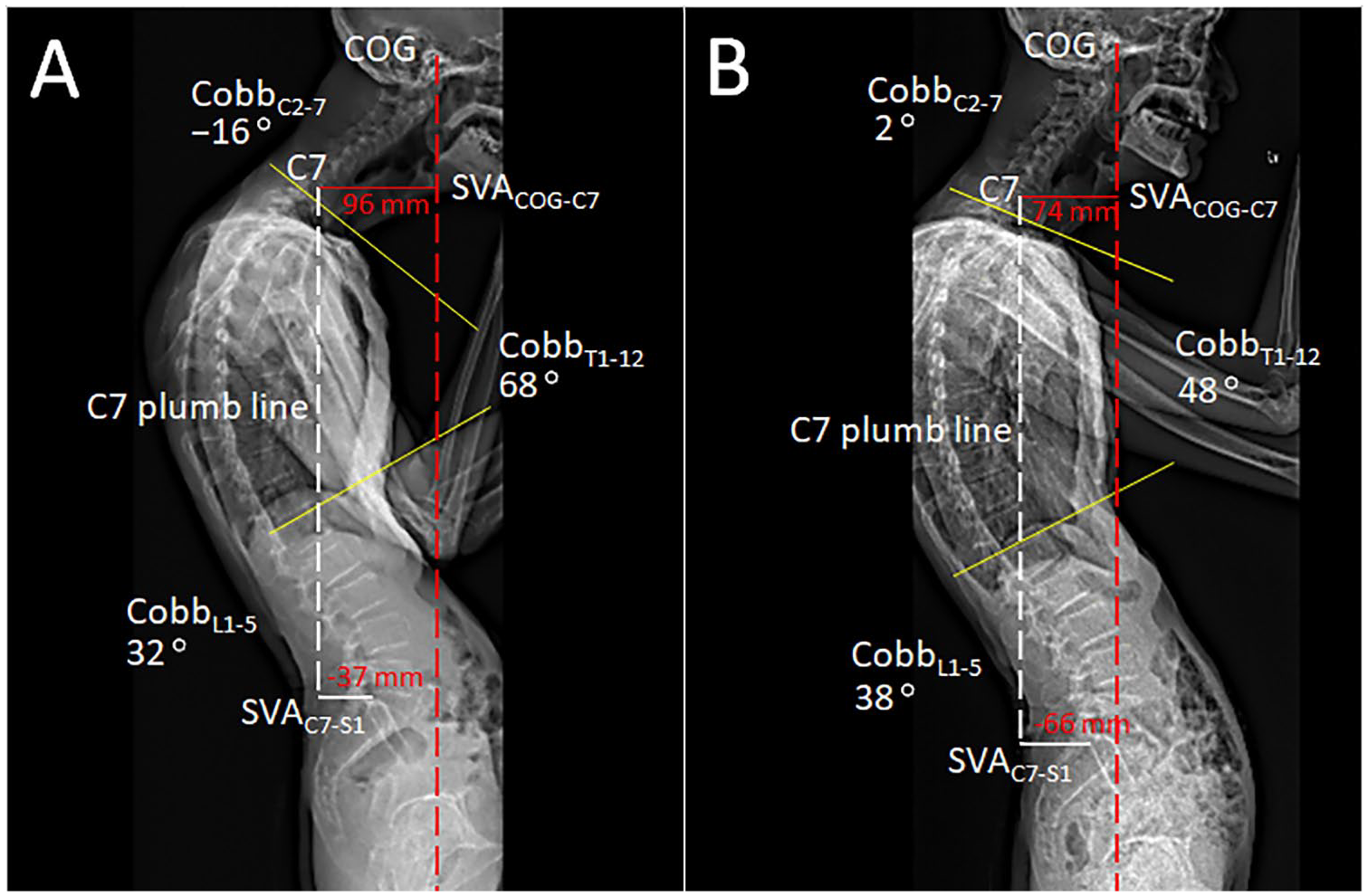
Postural parameters measured on sagittal standing full-spine EOS®: (A) before treatment, a CobbC2-C7 angle <0° was defined as reverse lordosis. Normal range: cervical lordosis 20° to 40°, thoracic kyphosis 20° to 50°, and lumbar lordosis 60°. SVACOG-C7 (red solid line, normal ⩽30 mm) was 96 mm, indicating occiput-trunk discordance and (B) at 6-month follow-up, most of the radiographic parameters were improved, except SVAC7-S1 offset (white solid line, normal ⩽30 mm). SVAC7-S1 moved posteriorly (from −37 to −66 mm), indicating negative sagittal balance.
The chiropractic regimen consisted of upper thoracic spine manipulation, electrical muscle stimulation (EMS), cervical extension exercises and cervical collar. The splenius capitis, semispinalis capitis, semispinalis cervicis, and trapezius are the key muscles for cervical extension. In order to correct dropped head posture and relieve neck pain, these muscles need to be strengthened specifically. In the presence of instability at C3/4 and C4/5 levels, cervical manipulation was contraindicated. An upper thoracic manipulation was cautiously delivered instead. An inflatable air pump cervical collar was prescribed to maintain neck posture and to relieve neural compression when patient was at home. Greater functional range of active cervical motion was obtained after 2 weeks of treatment 5 times per week. Subsequently, in addition to manipulative therapy, EMS of the neck extensors and cervical extension exercises for muscle strengthening were added in each treatment session. Treatments were delivered 3 times weekly for further 3 months. Dropped head state was almost corrected and neck pain was fully resolved near the completion of treatment. The patient resumed normal daily activities and continued monthly follow-ups. At the 6-month follow-up, he regained upright posture of the head and global sagittal balance (Figure 1B). Repeat standing full-spine EOS® (Figures 2B and 3B) depicted substantial improving of most of the radiographic parameters except SVAC7-S1. The C7 plumb line (white dashed line) should fall within 30 mm, either anterior or posterior, to the posterosuperior endplate of the S1. 8 His SVAC7-S1 moved posteriorly (from −37 to −66 mm), indicating negative sagittal balance. 9
Discussion
Dropped head syndrome (DHS) is a functional deformity associated with a broad spectrum of neurological, neuromuscular, muscular, metabolic, and dystrophic diseases.1,2 Suarez and Kelly Jr described an isolated type of DHS caused by non-inflammatory myopathy, affecting predominantly the cervical paraspinal muscles in older individuals. 10 Subsequently, the term “isolated neck extensor myopathy” (INEM) was coined by Katz et al. 4 In the current study, the patient manifested classical characteristics of INEM described by Katz et al. The histologic features of trapezius biopsy provided additional evidence of a non-inflammatory myopathic process.
The etiology of DHS and INEM remains unclear and is likely multifactorial. In the older people with cervical spondylosis, some pathophysiology changes may lead to INEM. Firstly, it is hypothesized that, advancing age, kyphotic postural changes, laxity of neck soft tissues, and low physical performance may cause excessive load on the neck and induce isolated myopathy of neck extensors. 4 Secondly, age-related sarcopenia 11 and gradual weakening of neck muscles, the posterior tension-band will be over-loaded, which can lead to widening and increased mobility of the facet joints and result in cervical nerve root avulsion. 12 Given that cervical paraspinal musculature is supplied by the dorsal rami of cervical nerves from C3 downwards, denervation and progressive weakness of the paraspinal musculature likely occurs following nerve root avulsion. 12 Thirdly, spondylotic changes may cause spinal stenosis, microcirculatory disturbance and ischemic dysfunction of the anterior horn cells of the cord, 13 leading to atrophy of the affected muscles and a dropped head state. Further, certain individuals with compromised conditions are incapable to recover from injury and may manifest as myopathy. This scenario may result in aggravated spondylosis, myonecrosis, cervical myelopathy or neurological deficits.3,14
Development of INEM years after suffering from cervical spondylosis is a probable scenario but scarcely reported. 3 It has been observed that patients with cervical spondylosis complicated by INEM may require early surgical management before neurological symptoms appear. Delay in diagnosis and management of the radiculopathic and myelopathic changes may lead to poor prognosis. 3 Cases received conservative treatments had unfavorable outcomes for patient with progression of disease toward cervical spondylotic myelopathy, but surgeries,15-17 for example, spinal fusion or instrumentation, could provide cervicothoracic stabilization.
Mechanical neck pain is caused by an agitated nociceptive discharge of the afferent fibers in the vertebral facet joints, intervertebral discs, and paraspinal muscles. 18 It is possible that high velocity, low amplitude spinal adjustment of the upper thoracic segment, performed in the current case, unloaded some structures and relieved the associated soft tissues and neural compromise, allowing the compressed joints and affected muscles to restore their function. 19 Pain relief following chiropractic manipulation improved proprioception of cervical paraspinal muscles. 18 Subsequent neck exercises improved muscle endurance and strength to keep the head upright. In cases of INEM secondary to biomechanical factors, manipulative therapies may be an alternative therapy before considering surgery. Further researches to better clarify the role of chiropractic are necessary.
Conclusion
Presented is a case of cervical spondylosis coexisting with INEM. INEM is believed to be cause by isolated myopathic changes from injury and denervation of the cervical extensors. Cervical spondylosis and age-related sarcopenia may increase workloads on the neck that lead the cervical paraspinal musculature vulnerable to injury. Compromises physical health further plays a role in elderly individuals being more susceptible to muscular decompensation.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Authors’ Contribution
EC-PC contributed the case information and drafted the manuscript. AF-CL edited the article. The article took form under AY-LW’s guidance. All the authors have read and approved the final manuscript.
Informed Consent
Written informed consent was obtained from the patient for publication of this manuscript and any accompanying images.