
Abstract
Objective:
The aim of the work was to demonstrate the effectiveness and safety of ultrasonographic guided aspiration performed with corticosteroid injection intra-lesional for ruptured Baker cysts (BCs).
Methods:
Single-center retrospective study that included 42 patients with knee joint disorder associated with ruptured BCs were treated by ultrasonographic guided aspiration of fluid from the cyst and different points from the calf then intra-lesional injection of corticosteroids once or twice, 1 week apart. Follow up were done weekly until complete resolution of symptoms. Visual analog scale (VAS) and Rauschning-Lindgren and Lysholm Knee Scoring Scales (RLC) were used for assessment.
Results:
Clinical parameters (VAS and RLC) improved significantly in all patients at both post injection evaluation visits (1 week and 12 weeks). Ultrasonographic features improved significantly with complete disappearance of free fluid in the calf in 35 (83.3%) cases 1 week after the injection, and in 41 (97.6%) after 12 weeks. As regards BCs only 4 (9.5%) cases showed complete disappearance after 1 week and there was recurrent BCs in 38 (90.5%) cases which required reaspiration. While after 12 weeks, BCs were completely disappeared in 23 (54.8%) cases, most of the relapsed BCs were complex BCs. No side effects were reported in all cases.
Conclusion:
Ultrasonographic guided aspiration followed by injection of corticosteroids intra-lesional is an efficient and safe method for managing ruptured BCs.
Introduction
Baker’s cyst (BC) is the popliteal fossa’s most prevalent mass; the incidence in the general population has been reported to be between 10% and 41% and is the result of gastrocnemio-semimembranosus bursa fluid distension. Mostly asymptomatic, the patients may complain of the presence of a mass or growth in the knee’s posterior region.1-4 The incidence of BC is between 5% and 38% and increments with aging. Various rheumatological diseases associated with BCs include osteoarthritis (OA), rheumatoid arthritis (RA), spondyloarthropathies (SpA) and Behçet disease. 5
BC is most often complicated by rupture and/or dissection of fluid in the nearby muscle belly of the proximal gastrocnemius, which results in a pseudothrombophlebitis syndrome that mimic the symptoms of deep vein thrombosis (DVT) causing calf pain and swelling.4-7 Musculoskeletal Ultrasound (MUS) may be used easily and accurately in patients suffering from painful swollen legs to distinguish ruptured BC from other diseases for accurate diagnosis before evaluation for DVT to avoid unnecessary anticoagulant medications. 8 Ruptured BC treatment ranged from conservative management to operative resection.
Ultrasonographic directed aspiration and injection of corticosteroids may be an effective and easy method for managing such instances.9,10 Up to the best of our knowledge, this is the first study to detect the efficacy and safety of MUS guided aspiration of ruptured BCs and different points from the calf then intra-lesional injection of corticosteroids.
Methods
Patients
A retrospective single-center study was performed in 42 patients with knee joint disorder associated with ruptured BCs (12 males and 30 females, mean age 36 ± 10 SD years old) were included in the period between January 2013 to January 2019. The diagnosis was done by clinical presentation of calf muscles tenderness, swelling and ultrasonographic evidences of ruptured BCs as a free fluid accumulation in the calf linked to a well-defined cyst at the back of knee. The cases were either referred or primary diagnosed in the department of rheumatology, physical medicine and rehabilitation, Zagazig University hospitals from January 2013 to January 2019. Consent was obtained for each patient before the procedure.
Imaging and intervention
All patients were examined by B-Mode (gray-scale) real-time musculoskeletal ultrasound was performed by a rheumatologist experienced in musculoskeletal ultrasonography, using either:
Hitachi-Aloka F37, Japan interfaced with a 10-18 MHz linear array transducer (2018)
Sonoscape S6, 7-15 MHz Linear array transducer (2016)
Medison, R3, 5-12 MHz Linear array transducer was used (2011). The frequency of gray scale ultrasonography used during ultrasonographic examination, aspiration and injections was ranged from using 7- to 12-MHz.When needed Power Doppler US was used to differentiate BC from blood vessels.
The diagnosis was initially made by the existence of BC ultrasonographic characteristics (a well-defined cyst linked to the knee joint which has distinct components of a typical popliteal cyst: base, neck, and body). The indicator of rupture was the pointed configuration of the distal edge and fluid extension to the lower calf with subcutaneous space swelling. BCs were classified as complex (characterized by the presence of one or more of the following: Echogenic bodies, Internal synovitis, septation, and synovial thickening) or simple (characterized with a thin synoival wall and well-defined smooth borders).
Under complete aseptic conditions and under the guidance of ultrasonography with patient lying prone, BC was punctured by a 18 G Seldinger needle, the intraluminal content was diluted by injection of 1% lidocaine to facilitate complete evacuation. 1 If the complex BC with septations, the cyst was penetrated and aspirated from several different points until BC almost completely decompressed. Also, Aspiration of different points from the calf was done, and then 40 mg triamcinolone acetonide was injected intra-lesionally into the BC once or twice with one week apart according to the patient response as shown in Figures 1-3. The patients were advised to wear compression bandage after the procedure for one week to promote adhesion of the evacuated cyst walls.

Seven serial longitudinal view photos of ruptured Baker cyst (A1-A7) at back of knee and extending up to the middle of the calf in a patient with knee osteoarthritis, (B) aspiration of ruptured Baker cyst arrows refer to the needle inside the caudal area of the ruptured cyst at the calf, (C) 1 week after aspiration and local injection of ruptured Baker cyst. Persistence of the complex cyst and disappearance of the extended part at the calf, and (D) 3 months after aspiration and local injection of ruptured Baker cyst.

Seven serial longitudinal view photos of ruptured Baker cyst (A1-A7) at back of knee and extending up to the middle of the calf in a patient with rheumatoid arthritis and (B) 3 months after aspiration and local injection of ruptured Baker cyst.

Eight serial longitudinal view photos of ruptured Baker cyst (A1-A8) at back of knee and extending up to the middle of the calf in a patient with Psoriatic arthritis, (B) 1 week after aspiration and local injection of ruptured Baker cyst. Persistence of the complex cyst and disappearance of the extended part at the calf, and (C) 3 months after aspiration and local injection of ruptured Baker cyst.
Evaluation of treatment efficacy
Follow up were done clinically as well as via ultrasonography weekly until complete resolution of symptoms then 3 months later as regarding recurrence, complication, as well as the following parameters to assess pre/post-injection knee functions:
Visual analog scale (VAS) for calf pain: VAS is a subjective measure for evaluation the pain intensity evaluation. Patients indicate their degree of pain on a scale of 0 (no pain) to 10 (extreme pain).
Rauschning-Lindgren and Lysholm Knee Scoring Scales (RLC): patients were scored with RLC according to the following;11,12
– “0: No pain in the popliteal fossa and swelling, normal range motion.
– 1: Swelling and pain after hard exercise with minimal reduction of range motion.
– 2: Swelling and pain after soft exercise with reduction of range motion <20°.
– 3: Swelling and pain at rest with reduction of range motion >20°”.
Statistical analysis
The collected data were coded, entered, presented, and analyzed by computer using a data base software program, Statistical Package for Social Science (version 20, SPSS Inc., Chicago, IL). Quantitative variables were expressed as the mean ± standard deviation (SD) and median as the data was not normally distributed while the qualitative variables were expressed as a number and percentage. For quantitative variables, Friedman test for repeated-measures and Wilcoxon’s signed-rank test were used as appropriate for not normally distributed data. Cochran’s Q test and McNemar’s test were used to detect the difference in the same group. The results were considered statistically significant when the significant probability (P value) was <.05* and <.001** respectively.
Results
A total of (42) patients were included in the study, 12 (28.6%) patients were males and 30 (71.4%) were females, mean age (36 ± 10 years old). As regarding to the underlying diagnosis of the ruptured BCs patients in this study, we noticed higher frequency in RA (42.8%) while (37.5%) were with OA and (21.4%) with psoriatic arthritis (PsA) patients.
US images were also retrospectively reviewed to determine the type of the cyst before the procedure and demonstrated that 10 patients (23.8%) had simple BCs while 32 patients (76.2%) had complex BCs (Table 1).
Characteristics of the patients included in the study.

Abbreviation: BC, Baker’s cyst.
Table 2 shows that, on comparing RLC scale at pre injection& 1 week and at pre injection&12 weeks, there was statistical significant difference (P < .001) among the patients.
Clinical results of the procedure (RLC scale and VAS for calf pain) at the follow up visits.

Abbreviations: VAS, visual analog scale; RLC, Rauschning-Lindgren and Lysholm Knee Scoring Scales.
a Cochran ‘s Q test.
P1: between pre injection and 1 week, P2: between 1 week and 12 weeks, P3: between pre injection and 12 weeks.
b Friedman test for repeated-measures.
c Wilcoxon’s signed-rank.
P1#: between pre injection and 1 week, P2#: between 1 week and 12 weeks, P3#: between pre injection and 12 weeks.
Statistically significant difference.
Highly statistical significant difference.
Regarding VAS improvement for calf pain, there was statistical significant difference (P < .001) among the patients on comparing it at pre injection& one week, and at pre injection&12 weeks.
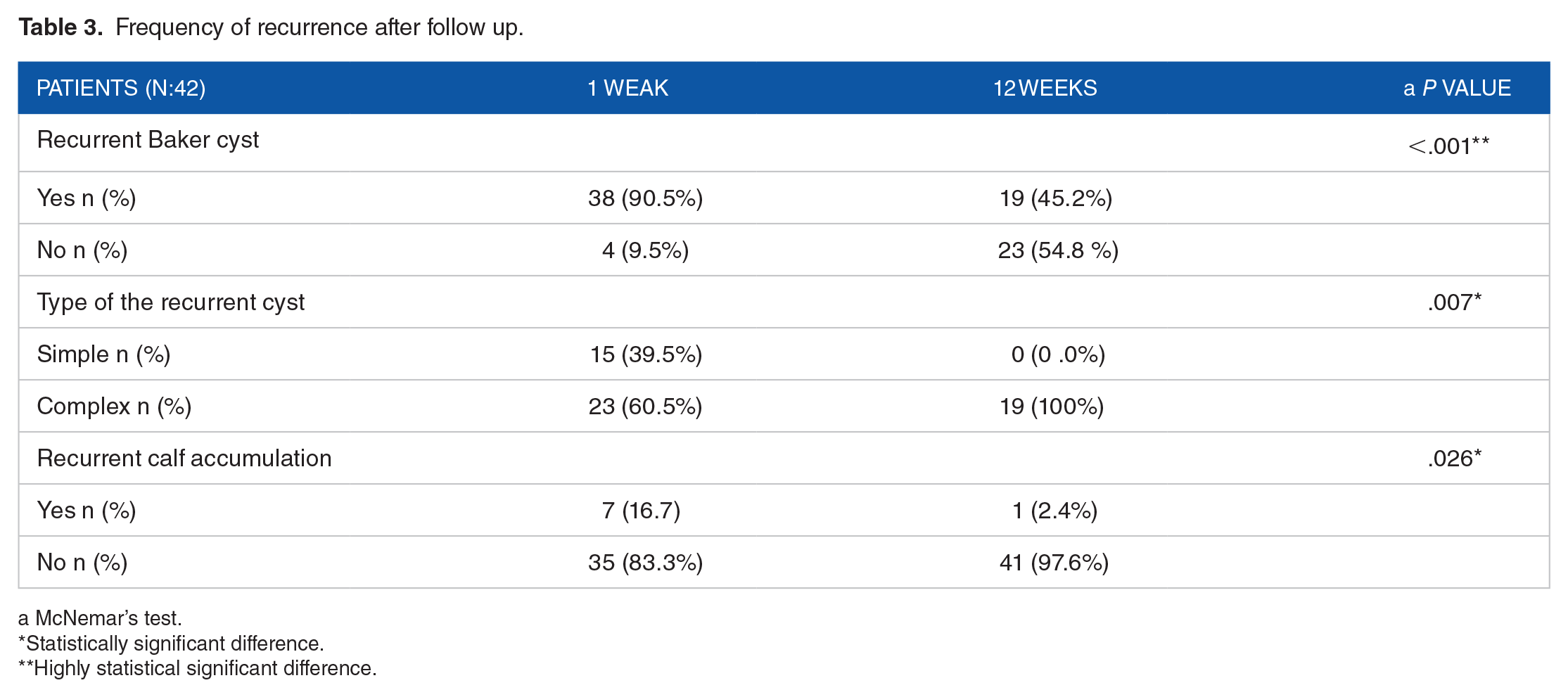
As regards BCs only 4 (9.5%) cases showed complete disappearance of the BCs after 1 week and in the majority of cases 38 (90.5%) there were recurrent BCs which required reaspiration after 1 weak, while After 12 weeks follow-up, we found improvement in the frequency of BCs recurrence as completely disappeared in 23 (54.8%) among the studied patients which was statistically significant difference (P < .001).
There was a general decrease in the number of the complex cyst on US during the study. After 12 weeks there was statistically significant difference in US-detected type of cyst, All BCs relapsed were complex type (P < .001).
Also, there was complete disappearance of free fluid at the calf in 35 (83.3%) cases 1 week after the injection, and in 41 (97.6%) after 12 weeks on US (P < .001) as shown in Table 3.
Frequency of recurrence after follow up.
a McNemar’s test.
Statistically significant difference.
Highly statistical significant difference.
Tables 4 and 5 show that no significant difference between initial diagnosis (Rheumatoid arthritis,Psoriatic arthiritis or Osteoarthritis) to Visual analogue scale, to RLC score and their improvement respectively.
Association between the initial diagnosis (Rheumatoid arthritis, Psoriatic arthiritis or Osteoarthritis) to Visual analog scale and their improvement.

Abbreviation: VAS, visual analog scale.
P value < .05: non-significant correlation.
Association between the initial diagnosis (Rheumatoid arthritis, Psoriatic arthiritis or Osteoarthritis) to RLC score and their improvement.

Abbreviations: RLC score, Rauschning-Lindgren and Lysholm knee scoring scales.
Discussion
To the best of the authors’ knowledge, this is the first study to demonstrate the efficacy and safety of ultrasonographic guided aspiration of ruptured BC performed in combination with intra-lesional corticosteroids injection. And this data analysis supports the use of ultrasonographic guided aspiration of fluid from the cyst and different points from the calf and corticosteroid injection as efficient and safe method for ruptured BCs management.
Ruptured BCs may trigger inflammatory alterations in the subcutaneous fat and muscles and have been linked to neurological deficit and compartmental syndrome. So, early management can therefore allow complete recovery and reduce these complications.13-15
Although treatment for BCs relies on the management of the underlying causative disease in order to decrease the rate of recurrence and the enlargement of the cyst, recent studies have demonstrated favorable clinical and songraphic follow-up results in patients managed by ultrasound-guided aspiration followed by injection of corticosteroid intra-articular or intra-lesional without surgery and still widespread practices.1,15 However, no studies have assessed the efficacy of ultrasonographic guided aspiration and corticosteroid injections for ruptured BCs.
Our data showed that the highest frequency of ruptured BCs was noticed in rheumatoid arthritis patients (42.8%), which is similar to another study, 16 which revealed that inflammatory pathology in ruptured BCs patients (66.7%) is higher than the degenerative disease (33.3%).
In the present study, we observed after 1 week and 3 months of treatment, that all the parameters showed a real improvement in all patients baseline as assessed by (VAS for calf pain and RLC score) after combination between ultrasound-guided aspiration of ruptured BCs and intra-lesional corticosteroid injection (P < .001).
Regarding the efficacy of the mentioned combination in this study, our results were consistent with the case report study, 10 the patient was diagnosed as having knee osteoarthritis who had a swelling on the popliteal fossa, suddenly complained of unilateral calf enlargement, pain, slight redness and warmth, diagnosis was confirmed as ruptured BC, ultrasound guided aspiration was performed followed by intra-lesional injection of corticosteroid. After 1week follow up, ultrasound revealed recurrent fluid collection in the leg, ultrasound guided re-aspiration was done and the pain was relieved with post- procedure resolution of the cysts, which was confirmed by US examination.
Similarly, another case report study was done in a rheumatoid arthritis patient, 17 within the report MUS was used for differential diagnosis and treatment. Inflammatory fluid was aspirated from the leg twice, one week apart and steroid was injected into right knee joint. During the follow up time, they noticed that the patient swelling and redness disappeared and the VAS value was decreased which continued to improve at the follow up visits. And they postulated the importance of ultrasonography in accurate diagnosis and proper treatment of pseudothrombophlebitis syndrome and to ensure that the whole fluid was aspirated entirely.
Therefore, after performing an extensive review of the literature, we did not identify any study, other than those previously mentioned,10,17 reporting on the results of the combination between ultrasound-guided aspiration followed by intra-lesional/ intra-articular injection of corticosteroid for rupture BC which were limited case reports. In our work, direct steroid injection into BC has been used which was based on the finding of other study 9 which stated that direct cyst injection can ensure direct infiltration and steroid might reach a higher amount inside the cyst rapidly. The study strength point is the use of MUS to document the outcome measures providing a more accurate assessment of the injections local effect.
In contradiction to us, case report literatures18,19 were conducted to evaluate early diagnosis of ruptured BC and its management thereafter, they concluded that most cases of ruptured BC are self-remitting, and can be treated by conservative therapy in the form of elevation of the affected leg and local heating, while surgical excision can be performed in rare cases. However, Additionally, in agreement with this study, a previously published study 20 emphasize the importance of MUS in the diagnosis of ruptured BC as powerful, rapid and easily available tool for examining a swollen leg.
Moreover, in this study we found the relapse frequency of BCs was (45.2%) at the end of follow up among the studied patients and additionally, we found that most of the relapsed cysts were complex BCs after 1 week follow up. As far as we know, no previous studies have investigated the recurrence rate in patients with ruptured BCs after the combination of aspiration and corticosteroid injection, but that mentioned rate of recurrence could be compared favorably with rate after excision surgically of BCs which has been reported to range from 5% to 70%.21-23
However, regarding the recurrence, a prospective cohort study was conducted, 24 which included a total of 32 knee osteoarthritis patients, they were divided into simple 24 (75%) or complex cyst 8 (25%) groups and follow up was done for 6 months clinically as well as via ultrasonography after BCs ultrasound-guided aspiration and direct injection of steroid. There was a significant improvement clinically and decreased cysts volume considerably in both groups, with 6 patients (19%) recurrences were reported in the complex type. Furthermore, they concluded that both complex and simple BCs gained same clinical benefits after the procedures. And they proposed that the procedure was an effective for managing both simple and complex BC subgroups.
Both of the following reasons may explain the difference between our results and previous discussed one. 24 The first potential reason is the underlying disease of patients in our study was different, and it affects the cyst type. The other potential reason is the follow up timing which was extended in their study for 6 months. So, it is beneficial to determine the cyst type as well as the nature of underlying intra-articular disorders in order to achieve optimal clinical results and provide the patients with reasonable expectation.
This study is in accordance with other literatures investigating the importance of MUS in the management of the usual BCs without rupture. Similarly, Ultrasound-guided BCs aspiration was used in combination with corticosteroid injection in osteoarthritis patients, showed significant clinical and ultrasonic improvement and they concluded that MUS can be used for the diagnosis of BCs and also to monitor the therapy response.25,26
Another, prospective observational study observed that after ultrasound guided aspiration of 26 popliteal cysts with steroid injection, there were statistically significant improvement on the visual analog pain scale, WOMAC pain scale, and cyst area after 1 month. 27 Moreover With regard to its therapeutic role, the implementation of MUS has shown greater accuracy and safety in several intra and/or peri-articular procedures with improved clinical results for various rheumatology practices. 28
Limitation: the study was retrospective, lack of comparison group for ruptured BCs, but treated conservatively and relatively small number of enrolled patients; we suggest long term follow-up more than 3 months is required.
Conclusion
Ultrasonographic guided aspiration followed by intra-lesional corticosteroids injection is an effective and safe method for managing ruptured Baker cysts. BCs should be classified as simple and complex subgroups before the treatment by ultrasound, and the complex subgroup should be more closely monitored for early and proper management.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
MM did all aspirations, injections and ultrasonographic examinations. YAA performed all clinical assessments and the RSZ contributed to the design and implementation of the research, to the interpretation of the results and wrote the manuscript. Each author made significant individual contributions to this manuscript. The manuscript has been read and approved by all the authors. Each author believes that the manuscript represents honest work.
Ethical Statement
Informed consents were obtained from all patients or families (in case of deceased patients). The study was approved by ethical committee of the institute and the study was conducted in conformity with Declaration of Helsinki.
Compliance with Ethical Standards
This study was approved by the ethics committee of the university (ZU-IRB#5556, Date: 28-8-2019) and all patients give written consent before injections The work described has been carried out in accordance with (Declaration of Helsinki).