
Abstract
Objectives:
Deteriorating functionality and loss of mobility, resulting from Parkinson’s disease, may be worsened by osteoarthritis, which is the most common form of joint disease causing pain and functional impairment. We assessed the association between symptomatic hip or knee osteoarthritis, falls, and the ability to walk among patients with Parkinson’s disease compared to a control group.
Methods:
A total of 136 patients with Parkinson’s disease in Southern Estonia and 142 controls with an average age of 76.8 and 76.3 years, respectively, were enrolled in a retrospective case-control study. Information on falls and related fractures during the previous year was collected from the patients with Parkinson’s disease and controls. Covariates included gender, age, mobility, duration of Parkinson’s disease, and fractures.
Results:
Patients with Parkinson’s disease were at an increased risk of falls compared to the control group, and for the higher risk of fractures. Symptomatic knee or hip osteoarthritis was a significant independent predictor of falls in both patients with Parkinson’s disease and controls. The higher risk for fractures during the previous year was demonstrated in symptomatic osteoarthritis. Risk factors for falls included also female gender, use of sleep pills, and the inability to walk 500 m.
Conclusions:
Symptomatic hip and knee osteoarthritis are risk factors for falls and related fractures among the elderly population with and without Parkinson’s disease. The inability to walk 500 m could be used as a simple predictive factor for the increased risk of falls among elderly populations.
Introduction
Parkinson’s disease (PD) is the most common neurodegenerative movement disorder, affecting approximately 1% of people above 60 years old in Estonia. 1 Prospective and retrospective studies have reported a high frequency of falls among PD patients (up to 68%, compared to 18% among control subjects without PD).2 -6 Falls are particularly problematic in PD due to the high risk of hospital admittance with approximately 50% of PD fallers requiring medical care. 2 Furthermore, hip fractures resulting from falls in people with PD results in higher morbidity and mortality compared to healthy older adults. 4 Previously, the best predictor of a fall has been a previous fall, 3 thus, predictors of future falls – particularly in PD – continue to be sought.
Risks for falls in PD are complex and multifactorial: in addition to common risk factors such as older age, female gender, low body mass index (BMI), low bone mineral density, depression, dementia and anxiety, longer disease duration, and fear of falling,2,3,7 -11 there are additional disease-specific factors related to motor and nonmotor symptoms. Prediction models have also identified such risk factors of falls like freezing of gait, disease severity, slow mobility, and poorer balance.6,12 In a falls-naive cohort of de novo PD, discrete gait characteristics of gait speed and stance time emerged as significant predictors of the first fall. 13 Different factors relating to falls were considered among community-dwelling older people, including sociodemographic, mobility, sensory, psychological, and medical factors (including the use of medications); among them, the strongest correlations were with a history of falls, gait problems, the use of walking aids, and fear of falling. 14
Arthritis is commonly associated with falls in older adults.7,14 -16 The presence of comorbidities has been shown as an independent risk factor for falls in PD 6 ; however, according to our best knowledge, the separate effects of arthritis have not been investigated in PD patients. Osteoarthritis (OA) is the most common form of arthritis and is one of several chronic conditions that is becoming more prevalent with the ageing population.17,18 The association between OA symptoms and imaging findings is inconsistent and variable in different joints. 18 In general, estimates of OA based on radiologic parameters present higher estimates than those based on a symptomatic definition of OA.18,19 Radiographic knee OA was detected in 25.4% of the general population in a Nordic cohort study, but only 15% of middle aged or elderly individuals from the same cohort had symptomatic knee OA, with the Kellgren-Lawrence (KL) score ⩾2, and joint pain. 20 The risk of developing OA may be higher in PD patients than the general population. 21 It has been estimated that falls causing fractures occur more frequently in PD patients than controls and are associated with female gender and underlying knee OA.2,22,23 The mechanism of falls in PD patients with OA has not been established, but arthritis may lead to inactivity and thereby leg muscle weakness, which in turn would predispose patients to gait abnormalities and a loss of body mass, possibly resulting in falls and fractures.7,24,25
The purpose of this study was to determine the risk of falls in PD patients and a non-PD control group, and the potential influence of symptomatic hip or knee OA upon falls. The presence of OA has not been shown as an independent risk factor for falls in PD. We hypothesise that patients with PD fall more often than persons without PD; symptomatic OA and the moving capability are predisposal factors of falls in PD and the elderly population.
Materials and methods
The study was carried out in the Tartu and Põlva districts of the Southern Estonia with a population of approximately 240,500. The data were collected over the period 2012 to 2014.
Participants
This cross-sectional study recruited PD participants from the epidemiological database of the Department of Neurology of the University of Tartu (Estonia). Inclusion criteria were as follows: (1) confirmation of the diagnosis of idiopathic PD by a neurologist according to the UK Brain Bank criteria 26 ; (2) the patient visited neurologist at least once during the past 5 years; (3) the patient was a resident of Tartu or Põlva District. The control group consisted of age-matched subjects without PD diagnosis who were recruited from general practitioners. Exclusion criteria for both groups were a limited ability to complete the questionnaire and complicated cardiovascular, metabolic, or other neurologic conditions that would interfere with moving and balance.
Data collection
Demographic data and history of the disease have been obtained from the database of the recent epidemiological study 1 ; information on falls has been collected with a self-assessment questionnaire designed for the study that has been sent to the patients, and health data on other diseases including OA was obtained from the database of the Estonian Health Insurance Fund. The self-assessment questionnaire with items on pain and movement abilities, use of medicines (asked to name all medicines in use constantly), number of falls and fractures during the previous year, was sent to 250 PD patients. We collected 136 answers (response rate of 54.4%). Falls are defined as unintentionally coming to rest on the ground or other lower surface without overwhelming external force or a major internal event. 27 The control group filled in the questionnaire during the visit to their general practitioner. The data on duration of PD were collected, and all participants were asked on their ability to walk in one go (response options were: 500 m and over; 100–500 m; 10 m; bedridden). In addition, from the Health Insurance Fund databases, we collected data on number of bone fractures due to falls during the preceding 10 years.
Pain evaluation was a part of the self-assessment questionnaire to determine the presence or absence of chronic pain in each knee and hip joint. The subjects reporting knee or hip pain lasting at least 4 weeks were referred as having frequent pain. All the participants with knee or hip pain who had no hip or knee X-rays due to pain were invited to imaging investigation. Radiologic knee and hip scans were classified using the KL 0–4 score 28 by an orthopaedic radiologist, according to the Osteoarthritis Research Society International (OARSI) criteria. 29 The knee OA is defined as having radiographic OA if either the KL score at the tibiofemoral joint was ⩾2 or OA was present at the patellofemoral joint based on OARSI criteria. Symptomatic knee or hip OA was defined if pain occurred on most days during the past month and radiographic OA was present on the same knee or hip. A participant was considered as having symptomatic OA if they had specific changes at least in 1 of the 4 joints.
Fall classification
The PD and control groups were each divided into 2 groups: (1) fallers and (2) nonfallers. A ‘faller’ was defined as someone who had fallen at least once during the previous year; a ‘recurrent faller’ was someone who had fallen at least twice during the same period.
Patients with PD have been divided also into different groups by PD duration: under 1 year, 1 to 3 years, 4 to 5 years, 6 to 10 years, and more than 10 years.
Data analysis
For the statistical analysis, both the exposure (symptomatic OA) and outcomes (falling during previous year and fall-associated fractures during the previous year) were binarised. The chi-square and Mann-Whitney U-tests were used to compare parameters of fallers and nonfallers separately for PD participants and controls. The localisations of fractures were collected for last 10 years in PD and control groups to specify the fracture locations. Two univariate logistic models were built up for PD patients: the first explored the association between falls and the presence of symptomatic OA. For the second model, the dependent variable was a fracture associated to a fall during the previous year. The results were adjusted for sex and age. The results were presented as odds ratios (ORs) with 95% confidence intervals (CIs).
Our primary endpoint was to evaluate the rate of fallers between PD and healthy controls and to determine the potential influence of symptomatic hip or knee OA upon falls and fall-associated fractures. As secondary analyses, we evaluated whether walk ability could be a predictor of falls.
Ethical aspects
This study was approved by the Research Ethics Committee of the University of Tartu. A written consent was obtained from every patient.
Results
Participants
A total of 136 PD participants and 142 control participants were recruited to the study. Participant demographics are shown in Table 1. The PD group were aged between 49 and 98 (median = 77) years, of which 62% were female and 38% were male. The control group consisted of 142 subjects, age = 57 to 90 (median = 76) years; female = 62%. The PD participants and control group did not differ significantly in terms of age or gender (Table 1).
Demographic and clinical characteristics of participants (PD group and controls).
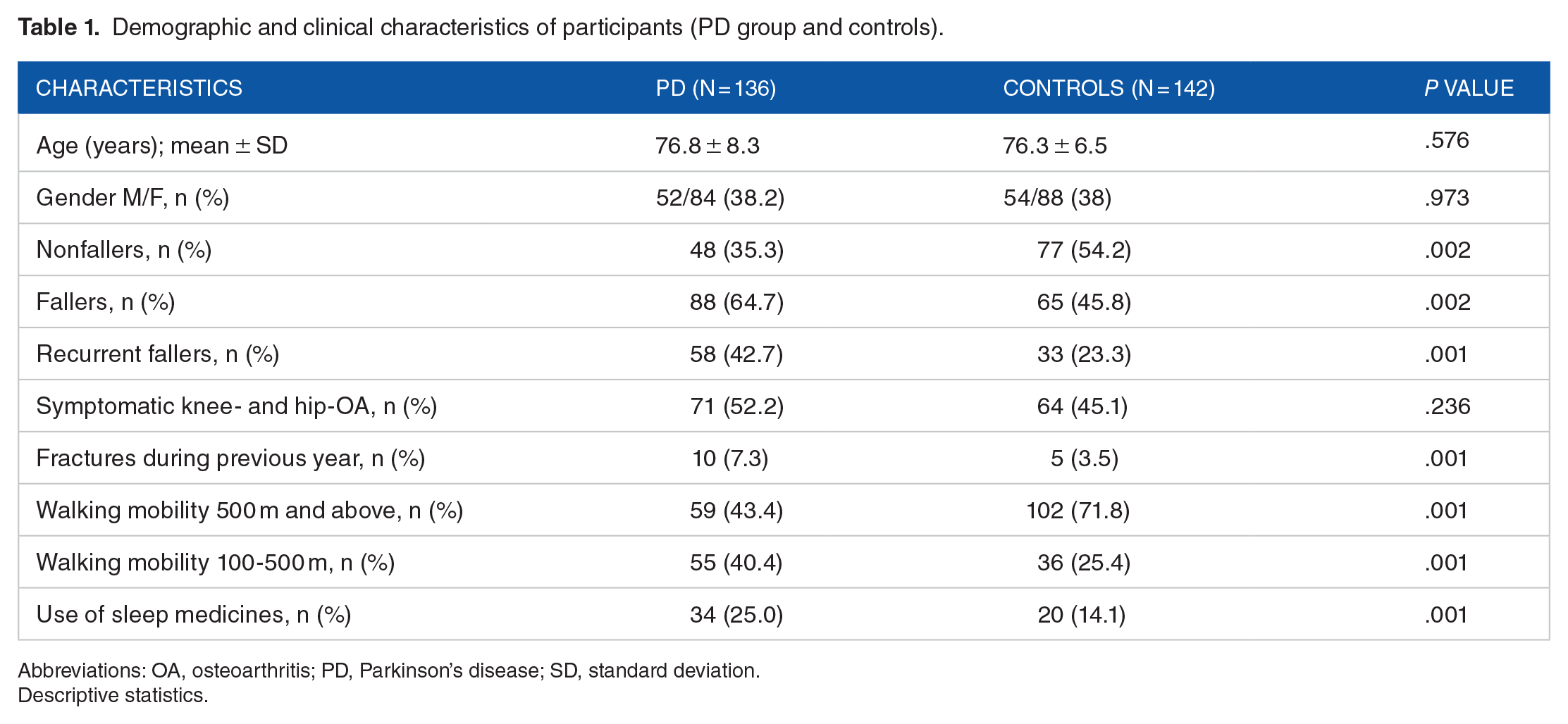
Abbreviations: OA, osteoarthritis; PD, Parkinson’s disease; SD, standard deviation.
Descriptive statistics.
Symptomatic knee and hip OA as a predictor of falls
Symptomatic OA of the hip and or knee joints was detected in 52.2% of PD subjects and 45.1% of control subjects. Knee or hip OA was a significant independent predictor of falls in both groups: PD (OR = 3.33, 95% CI = 1.6-7.0, P = .001) and controls (OR = 3.53, 95% CI = 1.8-7.1, P = .001). If calculated by logistic regression, univariate analysis for risk factors of falling in PD t is 4.2-fold higher risk to fall in PD group with OA (Tables 2 and 3).
Comparison of fallers and nonfallers in PD group.

Abbreviations: CI, confidence Interval; OA, osteoarthritis; OR, odds ratios; PD, Parkinson’s disease, SD, standard deviation.
Univariate logistic model.
Comparison of fallers and nonfallers in the control group.

Abbreviations: CI, confidence Interval; OA, osteoarthritis; OR, odds ratios; PD, Parkinson’s disease, SD, standard deviation.
Univariate logistic model.
Fractures and falls
Patients with PD were more likely to have fallen once (64.7% in PD group and 45.8% in controls) and experience recurrent falls (42.7% vs 23.3%). Patients with PD had a total 2.2-fold higher risk of falling (including recurrently) compared to the control group (OR = 2.19, 95% CI = 1.3-3.6, P = .002). Female PD patients were at a higher risk of falling than male PD patients (OR = 3.24, 95% CI = 1.5-6.3, P = .001), but there was no significant difference between women and men in the control group. There was no statistical association between age and incidences of falling in either the PD or control groups (Tables 2 and 3).
Patients with PD had a total 2.1-fold higher risk of getting fracture compared to the control group (OR = 2.07, 95% CI = 1.1-3.0, P = .027). During the previous year, 10 subjects (7.3%) in the PD group and 5 (3.5%) in the control group had experienced a bone fracture (Table 1). There was no statistically significant association between symptomatic OA and having fracture in PD or control group separately, but when the PD and control groups were combined, in total there was a 2.9-fold higher risk of fractures among participants with symptomatic OA than those without during the previous year (OR = 2.94, 95% confidence limit [CL] = 1.02-8.49, P = .046).
There was no significant difference between age and incidence of fractures among either the PD group (P = .979) or controls (P = .175). Women had 8.5-fold higher risk for fractures during the previous year among the PD group (OR = 0.12, 95% CL = 1.15-9.34, P = .027), but no significant difference between the genders and incidence of fractures occurred among the control group (P = .066).
The analysis during the preceding 10 years showed that there were more fractures in the proximal femur and shoulder in the PD group (Table 4).
The distribution of fracture localiztion in patients with or without PD and controls within the preceding 10 years.

Abbreviation: PD, Parkinson’s disease.
Descriptive statistics.
Falling and PD duration
The percentage of having fallen at least once was significantly higher for patients who had suffered from PD for 4 to 5 years (incidence of falling/nonfalling = 15.9%/2.1%, OR = 3.99, 95% CL = 1.765-9.029, P = .01) than those who had suffered from PD less than 1 year (incidence of falling/nonfalling = 5.7%/10.4%, P = .036) without significant difference versus PD group 5 to 10 years (incidence of falling/nonfalling = 21.6%/14.6%, OR = 1.76, 95% CL = 0.107-28.919, P = .693; Table 2). Logistic regression analysis showed that PD duration in total did not have a significant effect on falls.
Falling and use of medicines
Logistic regression analysis showed that using sleep pills in PD group increase the risk of falling 3 times (OR = 3.0, 95% CL = 1.519-5.929, P = .01; Table 2) and getting fracture up to 2.1 times (OR = 2.1, 95% CL = 0.095-4.456, P = .027). Control subjects also had an 8.74-fold higher incidence of falling when using sleep pills (OR = 8.74, 95% CL = 7.015-31.400; P = .0001; Table 3).
There were no significant correlations between falls and using of beta blockers, calcium channel blockers, or angiotensin-converting enzyme inhibitors (Tables 2 and 3).
Functional state
Forty-three percent (59 subjects) of the PD group and 72% (102 subjects) of the control group were able to walk independently more than 500 m, with or without a walking aid at least before last fall complicated with fracture.
There were significant correlations between falls and mobility: participants with PD who was able to walk a maximum of 500 m, had a 2.4-fold higher risk of falls than PD participants able to walk more than 500 m (OR = 2.41, 95% CL = 1.1-5.3, P = .011; Table 2). Similar correlation has been found in control group as 4-fold higher risk of falls than the control group (OR = 3.99, 95% CL = 1.8-9.0, P = .001; Table 3).
Discussion
This cross-sectional study aimed to find the association between symptomatic knee and hip OA in association with falls in a cohort of PD and a control group of matched elderly population without PD. We demonstrated that one of the main risk factors for falls among PD and control groups was symptomatic knee or hip OA, already known to be a risk factor for falls among the elderly population. 16 The importance of the study is to pay attention to symptomatic OA as a separate disease in PD patients and a powerful possible factor to trigger falls.
In our study, the incidence of OA in the hip and knee in people with PD was high as 52.2% which is comparable to a previous large cross-sectional cohort, who reported OA to be in 47.2% of PD patients. 6 There is a difference between estimation of OA in different countries. The age-standardised prevalence of radiographic knee OA in adults aged ⩾45 was 19.2% among the participants in the Framingham Study and 27.8% in the Johnston County Osteoarthritis Project.17,30 The WHO data on an estimated risk of OA are 10% to 15% in all adults aged more than 60 years. 31 In a cross-sectional Germany study, 32 hip and knee OA in people aged 60 years or above was 21.8% to 31% with a total of 595,754 patients included, using unidentified data claims from the Health Insurance Fund without radiologic findings. It is known that lifetime risk of OA increase with increasing BMI. 33 This could be relevant for Estonians who have a higher body weight in comparison to Germans or other European countries. 34 An Estonian study on OA in population aged 34 to 54 years, OA I stage has been found in 50% of cases. 35 However, for conclusion, the bigger control group might be needed.
The results of this study confirm the findings of previous studies and foster domain-general strategy knowledge2 -5,9,23,24,36 with regard to a higher risk of falls and receiving fractures as a result among PD participants. Approximately, 65% of our PD participants had experienced falls, which is comparable to several prospective and retrospective studies2 -5,9 that reported a risk of falls among PD participants of up to 70%, and recurrent falls of up to 51%.
Importantly, our study also determined OA incidence was significantly higher in PD fallers than nonfallers. Falls are the causative events of most fractures among elderly populations and in PD.7,37 In that case, OA may play a big role in maintaining balance and rise of falls and fractures of PD patients.
Locations of fractures over the previous 10 years were also different among groups in our study. Compared to controls, for which the most common fracture was in the distal forearm, the most common fracture sites in PD were the proximal femur, shoulder, and distal forearm. These results were similar as those of Genever (2005) who found that the most frequent fracture site was femur in PD patients, and the forearm in controls. 22 This may demonstrate a fall model in patients with PD.
The number of studies has been demonstrated that women have a higher risk of falling, both in PD and the general elderly population.10,11,35 In our study, we found significantly increased risk of falls and fractures in female of the PD group, but it was not seen in healthy older adults.
The logistic regression analysis detected also that the risk for fractures is higher if participants use sleep pills. This is also an important knowledge for healthcarers.
In this study, a significant predictor for falls was the inability to walk 500 m among both the PD participants and controls. Considering the results of the different surveys on mobility disturbance among PD patients and controls,8,10,15 the inability to walk 500 m could be a simple predictive factor of falls. Preserving the ability to independently and safely cover a distance ⩾500 m, with or without a mobility device, could be important to reduce the risk of falls in elderly people and should be investigated further.
The main limitation for our study was the method of retrospective self-reporting of the falls. A prospective longitudinal study would provide more information on the potential impact of knee and hip OA on the movement abilities, and risk of falling among elderly populations including PD patients.
In conclusion, we identified that the hip and knee OA are significant risk factors for falling in PD participants and elderly people and that those with PD were more likely to fracture as a result of a fall compared to older adults. These results may have important clinical implications in clinical management of elderly population and participants with PD. Patients who report falls should be examined for joint diseases that may impair patients’ movement and increase the incidence of fractures caused by falls. The inability to walk 500 m could be a simple predictive factor of falling. The results of this study suggest the need for longitudinal follow-up studies involving larger cohorts and more efficient interventions for the prevention of falls among elderly people to reduce the risk of fractures and other serious adverse health consequences.
Footnotes
Funding:
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: This study was supported by the Grant PUT1239 of the Estonian Research Council. The funders had no role in study design, data collection and analysis, decisions to publish, or preparation of the manuscript.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
PT, ATB, AM- study design, data collection, data analysis, article writing; MR- data analysis, statistics, article writing.