
Abstract
The association of HLA-B27 with ankylosing spondylitis (AS) remains as one of the intriguing models that could exist between a molecule and human disease in medicine. Although it was reported in 1973, its contribution to AS and related spondyloarthritis continues to be a major challenge for scientific community. It is important to understand its etiopathogenic mechanism and its functions in these diseases. Although the diagnostic and prognostic roles of HLA-B27 in AS are still debated, there is an increasing interest for HLA-B27–based effects especially in HLA-B27(+) patients with AS. This review will focus in the examination of published reports regarding the influence of HLA-B27 status on the demographic and clinical features in AS, with specific interest to its role on AS severity.
Introduction
Ankylosing spondylitis (AS) is a common chronic inflammatory rheumatic disorder from the group of spondyloarthritis (SpA), which affects sacroiliac joints, spine, and peripheral arthritis. 1 This disease is more common in young adult men, with a sex ratio of approximately 3:1 (M:F). 2 The estimated prevalence of this disease is 0.23% in European population and 0.16% in Asia 3 and lesser common in African population. 3 Strong evidence of familiality and heritability has been shown in patients with AS. 4 Although the improved treatments that suppress inflammation and improve symptoms are available, they still have been unable to induce disease remission.
Numerous studies have indicated the implication of genetic and environmental factors in the predisposition and the susceptibility to the AS. 5 In fact, AS has long been associated with HLA-B27 (human leukocyte antigen B27) with large percentage and it is a remarkable example of a disease association with a genetic marker.5–7 Most patients with AS express HLA-B27 (90%), whereas the frequency of this gene in the general population is less than 8%.6–8 However, the pathogenetic role of this gene has not been convincingly explained to date. Various hypotheses have been raised to describe the mechanism by which HLA-B27 could develop AS (Table 1): (1) the arthritogenic peptide hypothesis assumes that the existence of a molecular mimicry between pathogens and self-peptides could be at the origin of cytotoxic T cell lines (CTLs) cross-reactivity, leading to AS 9 ; (2) the HLA-B27 misfolding hypothesis enunciates that the accumulation of aberrant folded HLA-B27 in endoplasmic reticulum (ER) activates an intracellular signaling, leading to ER stress and unfolded protein response 10 ; (3) the hypothesis relating the formation of HLA-B27 homodimer on cell surface to an abnormal immune response, these dimers are recognized by specific receptors—the killer immunoglobulin-like receptors—expressed on the surface of natural killer and CD4+ T cells. 11
Hypotheses explaining pathogenic mechanism of HLA-B27 in AS.

Abbreviations: APC, antigen-presenting cell; AS, ankylosing spondylitis; FHC, free heavy chain; KIR, killer cell immunoglobulin-like receptor; TCR, T-cell receptor; UPR, unfolded protein response.
Despite extensive searches to resolve the mechanism of action of HLA-B27 in AS, the question remains open and not fully resolved. The highlighting of immunobiological features of HLA-B27 may contribute to dissect the exact role of this molecule in the pathogenesis of AS.
One of HLA class I molecules, HLA-B27, is encoded at the B locus of the major histocompatibility complex located in the short arm of chromosome 6. 12 The quaternary structure of mature class I consists of a heavy chain, β2-microglobulin, and a short peptide derived from self-proteins and/or intracellular pathogens. The traditional function of HLA class I is to present the peptides to CTLs to initiate immune responses. 13 Furthermore, the HLA-B27 shows a high degree of polymorphism resulting from nucleotide substitutions in exons 2 and 3, which encode the α1 and α2 domains of the B27’s heavy chain. 14 This high polymorphism may not only influence the specificity of binding antigenic peptides but also can play a role in the pathogenicity and susceptibility of AS.
Currently, more than 160 subtypes of HLA-B27 have been identified, namely, HLA-B*27:01 to HLA-B*27:161, and encoded by 213 allelic variants. 15 There is evidence that the distribution of HLA-B27 subtypes worldwide is widely influenced by the race and the ethnicity with different strengths of association with AS. 15 The most common disease-associated subtypes are B*2702 (Mediterranean population), B*2705 (whites and American Indians), and B*2704 (Asians); this association subtype-AS is confirmed in multiple population studies and commonly recognised.15–17 Most other subtypes are found in small frequency, and their relationship to the disease is somewhat more problematic (Figure 1).
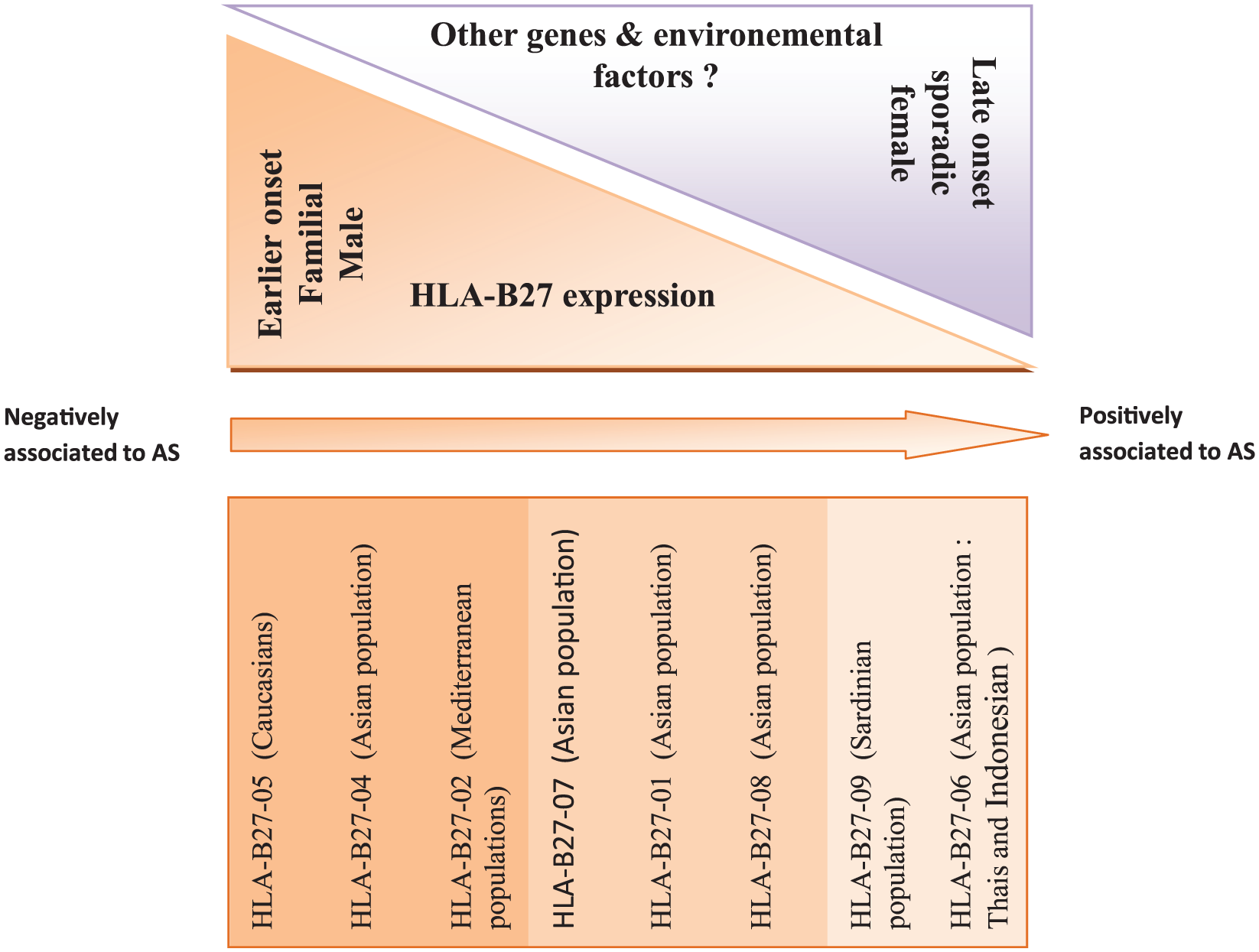
Model for the relationship between HLA-B27 and AS and the degree of association between HLA-B27 subtypes and AS: B27-06 and B27-09 conferring protection to AS in different populations. B27-05, B27-04, and B27-02 are the common AS-associated subtypes. B27-08 and B27-06—the evidence of the association with AS is still not conclusive. AS indicates ankylosing spondylitis.
Recently, a new concept has emerged: the axial SpA (axial SpA), which englobes both the patients with nonradiographic (AS without sacroiliitis) and with radiographic axial SpA (AS). 18 The nonradiographic SpA (nr-axSpA) is considered to be an early stage of AS.18,19 Although the diagnosis of nr-axSpA is somewhat problematic, many studies have been working on the development of approaches to facilitate this diagnosis,18,19 which is essential for the choice of effective treatments. This diagnosis is based on the combination of a set of clinical, biological, and radiographic indices. In this context, HLA-B27 could play a crucial role in diagnosis of axial SpA without radiologic evidence. Indeed, the study of Rudwaleit et al reported, in HLA-B27(−) patients with inflammatory back pain and without imaging evidence, that at least 3 SpA features (enthesitis, dactylitis, uveitis, positive family history, etc) are needed to evoke axial SpA, whereas only 1 or 2 SpA features are needed in HLA-B27(+) patients. 20
In addition to the diagnostic value of HLA-B27 in AS, HLA-B27 positivity is one of the key issues that might affect AS phenotype and susceptibility. Indeed, several studies suggest that HLA-B27(+) patients with AS are more severe clinically and radiologically than those without HLA-B27.21,22 It is in this perspective, this review proposes to discuss the influence of HLA-B27 status (ie, the presence of HLA-B27 gene in patients with AS vs the absence of this gene in patients with AS) on the phenotype of AS based on what has been reported in the literature. The search approach of this review is focused on AS, which offers more available and exploitable data than nr-axSpA.
HLA-B27 Status and Sex Distribution
Several studies showed a male prevalence in the HLA-B27(+) AS group.23,24 In fact, based on HLA-B27 status, the number of male patients with HLA-B27 was higher than male patients without HLA-B27 in those studies. Thus, a representative study of Yang et al 23 conducted on Chinese patients with AS showed the following distribution of sex based on HLA-B27 status: 80.2% of male patients with AS with HLA-B27 vs 72.4% without HLA-B27 (P < .001). Other study based on sex status comparison in patients with AS revealed that men have a greater HLA-B27(+) rate. 25 To explain the relationship between sex ratio and HLA-B27, a study proposed that the antigen HLA-B27 is linked with high concentrations of testosterone in men. 26 If this is correct, then one would expect that HLA-B27 could serve as a diagnostic and prognostic marker for AS in men.
HLA-B27 Status and the Age of Onset Distribution
The clinical picture of early-onset AS differs from that of adult-onset AS, which makes the age of onset an important factor in AS phenotype. Regarding the relationship between HLA-B27 and the age of onset of AS, many studies have shown that HLA-B27 patients have a younger age of onset.27,28 Other studies based on the age of onset of AS reported that late-onset patients with AS were characterized with lower frequency of HLA-B27 positivity, lower levels in inflammatory markers, delay in diagnosis, and lower usage of methotrexate, and anti–tumor necrosis factor α drug. 29 The association between age of onset and HLA-B27 positivity is an interesting feature of AS, which may play a predictive tool to evaluate the disease evolution and prognosis.
Another factor as important as the age of onset is the delay between the first spondyloarthritic symptoms and diagnosis; Feldtkeller et al 28 showed that the average delay is significantly longer in HLA-B27(−) than in HLA-B27(+) patients with AS.
HLA-B27 Status and the Family History of AS
The strong genetic component of AS predisposition has been shown in familial and twins’ studies. The monozygotic twins’ recurrence risk of AS is 63% compared with 0.1% in the general population. 30 The most important part in the inheritance of AS comes from the HLA-B27. Indeed, a number of updated works based on the correlation between HLA-B27 status and family history of AS revealed a relatively higher percentage of family with AS history in patients with AS with HLA-B27 compared with patients with AS without HLA-B27,23,24 and risk of AS is 16 times greater in the HLA-B27(+) relatives compared with isolated individuals with HLA-B27 in general population.31,32 In addition, a representative genetic study based on the comparison of the genetic data between confirmed familial and sporadic cases of AS demonstrated a higher familial aggregation of AS in HLA-B27 patients with AS (P = .0001; odds ratio: 4.44, confidence interval: 2.06-9.55). 33 Another interesting study of the seemingly healthy first-degree relatives (FDRs) of HLA-B27(+) patients with AS showed clinical signs and imaging abnormalities suggestive of SpA with 33% FDRs fulfilling SpA. 34 These findings demonstrate that HLA-B27 might not only affect familial occurrence of AS but also open the way to make from the HLA-B27 useful marker for early management of disease in families with AS history.
HLA-B27 Status and Clinical Manifestations
The possible correlation among different clinical manifestations and HLA-B27 status in patients with AS was identified. Indeed, some studies have reported that HLA-B27 is associated with a higher prevalence of uveitis and cardiac involvement in patients with AS.35,36 Using regression analysis, Xiong et al 37 showed that HLA-B27 positivity was associated with worse sacroiliitis on computed tomography imaging. In addition, the large-scale study of Yang et al 23 revealed that HLA-B27(+) patients with AS have significantly more symptoms of spinal column involvement (lumbar spine and thoracic spine), hip joint involvement, and peripheral involvement than HLA-B27(−) patients with AS. The hip joint involvement correlation with HLA-B27 status was confirmed in a Korean population by both the studies of Kim et al. These studies demonstrated the involvement of the higher frequency of hip joint in HLA-B27(+) AS compared with HLA-B27(−) AS.38,39 Moreover, it has been shown that the ratio of sacroiliac joint involvement increases significantly in HLA-B27(+) patients. 27 Further studies revealed that uveitis/iritis and a worse visual prognosis were more frequent in the HLA-B27(+) AS group compared with their HLA-B27(−) patients with AS.21,23,40–42 Effectively, a meta-analysis study, exploring the clinical aspects of the HLA-B27 with acute anterior uveitis, reported that the incidence of AS is higher in the HLA-B27(+) group. 43 In addition, the cross-sectional study conducted by Fallahi et al 44 found no significant differences between HLA-B27(+) and HLA-B27(−) groups for hip involvement, primary involved joint, enthesitis, decrease in lumbar lordosis, and sacroiliitis grading. However, HLA-B27(+) was associated with peripheral arthritis, increase in dorsal kyphosis, and decrease in cervical slope. 44
HLA-B27 Status and Severity
Some researchers have suggested that disease severity of AS might be related to HLA-B27 status. In fact, Freeston et al 22 reported that HLA-B27(+) patients with AS have significantly longer disease duration and present worse Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), Bath Ankylosing Spondylitis Functional Index (BASFI), and Ankylosing Spondylitis Quality of Life (ASQoL) compared with HLA-B27(−) AS. Moreover, these authors showed that HLA-B27 has strong positive influence on the incidence and severity of extra-articular/musculoskeletal manifestations of inflammatory disease including ocular, cardiac, and respiratory diagnoses. 22 Furthermore, Vargas-Alarcón et al 45 showed that the Bath indices for disease activity and functioning were higher in HLA-B27(+) patients, which is in line with the work of Popescu et al 46 which revealed that HLA-B27(+) patients have a median BASDAI 5 times higher than HLA-B27(−) patients (P = .033).
In a meta-analysis study, Linssen 21 reported that more severe spinal disease and more frequent peripheral arthritis in B27(+) patients with AS compared with B27(−) ones. Finally, other studies suggested that severity based on HLA-B27 presence may be reflected by elevated inflammatory markers such as higher erythrocyte sedimentation rate and C-reactive protein.21,47,48
HLA-B27 Status and Other Genes
Several studies conducted on patients with AS without HLA-B27 allowed a wider view of non–HLA-B27 genetic susceptibility factors related to AS. 47 However, some of these genes have a strong relationship with HLA-B27.
Of particular interest is ERAP1 gene, which encodes an ER aminopeptidase 1 that plays a role in peptide trimming before HLA class I presentation. It shows a strong genetic association with AS risk,48–50 first reported in 2007 by the “Wellcome Trust Case Control Consortium” (WTCCC) and “Australo-Anglo-American Spondylitis Consortium” (TASC), and this association is restricted to HLA-B27(+) patients with AS. The digenic epistatic relationship between ERAP1 and HLA-B27 supports the hypothesis that the mechanism of action of HLA-B27 in AS involves aberrant processing of antigenic peptides’ presentation.51,52 The discovery of the mechanism by which HLA-B27 and ERAP1 interaction contributes to the pathogenesis will open the way to better AS understanding and management.
Another, gene-gene interaction is HLA-B60 and HLA-B27. Indeed, numerous studies revealed that the strong epistatic interaction between these 2 genes increases the risk of AS susceptibility.53,54
Does HLA-B27 Subtypes Influence AS Phenotype?
The association between certain HLA-B27 subtypes and AS has been well demonstrated in many racial and ethnic groups throughout the world. The most common subtypes are B*2705, B*2704, and B*2702. However, the evidence that HLA-B27 subtypes may influence the AS phenotype is an issue which has raised considerable debate. Indeed, even though some researchers have shown that B27 polymorphism may affect disease phenotype,27,44,55–58,59 other studies reported no correlation between B27 subtypes and clinical features of AS. 60 Table 2 summarizes the findings of some studies that have reported the relationship between B27 subtypes and AS phenotype.
Finding from published studies of the influence of HLA-B27 subtypes on AS phenotype.

Abbreviation: AS, ankylosing spondylitis.
Conclusions
In summary, several features of AS, especially age of onset, sex, and family history, appeared to be influenced by HLA-B27. Effectively, the patients with AS with HLA-B27 were more prevalent among young men with relatively higher percentage of family with AS history. In addition, these patients presented more severe and active disease. These results confirm that HLA-B27 may play a predictive role in diagnosis and prognosis and could also present new insights in terms of a therapeutic tool.
Footnotes
Funding:
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Mohammed V-Agdal University “plan d’urgence” research grant.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
AA and YB contributed to the design and writing of this manuscript and read and approved the final manuscript.