
Abstract
Objective
This study assessed the association between various routes of tobacco use and hypertension while exploring the roles of confounders and effect modifiers among the adult rural people of Bangladesh.
Methods
A cross-sectional study was conducted with a combination of open and closed-ended questionnaires. Data were collected from 496 adult rural patients during their doctor visits. All the data were analyzed using SAS 9.4 statistical software. Continuous variables were summarized as Means (M) and Standard Deviations (SD), and categorical variables were summarized as frequencies and proportions. Logistic regression model assessed associations with Odds Ratios (ORs) and 95% Confidence Intervals (95% CIs).
Results
Among the 496 participants, 50.8% were female, with an average age of 49.5 ± 11.8 years (M ± SD). 19/496 (3.83%) of inhaled smoker participants had hypertension. 58/496 (11.69%) of the chewing tobacco users were discovered to be hypertensive. The combined use of both inhalation and chewing tobacco was associated with higher odds of hypertension (OR = 1.27, 95% CI: 0.64-2.49), while inhalation tobacco was not (OR = 0.16, 95% CI: 0.05-0.53). Betel leaf use was prevalent among chewing tobacco users but did not significantly modify the association with hypertension. Age was identified as an independent variable that did not confound or modify the association between tobacco use and hypertension.
Conclusion
Together, inhalation and chewing of tobacco may increase hypertension risk, necessitating targeted public health interventions to curb its use among adult Bangladeshi rural populations. Nevertheless, we cannot establish temporality or causality from this study.
Introduction
The use of all types of tobacco products creates a significant public health burden globally. According to the World Health Organization (WHO), tobacco is one of the leading causes of cardiovascular disease and mortality. In South Asia, the use of both inhalation and chewing tobacco is increasing very rapidly. 1 The high prevalence of tobacco use in developing countries, including Bangladesh, indicates a looming public health crisis. 2 Bangladesh has extensive tobacco cultivation, industry, and many people are involved in tobacco farming and processing. 3 Various forms of tobacco, including Zarda, dried tobacco leaf, Gul, Sada Pata, and Khoinee, are commonly consumed in the countryside. 4 Notably, 58% of men and 29% of women in Bangladesh are using tobacco, and 46.3 million adults are using at least one form of tobacco. 5 Chewing tobacco use is particularly prevalent among women. 6 The number of tobacco users has dramatically increased by 80% from 1997 to the present. 7
The use of chewing tobacco is skyrocketing in both the USA and Asia.8,9 In Southeast Asia, it is often combined with betel leaf and other ingredients. Tobacco use contributes to 6 million deaths worldwide annually, accounting for 6% of total global mortality. 10 In Bangladesh, hypertension is more prevalent among women and urban populations, with older adults (>60 years) showing a higher incidence compared to younger individuals. 11 Additionally, higher education, obesity, and diabetes increase the risk of hypertension. 12 Approximately 20% of adults and 40%-65% of older adults in Bangladesh suffer from hypertension, 13 and tobacco-related health issues contribute significantly to mortality, 14 with one in every six young adult deaths attributed to tobacco use. 6 Inhalation smoking status is also linked to social determinants such as culture, stress, and income. 4
The tobacco leaf contains a chemical named nicotine. This nicotine is a key factor in the development of hypertension and heart disease. 15 The use of both inhalation and chewing tobacco is associated with adverse cardiovascular effects. 8 Both inhalation and chewing tobacco cause tachycardia, high blood pressure, altered stroke volume, arrhythmias, and coronary blood flow. 16 Chronic tobacco use also leads to arterial stiffness and myocardial infarctions. 17 Chewing tobacco is particularly linked to a sudden increase in hypertension compared to inhalation. 18 Holm et al 19 reported that chewing tobacco enters the bloodstream within 10 min, which rapidly increases the risk of heart disease. Studies have shown that both forms of tobacco use lead to an increased heart rate. 9
The chewing tobacco use can be classified as powdered tobacco, dried tobacco, and sweet tobacco. The inhalation forms can be classified as water pipe tobacco, pipe tobacco, and cigarettes. 20 Understanding which form of tobacco is most harmful to human health is crucial. This study aims to evaluate the association between different routes of tobacco use (chewing, inhalation, or both) and hypertension among rural adults in Bangladesh while considering confounders such as age and betel leaf use, which may influence these associations.
Methods
Sample Size and Study Design
The sample (patients’) number was calculated using the formula S =
Participants’ Selection Criteria
The participants (male and female) who were at least 20 years old have been selected for this study. The participants must be rural citizens of the two assigned districts (Bagerhat and Khulna) of Bangladesh. They must have at least one health issue (e.g., Diabetes, respiratory disease, heart disease, musculoskeletal disorder, digestive system disorder, etc.) and have come to visit a fixed medical specialist in the two assigned clinics. All types of occupations have been considered during participants’ selection. The participants who gave the information willingly have been selected. All rural patients have been considered for this study. A systematic sampling method was used during the study. The first participants were randomly selected to start the systematic sampling after providing sufficient rest, and then every second participant was selected during the doctor’s visit.
Study Location and Time
The study location was the Bagerhat and Khulna districts in Bangladesh. Two clinics were selected in the two sub-district cities from these two districts, where some medical doctors provide services for the remote rural patients. This is a sub-district city’s clinic where the assigned physician visits patients twice a week. The data was collected within 6 months, from November 2023 to April 2024.
Data Collection Tools
Data collection was done through a combined open and closed-ended questionnaire designed for this study. There were three sections. Section A enclosed questions on the basic information of the study. Section B contains demographic information, and Section C is about the habitual facts of the participants. The body weight of the participants was measured by a digital weight scale (Carmy®). The height and blood pressure of the participants were measured by a manual height scale and a manual blood pressure machine (ALPK2®). To make better sense of questions, all questions were asked to participants in the Bengali language. Before data collection, the research assistant was trained in data quality control and data quality assurance.
Variable Definitions
To evaluate the relationship between smoking modes and hypertension status, several key variables were defined. Smoking behavior was categorized to distinguish between various forms of tobacco use. The use of tobacco was defined as smoking (inhalation) and chewing tobacco and categorized as three-level variables (i). Who only smoke (inhalation), (ii). Who only chews, (iii). Who used both inhalation and chewing tobacco, and (iv). Does not use tobacco. Hypertension was defined using Systolic Blood Pressure (SBP) and Diastolic Blood Pressure (DBP) measurements based on the American Heart Association (AHA) definition. 18 Participants’ outcomes were classified as (i). Hypertensive (SBP >130 mmHg and DBP >80 mmHg), (ii). Elevated (SBP 120-129 mmHg and DBP <80 mmHg), and (iii). Normal (SBP <120 and DBP <80 mmHg). 21 Potential confounding variables were selected based on theoretical relevance and prior literature, including age and use of betel leaf (commonly chewed with areca nut, slaked lime, and often tobacco to form “betel quid” or “paan,” widely used in South and Southeast Asia due to its stimulant effects). These factors were included to control variations in hypertension risk that may be independent of tobacco use.
Data Analysis
All the data was analyzed using the SAS-9.4 statistical software. Two types of analysis have been performed for this study. Descriptive statistics and logistic regression were performed to identify the association between the variables. Frequency, percentage, mean average, and standard deviation have been calculated for descriptive statistics. All the continuous variables have been measured by Mean (M) and Standard Deviation (SD). Whereas categorical variables were classified as dichotomous, ordinal, and nominal to be summarized as frequencies and proportions.
Ethical Approval
Before data collection from the participants, the research officer verbally informed the aim, objectives, and benefits of the study. The participants were also informed that personal information would not be revealed. The interviews were conducted by the research officer. The participants gave a sign at the bottom of the questionnaire by mentioning that the above information was given willingly for research purposes. Ethical permission has been taken from the Institutional Ethics Committee (IEC), Sylhet Agricultural University, Bangladesh. The issue number of ethical permissions is #AUP2023017/January 10, 2023.
Results
Demographic and Habitual Data of the Participants
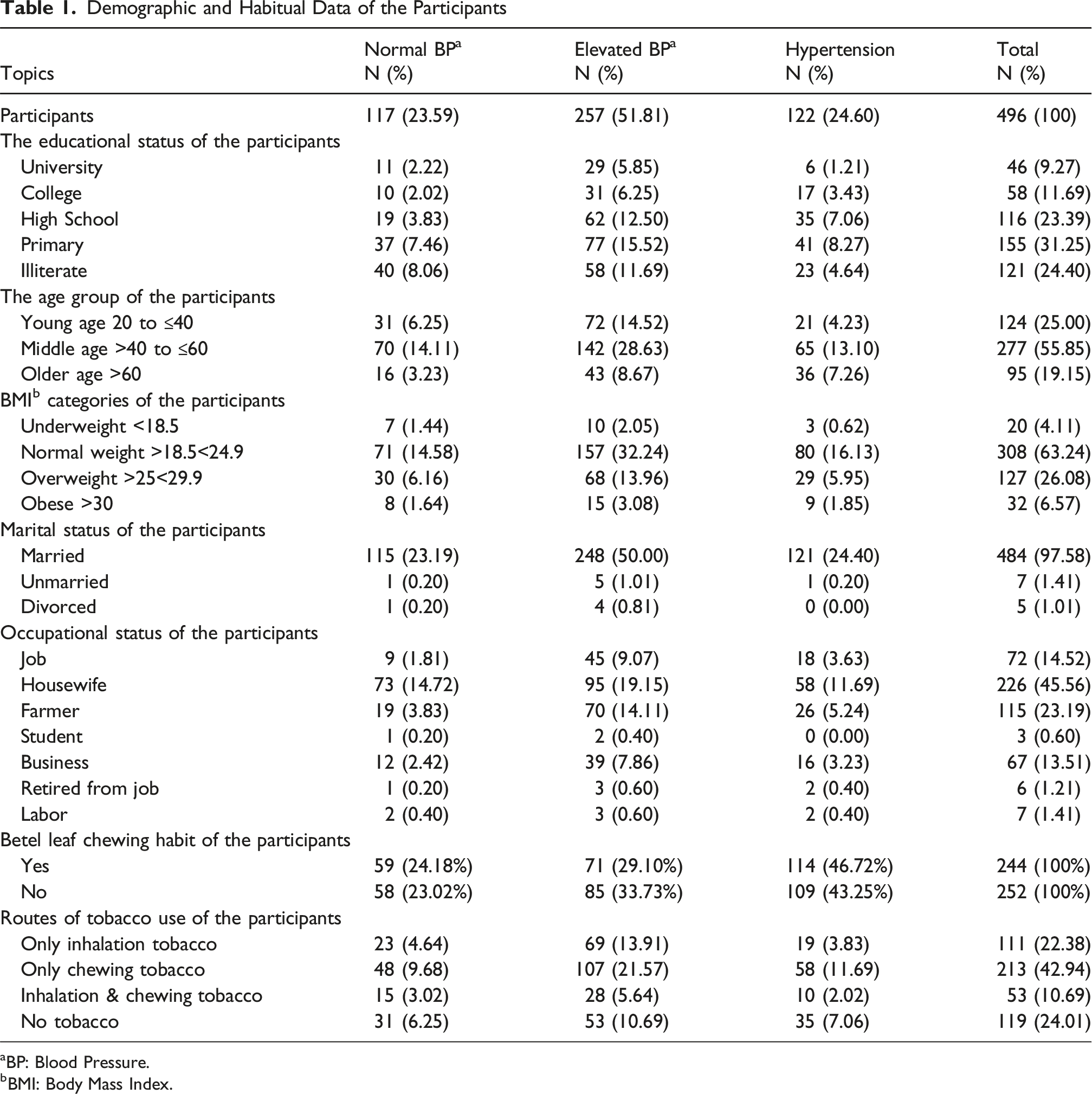
aBP: Blood Pressure.
bBMI: Body Mass Index.
Crude Association Between Routes of Tobacco and Hypertension
Association Between Routes of Tobacco and Hypertension

Effect of Age on Routes of Tobacco and Hypertension
Individuals who smoke regularly are significantly less likely to have hypertension compared to non-smokers (reference group). The odds ratio is 0.16 (95% CI: 0.05-0.55), which means that those who smoke by inhalation have about 84% lower odds of hypertension compared to non-smokers. Chewing vs no smoking: The estimate for those who chew tobacco is close to zero (−0.011) and is not statistically significant (P = .96). The odds ratio of 0.99 (95% CI: 0.61-1.59) indicates no significant difference in the likelihood of hypertension between smokers and non-smokers. Inhalation and chewing compared to non-smokers: The estimate for those who inhale and chew is positive (0.14) but not statistically significant (P = .69). The odds ratio of 1.15 (95% CI: 0.58-2.28) suggests a weak or no association with hypertension.: Age is statistically significant (P = .0001), meaning that age is an independent indicator for the relationship between the routes of tobacco and hypertension. However, applying the 10% rule means that for each additional year of age, the odds of having hypertension increase by 3.2%. The odds ratio for age is 1.03 (95% CI: 1.01-1.05), indicating that older individuals are more likely to have hypertension, controlling for tobacco routes. Age is not an essential covariate in this model (Table 2). Moreover, we studied the age and the mode of interaction on hypertension, and we concluded that age is not an effect modifier of the relationship between the routes of tobacco use and hypertension (chi-square 4.53, P-value = 0.21).
Effect of Betel Leaf on Routes of Tobacco and Hypertension
After adjusting with betel leaf, the crude odds and the adjusted odds of the three routes of tobacco are close to each other. When betel leaf “No” is the reference category, then odd is 0.82 (95% CI: 0.34-1.98) and the P > 0.05 and not statistically significant. So, the betel leaf is not a confounder but an independent predictor (Table 2).
Discussion
Inhalation tobacco also has various forms like cigarettes, biri, waterpipe (hookah), pipe, and hand-rolled cigarettes. 6 Most chewing tobacco is used with betel leaf, betel nut, lime paste, and any non-smoking tobacco. During this study, a total of 496 rural patients who came to visit a doctor were selected. Among these participants, 20.5% reported that they used inhaled tobacco, and 46.4% of participants reported that they used chewing tobacco. According to national and sub-national surveys, Bangladesh has a high prevalence of inhalation and chewing tobacco use. An epidemiological study revealed that the 55-64 age group in Bangladesh had a maximum of 12.3 odds of chewing tobacco. 22 In Bangladesh, rural people have the maximum tendency to use smokeless chewing tobacco rather than inhalation tobacco. 22 According to socio-economic status, educational status, and age group, tobacco use has different patterns. For this study, most participants were housewives, and the second majority group was farmers. The common habitual fact of rural people is to eat betel leaf and betel nut while chewing tobacco during their leisure time.
It is known that chewing and inhalation of tobacco both contribute to increasing blood pressure in the long run. Chewing tobacco has various forms like a dried tobacco leaf, Zarda, Khoinee, Sada Tamak Pata, dark-toned whole tobacco leaf, etc. 6 However, the immediate increase in diastolic blood pressure and mean arterial pressure because of the inhalation of nicotine through cigarette or waterpipe smoking, where nicotine enhances the sympathetic nervous system by releasing epinephrine, norepinephrine, and vasopressin, are well-documented in the literature.23-25 Contradicting findings from previous studies make it hard to agree on the long-term effects of smoking on blood pressure.18,26,27 Moreover, based on a pooled analysis of 89,051 individuals, the adjusted relative risk of those who chew betel leaves compared to non-chewers was 1.2 (P = 1.2). 28 In South and Southeast Asia, betel leaf is frequently chewed with slaked lime, chewing tobacco, and betel nut. 29 In our study, 29.23% of female and 19.96% of male participants had betel leaf chewing habits. The WHO reported that the combined effects of chewing tobacco, betel nut, and betel leaf have a significant association with increasing the risk of hypertension. 26 In our study, the betel leaf did not act as a confounder or effect modifier for hypertension development. There is no evidence that betel leaf acts as an effect modifier or confounder for the association of tobacco and hypertension. Fazal et al 30 revealed that betel leaf acts as an antibacterial, antifungal, larvicidal, antiprotozoal, anticaries, gastroprotective effects, free radical scavenging, antioxidant, anti-inflammatory, hepatoprotective, immunomodulatory, antiulcer, and chemopreventive activities.
Limitations
In our cross-sectional study, the data did not allow us to conclude the association between the mode of smoking and hypertension. However, we cannot establish temporality and causality from this cross-sectional study. We also determined the blood pressure category based on one SBP and DBP reading, which was taken once, disregarding whether the participant had hypertension, whether the participant was on antihypertensive medication, and whether participants were not asked about the last time before the interview they consumed tobacco, all these factors prevent us from drawing a robust conclusion about the impact of mode of smoking and hypertension. There could be a measurement error as manual blood pressure count equipment has been used. Potential confounders, such as dietary habits and genetic predisposition, were not fully explored. Due to resource constraints and a lack of funding, we obtained only one-time BP measurements despite the WHO’s recommendation for multiple readings to confirm a hypertension diagnosis. Additionally, the study did not assess the duration and frequency of tobacco use, which may impact on the observed associations. Future longitudinal studies are needed for more robust findings. We did not calculate the power for the sample size calculation. A non-validated questionnaire has been used during the conduct of this study, and no pilot test has been conducted. As research officers were non-professional so, there could be a little bit of interview bias. All occupations, religions, genders, and ethnicities of Bangladesh were not included in this study, from this study area, so there was a lack of generalizability for this study.
Conclusions
This study underscores the significant public health implications of chewing and inhalation of tobacco in rural Bangladesh. By addressing the cultural, socioeconomic, and healthcare barriers to cessation, policymakers and public health professionals can make meaningful strides in reducing the prevalence of hypertension and its associated cardiovascular disease burden. A comprehensive approach that combines education, policy enforcement, and healthcare integration has the potential to transform tobacco control efforts and improve population health in these underserved communities. These findings should serve as a call to action for national and global stakeholders to prioritize chewing tobacco in their tobacco control agendas, ensuring equitable access to preventive and therapeutic interventions for all.
Supplemental Material
Supplemental Material - Association Between Routes of Tobacco use and Hypertension Among Adult Rural People in Bangladesh: A Cross-Sectional Study
Supplemental Material for Association Between Routes of Tobacco use and Hypertension Among Adult Rural People in Bangladesh: A Cross-Sectional Study by Shobhan Das, Tanmay Mandal, Robert Spurgeon, Md. Hasibur Rahman, Queeneth Edwards, Amenah Qotineh, A.S.M. Mohiuddin, Rezwana Islam Rimi, Md. Mahfujur Rahman, Md. Masudur Rahman and Logan Cowan in Tobacco Use Insights
Footnotes
Acknowledgments
The authors are grateful to clinic owners and managers who cooperated during the conduct of this study. Special thanks to the field research officer, Md. Nazmul Hossain and Md. Sheikh Selim, for their tremendous support for this project.
ORCID iDs
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.