
Abstract
Introduction
Between 70%–85% of people living with schizophrenia currently smoke cigarettes, and among those with bipolar disorder 50%–70% smoke cigarettes. 1 Smokers with SMI smoke more heavily, have more severe withdrawal symptoms, lower quit rates, poorer health, and die about 25 years earlier than smokers without SMI.2-4 Smoking is one of the most important modifiable risk factors for excess morbidity and mortality in adults with SMI. Annually, over 200 000 U.S. adults with SMI die of tobacco-related diseases, accounting for nearly 40% of all annual tobacco attributable deaths. 5 Smokers with SMI spend almost a third of their monthly income on cigarettes. Societal costs include increased health care costs and work force absenteeism. 6 In addition to the benefits of improved physical health due to cessation, evidence suggests quitting smoking leads to decreased levels of depression, anxiety, and stress even in populations with mental health conditions. 7
Many smokers with SMI wish to quit, yet their rates of success are low and evidence-based treatment targeting this group is limited. 8 The gold standard for smoking cessation treatment includes pharmacotherapy (e.g., nicotine replacement therapy) and counseling. 9 People with SMI are often neither offered this type of combination therapy nor asked about their desire to quit smoking. Data indicate that some mental health staff may contribute to continued smoking among people with SMI due to unsubstantiated beliefs that patients may deteriorate without access to cigarettes. 10 Additionally, data show that when people with SMI do attempt to quit, success rates remain low. 8 Multiple psychiatric Associations encourage supports in addition to the standard smoking cessation interventions for people with SMI including tailoring the intervention for patient needs and their condition. 11
Combined treatments can provide these additional supports that help with the multi-level experience of quitting smoking, such as irritability and cravings. Strategies promoting overall health (e.g., exercise) are promising. 3 For example, a Cochrane review 12 of RCTs aimed at increasing physical activity, either alone or in combination with a smoking cessation intervention, 4 studies found an effect in favor of the intervention at the end of treatment.13-16 The effects indicate a positive impact of PA in reducing symptoms such as anxiety and nicotine withdrawal. In addition, we found that a game-based group physical activity (PA) program was an accessible and effective method to improve psychiatric symptoms, increase physical activity, decrease social isolation, and improve health among people with SMI.17,18 Our prior work also showed the importance of in-person support as people with SMI go through the smoking cessation process. 19 We hypothesized that adding a game-based group physical activity program would provide the additional support needed for smoking cessation.
We conducted a pilot two-arm randomized controlled trial (RCT) targeting adults with SMI who were integrated into Our Parks and Recreation (PARQuit) intervention. Our PARQuit intervention included counseling, pharmacotherapy, and 50 minutes active game-based PA groups 3xweek. The control group received counseling, pharmacotherapy, and 50-minute seated, sedentary, game-based groups 3xweek. Thus, the interventions differed only by type of group activity (active vs sedentary). In this paper, we report the results of qualitative interviews conducted with participants upon completion of the program. The purpose of the interviews was to gather participants feedback about the program as well as whether and/or how a sedentary vs active game-based approached differed in their impact on smoking cessation process. Preliminary efficacy of our program is presented elsewhere (paper under review).
Methods
Design
The theoretical framework for our PARQuit intervention is based on a model originally developed by Dr Debra Lieberman, Director of the Health Games Research national program and later refined by an American Heart Association scientific panel and published in a report entitled “The Power of Play: Innovations in Getting Active Summit 2011.” 20 The “Power of Play” theoretical model illustrates ways that active games may improve health behaviors by influencing mediating factors (e.g., PA) that are known to improve health behaviors. We used this model to guide our development and testing of our game-based program. The qualitative component of our study was based on Grounded Theory methodology 21 and is thus informed by symbolic interactionism, a theoretical framework that supports the view that individuals’ understandings occur within the context of relationships. 22 The intervention framework combines well with symbolic interactionism to guide our qualitative inquiry of how participants’ engaged in a group based program.
Researcher Positionality
The PI is a doctorally prepared family nurse practitioner with more than 15 years experience doing research with and providing care for people with serious mental illness. This experience informed the study design and provided the motivation to pursue the development, design, and testing of a smoking cessation program for this population. Her previous and ongoing clinical and research work inform her interpretation of the interviews. She engages in reflexive writing in addition to the theoretical and analytic memos. The PI was trained in grounded theory methodology during their doctoral training and led the interviews and analysis.
Participants and Settings
Inclusion criteria for the RCT were that the participants be at least 18 years of age or older, be diagnosed with a serious mental illness (i.e., schizophrenia, schizoaffective disorder, anxiety disorder) and documented in primary care or psychiatric records, current, daily smokers, willingness to set a quit date, and pass a capacity to consent test based on comprehension of the consent form. Participants were excluded if they had known medical conditions or other physical problems that required special attention to engage in an exercise program (e.g. uncontrolled hypertension, use of nitroglycerin to treat angina). Smoking characteristics were assessed during screening by the project director. In addition, during the initial assessment after informed consent, participants completed a readiness to quit scale. We received 103 referrals, 84 screened for eligibility, 73 were eligible and interested, 48 consented and were randomized to intervention (n = 24) and control groups (n = 24). Twenty (10 from each group) completed the qualitative interview.
Institutional review board approval was obtained from our university’s human subjects committee. Anonymity and confidentiality were maintained according to the guidelines set forth by the Institutional Review Board. Recruitment sites included an urban transitional residential and day treatment center for older adults with severe mental illness and an urban intensive case management program for individuals with serious mental illness. Theoretical sampling among people that completed the program was utilized to ensure maximum variation and build conceptual density of the emerging results. Theoretical sampling is a form of sampling used in grounded theory methodology that entails simultaneous collecting and analyzing data to decide what data to collect next and from how in order to develop theoretical density. 21
Randomization in the PARQuit intervention: After enrollment and baseline data collection, participants were randomized to the intervention or control condition. Randomization assignment cards were generated using a software program written to generate random assignment numbers for two equal groups of 5 in blocks of 10 cards.
Intervention Groups
The intervention was implemented in 5 successive 12-week “waves”. One intervention and one control group were offered simultaneously during each 12-week wave. Before the COVID-19 pandemic, the first wave was conducted indoors, within a transitional residence, using motion-based video games as the PA intervention and seated games for the control group. After public health initiated shutdowns in early 2020, study protocols were adapted and approved by the IRB to safely continue research outdoors without changing intervention procedures or data collection method. These new protocols were used for the last four participant waves. The major differences between the initial cohort and subsequent cohorts were indoor vs outdoor location and availability of specific games.
PARQuit PA Intervention
The PA intervention was introduced to participants 2 weeks prior to their target quit date.
Procedures for the PARQuit PA Groups
Participants engaged in an active game in a group outdoors in a San Francisco public park for 50 min, 3 times a week, for 12 weeks with groups were led by study staff. Each game sessions started with a 10-15 minute warm up (e.g., walking, stretching) and concluded with a 5-minute cool down. Participants were given the option of a variety of games for each session with all participants eventually playing the same games. Game options included: scavenger hunts, lawn bowling, hopscotch, jump rope competitions, spoon and golf ball races, dance competitions, kick ball, soccer, Simon Says with strengthening and flexibility activities, limbo, and timed strengthening and flexibility circuit activities.
PARQuit Control Intervention
Control group participants were introduced to the sedentary games two weeks prior to their target quit date.
Procedures for the PARQuit Control Subsequent Waves
Control group participants played sedentary group games outdoors in a public park for 50 min, 3 times per week, for 12-week with the PI or study staff facilitating the weekly sessions. Participants had a variety of games to try and all participants eventually played the same games. Game options included: Bingo, Guess the Song, Tic tac toe, Pictionary, trivia, charades, paper airplane building & racing, clay building competition, and art-based games.
Pharmacotherapy
After consultation with the principal investigator (PI), participants were provided with a prescription for nicotine replacement therapy (e.g., transdermal patch, gum, and/or lozenges) or Bupropion Sustained Release (SR), detailed information on possible adverse events related to use of NRT and/or bupropion SR, and a schedule for 12 weeks.
The PI followed up with participants at 24 and 48 hours after initiation of pharmacotherapy, to monitor for adverse effects, and also 1 and 2 weeks after initiation of pharmacotherapy.
Smoking Cessation Counseling
Study participants in both control and intervention groups were engaged in the same smoking cessation counseling protocol. We adapted the smoking cessation treatment protocol tested for psychiatric outpatients. 23 The project director provided the counseling intervention, and has experience delivering counseling for intervention studies. Counseling consisted of 8 sessions over 12 weeks. The counseling intervention was based on a cognitive-behavioral framework that focused on enhancing commitment to smoking abstinence, promoting medical adherence, and increasing behavioral skills for achieving and maintaining abstinence.
Qualitative data collection and analysis
Recruitment and data collection began in July 2019 and completed in March 2022. Data were obtained through interviews conducted in one-on-one sessions and participant observation. Interviews were conducted only once and upon completion of the 12-week program. The interviews lasted less than 60 minutes and were conducted with a semi-structured interview guide that was malleable to the responses and emerging themes encountered. A few questions asked were: What did you enjoy most about the game-based smoking cessation program you participated in? What did you enjoy least about the game based physical activity program you participated in? How did the program impact your smoking cessation? Ongoing participant observation was completed during the interview and during the 12-week program.
Consistent with Grounded Theory methodology, data collection and analysis were done simultaneously and used an approach of constant comparison analysis as initially described by Glaser and Strauss 21 and further informed by Charmaz 24 and Clarke. 25 Interviews were transcribed verbatim and then cross referenced to the audio recording for accuracy. Field notes and interview transcriptions were entered into Atlas.ti software to assist with data organization and analyses. The coding process was conducted by two members of the research team. Initial open coding was done with transcript analysis through word-by-word and segment-by-segment coding. Axial and selective coding were implemented to determine key themes and properties in the data and to eventually develop a conceptual framework of codes and categories. Theoretical memos captured the developing conceptualizations about the codes and categories as well as about relationships between categories. Conceptualizations about the categories and relationship between categories were discussed among with the research team. Theoretical and methodological notes were maintained regarding decisions made during the analytic process. Data collection concluded when theoretical saturation was achieved.
Results
Characteristics of Participants.
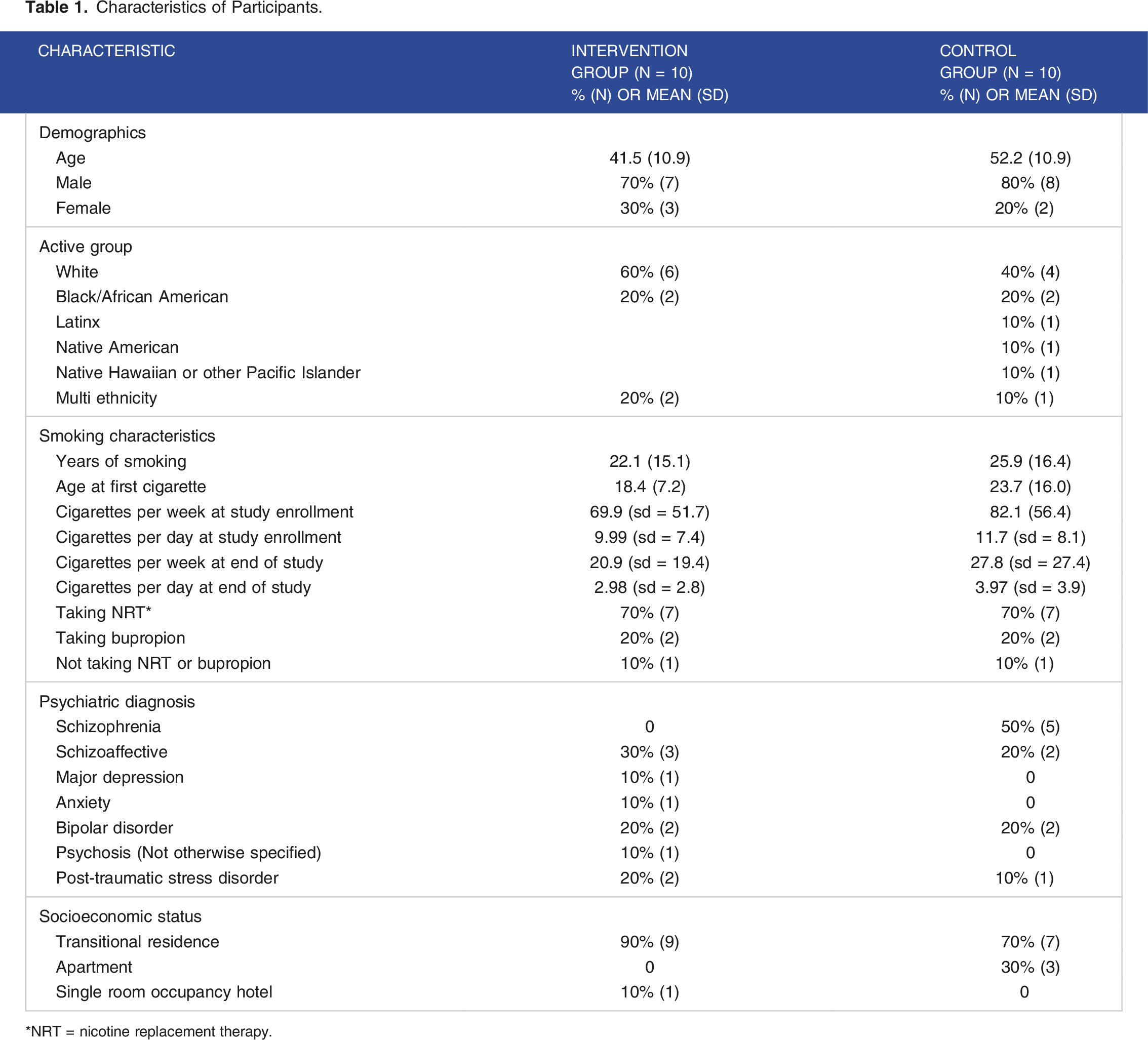
NRT = nicotine replacement therapy.
The average number of game sessions attended was 23.0/36.0 (sd = 7.5) and average number of counseling sessions attended 6.8/8.0 (sd = 2.1). Cigarettes smoked per week decreased significantly over the 12-week program for the 20 participants described in this qualitative report. The change in cigarettes smoked per week from enrollment to week 12 was an average decrease of 51.7 cigarettes (95% bias corrected confidence interval = −77.8 to −28.7). Estimates and inferences were through the use of the nonparametric bootstrap with bias-corrected confidence intervals (BC CI). 26 For non-normal data, this method also has the advantage of providing unbiased estimates without the required assumption of normality for parametric tests. Four participants quit smoking completely by week 12. This change represents a large effect size of .92 (Cohen’s d). 27
Of note, participants in both control (sedentary games) and intervention groups (active games) described how the “whole package” of our intervention helped with their quitting process: group-based games, counseling, and pharmacotherapy. The next section describes the participants perceptions of their experience with each component. The feedback from participants in control and intervention groups were similar so we report the results from both groups combined. We have identified the participant responses as either control or intervention group for clarity.
Whole package themes.

The next section describes the themes within each of the three domains along with factors that modify and contributed to the experiences described.
Arising from discussions of “The Group” were the overlapping themes of Structure (dedicated time and consistency), A Reminder (reinforced goal to quit), A Sense of Belonging (part of a group; peer support/talk to each other); and Commitment (related to sense of belonging, structure and consistency – place to be and stay with the group).
Themes arising from “Counseling” included: Personalization (individualized plan) and Someone to talk to when needed.
Themes arising from “Pharmacotherapy” included: Additional support; It’s subtle; a part of the package.
Factors that further supported engagement included the fact that the group ended up being held outside and included exercise (for the active PA intervention group) which helped make the participants feel good about themselves and supported their commitment to attend. At the same time, factors that created barriers that could influence long term commitment included unstable housing.
The Group
The Group: The presence of the group provided a structure and consistency to a daily schedule. As one active group participant noted, P: I think it's been positive, because having something to do, some structure outside of the house help structure. It gets me out of the house... I mean, you need structure.
Another active group participant noted similarly, P: It's good to have support. Like I smoke way less than I used to. I mean, it's good to have the structure, you know, coming in three times a week and just having a reminder that you're trying to quit smoking. You're not like on your own trying to quit…...having to come here, you know, yeah, it's just a good reminder that you're trying to quit smoking.
This latter quote also emphasized the value of the group in reminding participants of the goal to quit smoking and that they were not alone – they were in this process together. The quote also emphasizes how the group provided a sense of belonging – meeting and interacting with others that one could relate to. As one active group participant noted, “Meeting new people. It's nice meeting everyone.”
This participant went on to note, in response to a question about what they thought about doing all the activities as a group, “Oh, I think it was better to do as a group, for me anyway. It helped me get out – not isolated with myself, so the group is always good.”
The interactions provided support for their efforts to stop smoking, both when in the group and sometimes when not in the group itself. One active group participant specifically emphasized this point when they noted, “You know, it impacted me in a way, because I see cigarettes, for some people it's easy to stop smoking, for some people, it's not. And it impacted me in a kind of way where I see some of the clients who were thriving, you know. I would see we work out. We work out, and at the same time, try to quit smoking. And the emphasis that I see towards other clients, you know, who were pushing, you know, really encouraged my heart a lot, because to see that, you know, and to see that what they were doing.”
By seeing that others were also struggling, pushing to quit, provided encouragement. This encouragement sometimes came from others involved in the group during times the group was not meeting. A control, sedentary activity group participant whose roommate also was involved in the program noted that, “Yeah, that helped a lot. You know, him being in the same room and all that, being in the same study....So, you know, we could converse about it when the group wasn't – when the study wasn't actually taking place, or group wasn't actually in progress. We could converse about it, see?”
While the Group itself was helpful, aspects of the environment and the activities that the group participated in contributed to its positive impact. For example, participants spoke about the value of doing games and being outside. As one control group participant noted, “Well, the games, that's something fun, …. but you got to interact in doing something that I haven't done, you know, especially outdoors, you know, in this type of setting, you know...able to adapt and I enjoyed the moment. I enjoyed it....It fills my time.” Another active group person reflected on the value of engaging in outdoor game-based exercise “being outside, and the exercise and the consistency.” While another active group participant noted, “You had to use energy and be physically fit, and, you know, the games were just fun.”
These quotes suggest that the structure of a program is important but how the time itself, during the structured activity, is spent and where it is spent can facilitate the program’s success. Both the exercise and the games were key to the structured activities success.
Counseling
Counseling: The second component of the “whole package” that people described as critical to their journey was the counseling sessions. Based on the Transtheoretical Model of behavior change, which identifies 6 stages or readiness - precontemplation, contemplation, preparation, action, maintenance, and termination - the counseling sessions were designed with the goal of meeting people wherever they were on their smoking cessation journey. 28 We welcomed people with various levels of readiness to quit.
The stages are exemplified in the following quotes. For example, some participants noted they were motivated and ready to move forward with quitting – “The timing was right on time” – others were at various stages of stopping, as one active group participant noted, “I've tried to quit before. And this time's a little bit different, because I've been able to cut down, so I feel like I've made some progress. Whereas before, I was – I did not cut down and I was smoking the same amount, if not more. So, the progress is causing me to feel like I could actually do this. And the counseling was really helpful this time…”
Counseling included information on reasons people smoke, withdrawal symptoms, specific health risks of smoking and benefits of quitting, how body systems are impacted by smoking, and the financial and personal costs of smoking were provided. Such information did provide a specific rationale for quitting. As one active group participant noted, “just something that is acknowledging my smoking and telling me that it's like, these are the health benefits, these are the health risks, or like and these are the financial consequences of it.”
Another active group participant expanded on this noting, “I’ve said it though a few times after a cigarette, you know, I got to quit smoking. I’ve got to quit smoking. You know, it’s not like I don’t want to quit. It’s like I got to quit smoking, because it’s expensive, and I know it’s going to affect me over time. So it’s not smart to let it get out of hand, because I’m young, you know what I mean? Like because I’m young, somewhat young, like you could look at it like you have a credit card. You know what I mean, you can drink, you can smoke, and it’s not going to hurt you. Well, it can affect you and it can build up over time, you know what I mean? Before you know it, you’ve been drinking for 5 years, or before you know it, you’ve been smoking for 5 years. And time flies. So, I want to nip it in the bud within the next year, okay. It can also affect my mouth, I mean, like my teeth turn yellow, my gums might recede because of the heat from the smoke. So that’s some major stuff…. I hadn’t thought about this stuff before the program.”
Not only did participants learn about tools that they could use to help them quit, but also how to tailor these tools and develop unique strategies. This was one of the strengths of the counseling sessions – the development of individualized ‘quit plans’.
As an active group participant stated, “I tried to quit smoking before and I quit for three or four days. But I would be right back at it. The thing is, the tools that I learned, since I've been in this class, is the reason that I don't smoke no more.
The utility of a plan was further emphasized by an active group participant who noted, “Because it's always there for me. When (the facilitator) told me to write something down, then I think it helps me, or if I hear something, you or your co-workers tell me, then I write it down, and then I have it to read if I'm having doubts, or if I'm thinking that I can't do this. I can read and say, well, this is what I did before, so I can do this again. Or this is what I did on week four, and then it allows me to see, not only to think about it, but to see the things that help me. And I can read them and go over them and it keeps in your mind, and it keeps in your body, that this is what helped me and this is why I'm quitting smoking…I look at it mostly every night, because I have other people around me that smoke.”
Alternative strategies for smoking often incorporated relaxation techniques that helped ameliorate anxiety and tension. For example, one control group participant described being mindful and focusing on the breath. I: What did you find was the most helpful thing for helping you to not pick up a cigarette? P: For me, I tell myself and think about do I want it, you know...But I've learned to stop and tell myself....stay with the moment, inhale and exhale.
Components of the program that supported these counseling sessions included the presence of others who were also trying to quit but especially the researchers/ counselors themselves. As participants noted, Control group P: The fact that staff were so approachable, from the beginning, it was like a circle of trust. We were literally having fun sometimes I didn’t even think I was in a program. It made the connection and acceptance of the program. Active group P: Well, I had [researchers] to talk to, and then I had the other participants, which made it really easy, yeah. Control group P: Well, you just gave encouragement… giving us the incentive to stay strong and work towards the addictive behavior that we have with smoking. You were…positive
Pharmacotherapy
The third component of the “whole package” was Pharmacotherapy to help with smoking cessation. We coordinated with participants’ clinicians (behavioral health or primary care) to assure they had a prescription for a medication to help with quitting tobacco use. Participants were provided information from the PI about the different options including bupropion SR and/or nicotine replacement therapy in the form of a transdermal patch, gum, or lozenge. The effects of this component were much more subtle than the other components, partly because most participants were already on a number of medications, and it was more difficult to delineate the specific impact of the medication over and above the rest of the program. One active group participant noted, “I don't really know about the medication. I was taking it every day, but I don't know if it was the medication, or the tools. I think it was more of the tools, but I can't really say, because I was taking other medications, too, at the same time. So, I really don't know about what I can say about the medication part.” Another control group participant was more direct, noting, “I don't know. No, it didn't do anything, I don't think. I didn't notice anything with the Bupropion.” However, another active group participant could see the benefit noting, “That [the patch] helped. That helped a lot. Because with the patch and I don't think I'd be able to quit if – I think I'd still be smoking half a pack a day...”
Still others needed to be reminded that medications were another strategy they could use as part of their quitting process. A control group participant indicated: “I didn't even chew the gum yet. I haven't even need it. You know what? If I chewed the gum, I could probably stop smoking altogether I bet. I should try that. Maybe I'll try that tomorrow. I'll start with the gum. Yeah, if I chewed the gum, I could probably stop smoking altogether, because I only smoke a couple times a day anyway. I could chew a piece of gum now.”
Discussion
This study is the first to our knowledge to evaluate the combination of group-based PA, counseling and pharmacotherapy for people with SMI. Participants described the importance of the structure of our multi-component intervention for their smoking cessation journey. The results from our work suggest the perceived importance of intensive cessation support services for people with SMI that include multiple visits per week, peer-based support, and the integration of games in an outdoor environment.
29 Our adaptation to shift to the parks to minimize COVID-19 transmission provided more benefits beyond COVID mitigation.
For the general population of adult smokers, physical activity is a critical additional component of smoking cessation programs, and helps to buffer psychological withdrawal symptoms and reduce cravings. 12 Two studies13,14 documented that adding PA to smoking cessation strategies may benefit people experiencing depression and anxiety. Our qualitative findings suggest that PA is an acceptable and possibly beneficial component of smoking cessation interventions in a population experiencing serious psychiatric symptoms.
Park-based physical activity programs are accessible and may improve mental and physical health.30-32 A systematic review of 11 studies evaluating the effects of outdoor PA initiatives vs those conducted indoors, 9 studies showed improvement in mental well-being in outdoor PA. 31 Urban parks have been identified as key environmental sites that can provide people with a variety of active recreation options in a free and accessible location.30,32,33 Our PARQuit intervention harnesses these benefits of accessible and engaging park-based PA for smoking cessation and improved mental health.
A growing body of work suggests that cutting back, gradually reducing the number of cigarettes smoked with an ultimate goal of cessation, is an effective strategy. 34 This approach, called the “cutting back to quit” program, may work well for people that are not ready for an abrupt quit date. A qualitative evaluation of a program that employed the cutting back to quit approach highlighted some of the reasons participants found this approach worked and included: 1. Time and flexibility of going at their own pace; 2. The trust and empathic relationship built with their provider during the process; 3. Setting progressive goals; 4. Experimenting with different pharmacotherapies to assist with the process; and 5. On-going contact with the clinicians. 34 Participants in our program that utilized the cutting back to quit approach provided us with similar feedback about why this approach worked. The frequent sessions per week over a 3-month period also provided an ideal platform for this cutting back to quit approach.
Consistent with current guidelines for smoking cessation, 35 participants described the combination of counseling with pharmacotherapy as a helpful part of their cessation journey. These results emphasize the importance of combining treatments that help with the multi-level experience of quitting smoking, such as cessation concerns (e.g., irritability and cravings), indicate strategies to promote overall health (e.g., exercise) is a promising approach. People talked about how the NRT played a role in their cessation attempt and may need reminders to use the NRT to help with the cessation process. The data indicate that NRT, bupropion, and varenicline are superior to placebo and are well tolerated among people with SMI. 36 Lubitz et al 29 found in their survey of 482 people with SMI that among those that made a quit attempt in the previous year (44%), 61% reported using a cessation medication while only 13% utilized counseling. Our data suggest that combination treatments that include counseling, pharmacotherapy, and peer-based support are acceptable among SMI smokers and perceived as beneficial. Settings that offer services to consumers with SMI need to consider ways to provide these types of combination treatments.
Our study used a similar combined counseling and pharmacotherapy approach as the Smoking Cessation Intervention for Severe Mental Illness trial (SCIMITAR+). 37 In the SCIMITAR + trial, participants in the intervention group were offered a smoking cessation intervention by a trained mental health counseling cessation practitioner, typically an experienced mental health nurse. The structured counseling intervention was adapted for people with SMI to include offering NRT before the quit date, making several assessments prior to the quit date, offering home visits as well as face to face support after a relapse or unsuccessful quit attempt, and informing the participants’ primary care or psychiatric care provider about quit attempts. Our approach is similar in that we offered NRT prior to the quit date, maintained contact with participants’ providers, and offered multiple counseling sessions prior to the quit date along with ongoing face to face supports throughout the process. We differ in that we trained a staff member to provide the counseling yet an experienced mental health nurse maintained oversight of the protocol and was also in frequent contact with participants. The most marked differences between our studies are that our program was offered in group-based settings that allowed for peer-support and we also offered game-based physical (for the intervention group) or seated activities (for the control). The results from our qualitative evaluation indicate participants found our program engaging and accessible.
Limitations to our study include implementation in routine care may be problematic due to the staffing resources needed to run the program that might not be readily available in mental health programs. Future work will include evaluating the cost effectiveness of the program and sustainability outside research settings.
In conclusion, we developed a game-based program to further support the evidence-based strategies that may not only aid with quit attempts and cravings but can also allow for the development of additional health enhancing behaviors. Further, our findings suggest that the game-based program is engaging whether it is active or sedentary. What is central is that participation in a group-based, accessible, and engaging smoking cessation program incentivizes participants to focus on their health and reduces the tobacco industry’s influence on their lives. In addition, participants learn the skills to stay quit with a program that could be adapted for implementation across mental health treatment settings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Tobacco-Related Disease Research Program; TRDRP Grant #: T29IP0235 and T32IR4673.