
Abstract
Given the potential respiratory health risks, the association of COVID infection and the use of combustible cigarettes, electronic nicotine delivery systems (ENDS), and concurrent dual use is a priority for public health. Many published reports have not accounted for known covarying factors. This study sought to calculate adjusted odds ratios for self-reported COVID infection and disease severity as a function of smoking and ENDS use, while accounting for factors known to influence COVID infection and disease severity (i.e., age, sex, race and ethnicity, socioeconomic status and educational attainment, rural or urban environment, self-reported diabetes, COPD, coronary heart disease, and obesity status). Data from the 2021 U.S. National Health Interview Survey, a cross-sectional questionnaire design, were used to calculate both unadjusted and adjusted odds ratios for self-reported COVID infection and severity of symptoms. Results indicate that combustible cigarette use is associated with a lower likelihood of self-reported COVID infection relative to non-use of tobacco products (AOR = .64; 95% CI [.55, .74]), whereas ENDS use is associated with a higher likelihood of self-reported COVID infection (AOR = 1.30; 95% CI [1.04, 1.63]). There was no significant difference in COVID infection among dual users (ENDS and combustible use) when compared with non-users. Adjusting for covarying factors did not substantially change the results. There were no significant differences in COVID disease severity between those of varying smoking status. Future research should examine the relationship between smoking status and COVID infection and disease severity utilizing longitudinal study designs and non-self-report measures of smoking status (e.g., the biomarker cotinine), COVID infection (e.g., positive tests), and disease severity (e.g., hospitalizations, ventilator assistance, mortality, and ongoing symptoms of long COVID).
Keywords
Introduction
The use of combustible cigarettes and electronic nicotine device systems (ENDS; also known as vapes or e-cigarettes) has been associated with acute and chronic adverse respiratory illnesses which may exacerbate COVID infection or severity.1–3 Epidemiological studies demonstrate significant associations between combustible cigarette use and viral respiratory diseases (e.g., H1N1, influenza),4,5 bacterial pneumonia,4,6 chronic obstructive pulmonary disease (COPD), 7 and lung cancer. 8 Adverse respiratory tract health effects from use of ENDS are suspected due to glycol and glycerol vapors, which are associated with upper respiratory system irritation and inflammation, 9 which are increased in ENDS users. 10 Resulting inflammation are known to increase susceptibility to infection. 11 Indeed, inflammatory responses from ENDS use are greater than combustible cigarette smoke. 12 Dual use of both combustible cigarettes and ENDS may be particularly concerning for respiratory health.1–3 Compared to combustible cigarette use alone, dual use of combustible cigarettes and ENDS has been associated with greater respiratory symptomology and diagnoses (e.g., breathing difficulties, 13 increased risk of asthma and COPD 14 ) than combustible cigarette use alone. Given the respiratory health risks of combustible cigarettes, ENDS, and concurrent dual use of both, examining use associated with COVID infection and severity is a key concern for public health. 1
Combustible cigarette use and COVID-19 susceptibility and severity
Findings from studies of the association between combustible cigarette use and ENDS use, and COVID-related risks have changed by study design over the course of the pandemic. Initial findings suggested that combustible cigarette use was associated with lower rates of COVID infection among hospitalized patients 15 as well as those in primary care settings. 16 Subsequent meta-analyses, however, demonstrated an association between combustible cigarette use and increased severity of COVID symptoms and outcomes, including hospitalization and need for ventilation.17,18 Individuals who used combustible cigarettes were twice as likely to experience severe or critical COVID as former or never-smokers. 18 Currently, therefore, combustible cigarette use is a known risk factor for the development of severe COVID symptoms and outcomes.
ENDS use, dual use, and COVID-19 susceptibility and severity
Preliminary evidence suggests an increased risk of COVID infection and disease severity among those who use ENDS. 19 ENDS use has been shown to increase the prevalence of COVID cases and COVID mortality. 20 One study of youth determined that COVID diagnosis was 5 times more likely among ever users of ENDS only, 7 times more likely among ever dual users of ENDs and combustible cigarettes, and 6.8 times more likely among past-30-days dual users compared with those who had never used ENDS. 21 ENDS use was also shown to increase the risk for hospitalization from COVID. 21 Dual users of combustible cigarettes and ENDS were found to be the most likely to report COVID infection and COVID related symptoms. 22
While many studies have quantified the risk of COVID infection and severity associated with combustible cigarettes, ENDS, and dual use, many studies and meta-analyses that have been published report unadjusted odds ratios.23-27 Clinical comorbidities such as hypertension,17,28 cardiovascular diseases, 17,29 diabetes mellitus,17,30 chronic obstructive pulmonary disease (COPD),17,31,32 and obesity;17,33,34 as well as sociodemographic factors including age,35,36 sex,35,37,38 race and ethnicity,39-42 socioeconomic status and educational attainment, 43 and rural and urban environmental factors,44-46 have been shown to influence both infection and severity of COVID. Given the potential for these variables to also differ as a function of smoking/ENDS use, previous studies reporting unadjusted odds ratios for the risk of COVID infection and severity by nicotine use may provide misleading estimates of risk. It is imperative to control for known clinical comorbidities and sociodemographic factors that may differentially impact COVID infection and severity in the U.S. to isolate the effects of smoking status.
Methods
Participants
We utilized data from the cross-sectional 2021 U.S. National Health Interview Survey (NHIS) 47 to assess COVID infection and severity among individuals who use combustible cigarettes, ENDS products, and dual use of both, while accounting for clinical and demographic influences. The NHIS is an annual survey, funded and conducted through the Centers for Disease Prevention and Control. NHIS participants include non-institutionalized adults aged 18 or older from all 50 states of the U.S. and the District of Columbia. The survey is conducted using a complex sampling design and is weighted to be representative of the residents of the United States, which includes oversampling of minority groups. Data were collected January 2021 through December of 2021, therefore, this manuscript is largely in consideration of the dominant circulation of Delta and Omicron COVID-19 variants. In the U.S., the Delta variant was first identified in March 2021. 48 Thereafter, Delta became the predominant variant in the U.S. and caused a wave of new infections, especially in the Southeastern U.S. in places where community vaccination rates were low. 48 The Delta variant is highly infectious, and it is estimated to be about 60% more transmissible than the Alpha variant. 48 In unvaccinated patients, the Delta variant potentially causes more severe sickness than previous variants.49,50 This is of concern because vaccine hesitancy is common among current tobacco users, 51 and the prevalence of vaccine hesitancy has been shown to be significantly higher among young adults who were current smokers (including ENDS), when compared to non-current smokers (36% vs 22%). 52 Further, the Omicron variant was reported in the U.S. in November 2021, and the rate of infection was estimated to be 100 times greater than the previous Delta variant. 53 Therefore, examining the relationship between smoking status and COVID-19 susceptibility and severity during the height of the Delta wave and the beginning of the Omicron wave is of high importance.
COVID infection and severity
All COVID data were self-reported. Individuals were coded as having COVID infection if they reported that they had COVID or a positive COVID test. Participants reported severity of COVID symptoms as none, ‘mild,’ ‘moderate,’ or ‘severe.’ Respondents who refused or responded as ‘don’t know’ were excluded from the analysis.
Combustible cigarette, ENDs, and dual use
Combustible cigarette use was coded as a binary variable from the question “Do you NOW smoke cigarettes every day, some days, or not at all?” Those responding as “every day” or “some days” were classified as current smokers. A parallel question was asked to determine ENDS use: “Do you NOW use e-cigarettes or other electronic vaping products every day, some days, or not at all?” Similar coding applied to ENDS. Use variables were then combined to create a single variable for analysis representing non-use, cigarette use only, ENDS use only, and concurrent cigarette and ENDS use.
Sociodemographic and clinical characteristics
Demographic variables extracted from the dataset included age, sex, race/ethnicity, education, U.S. census region (e.g., South, Northeast, Midwest, West), and urbanicity (as defined by the 2013 National Center for Health Statistics Urban-Rural Classification Scheme for Counties). Race/ethnicity was analyzed using the NHIS coding which identifies Hispanic or non-Hispanic origin. The ‘American Indian/Alaskan Native only’ and ‘American Indian/Alaskan Native-’ with ‘-any other group’ were collapsed together into a single AIAN category. We relabeled the ‘Other single and multiple races’ as ‘Race not listed’. Education was recoded into 4 groups— ‘less than high school completion,’ ‘high school graduate or equivalent,’ ‘some college,’ or ‘completed technical or college degree.’ Urbanicity was recoded as either ‘metro’ or ‘non-metro.’ To control for co- or multi-morbidities that have been associated with severity of COVID symptoms, variables of self-reported diabetes, COPD, coronary heart disease, and obesity status were extracted from NHIS and coded as binary variables.
Statistical analysis
We report the sample (n) demographics, combustible cigarette, ENDS, and dual use prevalence, and reported COVID infection and disease severity. Next, logistic regression models were utilized to determine the likelihood of COVID infection, via odds ratios (OR) and adjusted odds ratios (AOR), between individuals who use nicotine products (by category) and those who do not. Lastly, chi-square tests were utilized to determine associations between combustible cigarettes, ENDS, and dual use status and reported severity of COVID symptoms. Statistical analyses were performed using Stata 16.1 (StataCorp LLC., College Station, TX) using sampling weights, provided by the NHIS. This project was submitted for ethics review and determined to be non-human subject research as defined in 45 CFR 46.102(d) and (f).
Results
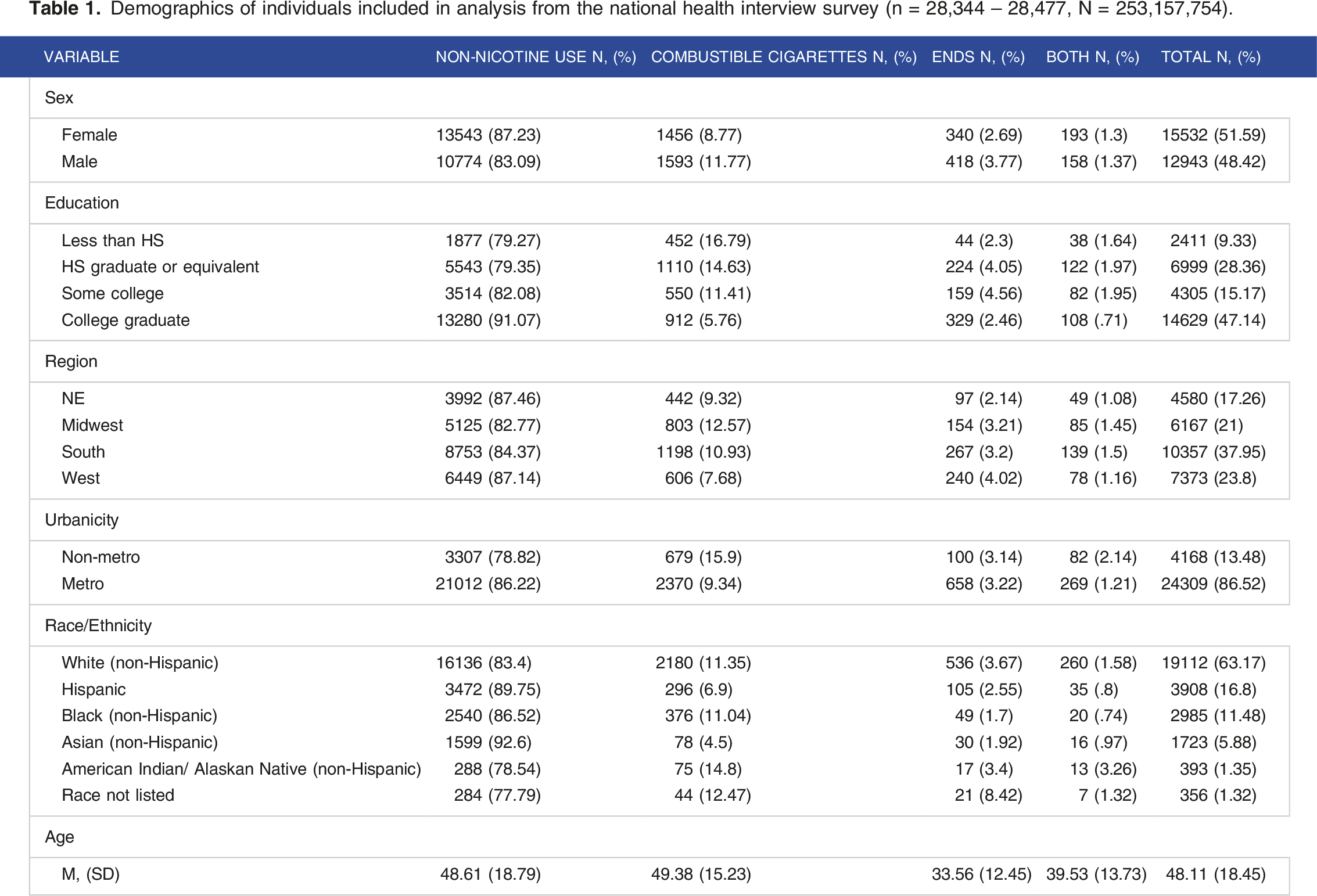
Participant characteristics
Demographics of individuals included in analysis from the national health interview survey (n = 28,344 – 28,477, N = 253,157,754).
COVID infection and severity and combustible cigarette, ENDs, and dual use
Prevalence and associations of COVID19-infection by nicotine status and type.

Adjusted model controlled for sex, race/ethnicity, region, urbanicity, education, age, and comorbidities of diabetes, COPD, coronary heart disease or had a heart attack, and obesity status.
Prevalence and associations of COVID severity by nicotine status and type.

Discussion
This study aimed to examine COVID infection odds ratios for combustible cigarette, ENDS, and dual use as well as adjusted odds ratios controlling for confounding factors that may impact infection and severity of COVID infections in the U.S. Controlling for sex, race, region, education, urbanicity, age and comorbidities, when compared with those who do not smoke, combustible cigarette use is associated with a lower likelihood, whereas ENDS use is associated with a higher likelihood of self-reported COVID infection. There were no significant differences in self-reported COVID infection between non-users and dual users, and no significant differences in self-reported COVID infection severity were identified between individuals who did not use nicotine products, those who use combustible cigarettes, those who use ENDS, and those who engage in dual use.
Combustible cigarette use and self-reported COVID infection
Our findings are consistent with other studies that found that combustible cigarette use is associated with lower likelihood of COVID infection15,16,54 when compared with individuals who did not use nicotine products. Combustible cigarette use has been shown to increase likelihood of infection by other respiratory infections,5,55 because combustible cigarette use leads to structural changes in the respiratory tract and a reduced respiratory immune response. 56 However, in the case of COVID, reduced respiratory immune response may be implicated in lower self-reported infection rates; recent findings suggest that monocytes become infected with SARS-CoV-2 and are responsible for triggering the inflammatory response associated with most severe COVID symptoms. 57 Therefore, speculatively, a reduced respiratory immune response stemming from combustible cigarette use may aid in reducing the likelihood of COVID infection as a result of reduced monocyte viability following exposure to combustible cigarettes. Nonetheless, it must be stressed that the negative health effects of combustible cigarette use far outweigh any potential benefit in COVID infection.
Importantly, other behavioral, environmental, and health-related considerations may help explain the current findings. The hand-to-mouth behavior associated with use of both combustible cigarettes and ENDS products may contribute to increased transmission of bacterial and viral respiratory illnesses. 58 However, behaviors associated with combustible smoking and ENDS use also include environmental factors that may also protect against COVID transmission (e.g., use in outdoor environments, staying 6 feet away from others in designated outdoor smoking areas, etc.). Finally, individuals who regularly use combustible cigarettes are more likely to report upper respiratory infection symptoms such as coughing, runny nose, and sore throat, 59 and therefore, may under report symptoms associated with infection and be less likely to test for COVID.
ENDS (electronic nicotine delivery system), dual use, and self-reported COVID infection
Findings suggest that ENDS use is associated with higher self-reported COVID infection compared to non-users, but we did not find an association in dual users. This may indicate that environmental protections for combustible cigarette users did not protect ENDS users from COVID infection, given there are fewer regulations concerning the public use of ENDS than with combustible cigarette use in the U.S., allowing them to be used more often in restaurants, worksites, and bars. 60 Thus, individuals using ENDS are not as likely to be engaging in isolated or outdoor smoking behaviors (as would be those using combustible cigarettes). Partially supporting this hypothesis, one study found that compliance of social distancing behaviors were the lowest for individuals who were currently using combustible and ENDS in the United Kingdom. 22 Further, sharing behaviors of ENDS may also contribute to increased COVID infection. In one sample of U.S. college students, 24% reported sharing ENDS daily, whereas 76% reported sharing ENDS on some days. 61 Therefore, sharing behavior of ENDS may also contribute to the increased COVID infection rates. Alternatively, this may be an artifact of a small sample of individuals using ENDS or reporting dual use that also reported COVID infection (n = 44).
Associations between nicotine products and self-reported COVID severity
Self-reported COVID severity (asymptomatic, mild, moderate, severe) did not vary significantly by nicotine product. These findings do not corroborate recent meta-analytic evidence that current smoking status is associated with severe COVID symptoms.25,36,62 However, our results corroborate findings from another meta-analysis showing that smoking status is not associated with COVID disease severity. 23 While disease severity measurement was highly heterogeneous between these meta-analyses and the current study, disease severity measurement does not reflect parallel measures of severity, making comparisons between studies flawed. Disease severity in our study was solely based on self-reported severity, and respondents may have interpreted levels of disease severity differently, based on their own subjective experience. Further, smoking status measurement in the current study did not reflect the intensity or frequency of use. Therefore, while our study did not find an association between self-reported COVID disease severity and nicotine status/product type, these factors should be considered as results may not be reflective of actual COVID disease severity outcomes.
Strengths, limitations, future directions
Strengths of the current study include utilizing data from the 2021 National Health Interview Survey, which utilizes complex survey design and oversampling of under-represented populations and is, therefore, representative of United States residents. While many studies that have been published were not representative in terms of the sample population, this study may be more generalizable to the U.S. population than other studies based on smaller samples with regional limitations. Further, utilizing odds ratios as well as adjusted odds ratios to control for many possible confounding sociodemographic and clinical characteristics is a major strength of this study, as known sociodemographic and clinical factors have been shown to influence both infection and severity of COVID disease, including age,35,36 sex,35,37,38 race and ethnicity,39-42 socioeconomic status and educational attainment, 43 rural and urban environmental factors,44-46 cardiovascular diseases,17,29 diabetes mellitus,17,30 chronic obstructive pulmonary disease (COPD),17,31,32 and obesity;17,33,34. While this study accounted for these factors, it demonstrates that these relationships exist even after accounting for these covarying factors.
This study is limited by the cross-sectional study design. With the current data we are not able to assess the temporal relationship between nicotine use and self-reported COVID infection and severity. The study design precludes examination of whether nicotine use causes one to be more susceptible COVID infection or developing more severe symptoms as direct result of smoking status, limiting the overall implications of the study. Further, like many other published studies that examine the relationship between COVID infection, severity, and nicotine use, this study is reliant on self-reported measures. Self-report measures of smoking status have been shown to underestimate smoking prevalence (24.7%) when compared with blood cotinine levels (36.1%). 63 Further, the low prevalence of adult ENDS use in the U.S. is also a notable limitation in the current study. This is reflected in a relatively small number of ENDs users and dual users in the current sample that may have reduced study power and led to error. Finally, these data were collected in the U.S., with wide variations in public health protections by state, and therefore, findings may not generalize to other populations.
Future studies should utilize longitudinal study designs to examine temporal relations between COVID infection, severity, and nicotine use. Future studies should compare a larger sample of ENDs and dual users with combustible cigarette users and non-smokers than was possible in this NHIS based study. Further, since each wave of COVID variants has had different impacts on both infectiousness and severity of disease (e.g., the omicron variant had higher infectiousness rates but lower rates of disease severity than other variants), 64 examining how smoking status impacts COVID infection and severity within new variant peaks may help disentangle risks for infection and development of severe disease. One important factor to consider and measure is the amount of combustible cigarette, ENDS, and dual usage. Measurement of the biomarker cotinine may help circumvent issues with social desirability biases and allow direct measurement of nicotine consumption. Also, capturing frequency and dose of nicotine consumed, as well as behaviors around use would clarify risk for infection with COVID. Future studies should also consider the enhanced measurement of COVID infection and symptom severity.
Conclusion
As the waves of the pandemic become more common and face a less coordinated public health response, examining potential risk and influencing factors associated with COVID infection and severity is of great importance to individual and public health. Results from this study show that combustible cigarette use is not associated with a higher likelihood of self-reported COVID infection when compared with those who do not smoke in the current sample. Moreover, after controlling for sex, race, region, education, urbanicity, age, and clinical comorbidities the overall results did not change substantially. There were no significant differences in self-reported COVID severity between individuals who do not use nicotine products, those who use combustible cigarettes, those who use ENDS, and those who engage in dual use. Although our findings suggest that combustible cigarette use did not impact the likelihood of having a COVID infection, the negative health effects of combustible cigarette use far outweigh any potential benefits identified in this study. Since combustible cigarette use is a known risk factor for other respiratory infections, it is imperative to accurately predict and quantify the risks associated with smoking status as new variants of COVID emerge to mitigate the impact on individual and population health.
Footnotes
Author Contributions
MH had full access to all data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: JMC, SAM, MH; Acquisition, analysis, or interpretation of data: MH; Drafting of the manuscript: SAM, MH, ALC, JMC, BG; Critical revision of the manuscript for important intellectual content: SAM, JAO, JMC, BG; Statistical analysis: MH.; Obtained funding: MH, JMC; Administrative, technical, or material support: JMC; Study supervision: MH.
DECLARATION OF CONFLICTING INTERESTS
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Hartwell receives research support through the National Institutes for Justice and the Health Resources Services Administration unrelated to the current work. Dr. Croff receives funding from the National Institutes for Health, Health Resources Services Administration, and the Substance Abuse and Mental Health Services Administration. Dr. Oliver receives funding from the National Institutes for Health and the Brain & Behavior Research Foundation.
FUNDING
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by the National Institute of Drug Abuse (U01DA055349, Julie Croff, PI; K23 DA042898, Jason Oliver PI), the National Institute of General Medical Sciences of the National Institutes of Health (2P20GM109097; Jennifer Hays-Grudo, PI), the Health Resources Services Administration (U4AMC44250-01-02, Audra Haney, PI), and the Oklahoma Tobacco Settlement Endowment Trust (TSET; R21-02). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health, the Health Resources Services Administration, or the Oklahoma Tobacco Settlement Endowment Trust.
Ethical Approval
This study was determined to be non-human subjects research by the Oklahoma State University Institutional Review Board. This study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.