
Abstract
Background:
Smoking is a leading cause of preventable deaths. Smoking cessation can reduce the risk of smoking-associated disease and death. But smoking cessation involves behaviour change. Existing research indicates that health-information seeking and health-promoting behaviours can be positively associated. However, in the context of smoking, the relationship between seeking health information and intending to quit smoking remains only partially understood.
Aim:
This study aimed to examine the relationship between seeking health information and intending to quit smoking and to determine whether this relationship is mediated by health beliefs.
Methods:
We used data from the fourth cycle of the US National Cancer Institute’s Health Information National Trends Survey (HINTS). Logistic regression was used to assess the independent variable (ie, health-information seeking) and dependent variable (ie, intention to quit smoking) as mediated by health belief.
Results:
Our findings suggest that smokers who seek health information have a 2.67 times higher odds of intending to quit smoking than smokers who do not seek health information. However, health beliefs do not have an intervening effect between seeking health information and intending to quit smoking.
Discussion:
Seeking health information is important in predicting attempts to quit smoking, regardless of the smokers’ pre-existing health beliefs. Our findings support cessation efforts that encourage smokers to seek health information. Determining optimal ways to encourage smokers to seek smoking-related information could support achieving and maintaining smoking cessation.
Conclusion:
Cessation programmes and policies should encourage smokers to seek health information. Additional research should further examine smokers’ motivators and cues for health-information seeking and should further probe smokers’ beliefs about the risks of smoking.
Introduction
In 2014, the US Department of Health and Human Services, estimated that more than 480 000 deaths in the United States are smoking related (2014), making smoking one of the leading causes of preventable disease and death.1,2 The World Health Organization 3 recognizes smoking as a severe global public health threat. Smoking increases the likelihood of cancer, heart disease, stroke, lung disease, diabetes, and chronic obstructive pulmonary disease, all of which result in potentially avoidable health care expenditures and productivity losses. 1 Risks of disease and mortality from smoking could be avoided if individuals did not initiate or quit smoking.4,5 Although rates of smoking have decreased significantly, approximately 18% of Americans still smoke, and more than 1 billion people smoke globally. 6
Factors associated with smoking and intention to quit include personal health attitudes and beliefs, perceptions of risk, psychological states, as well as socioeconomic, demographic, cultural, and other societal factors.2,7-9 Smokers tend to perceive fewer health risks of smoking compared with nonsmokers.10-12 For example, when compared with former smokers, smokers were less likely to believe that smoking causes heart disease, lung cancer, stroke, and other health problems. 12 Studies have found that increasing perceived risks of smoking may not always deter smoking but health beliefs and levels of health-related knowledge have been associated with decreases in smoking.13,14
Extant research explores various predictors of intention to quit smoking, including psychological readiness, attitudes, motivation, family support, social behaviour, smoking history, and mental health.15,16 Furthermore, research indicates that individuals who actively seek health information can improve their ability to make informed decisions; engage more readily in change behaviour; and improve the likelihood of being healthy.17-20 Seeking health information has been associated with various outcomes important to health, including changes in cognition, behaviour, and affect. 21 More specifically, seeking health information can impact decisions about engaging in health-promoting behaviours; it affects what information is available ‘on which the judgements, beliefs, and attitudes towards the health behaviour are based’. 21 However, despite the apparent connections between individuals’ health-information seeking and their health beliefs, the specific relationship between seeking health information and intention to quit smoking is not fully understood. Still unclear is whether health-information seeking among smokers is associated with an intention to quit. Therefore, the purpose of this study is to help fill this gap by examining the relationship between health-information seeking and intention to quit smoking and whether health beliefs play an intermediary role.
Background
Health-information seeking
Health-information seeking is critical to health. It is defined as intentional and active efforts to obtain specific information regarding a health issue.22,23 Notably, seeking health information may be an avenue to better-informed decisions and health-maximizing behaviours.17,18 Such health-information seeking can include Internet searches, discussions with healthcare providers, and calling hotlines regarding a health-related topic. 18 Low levels of health-information seeking have been associated with negative health outcomes, including delays in diagnosis and treatment of illnesses and continued unhealthy behaviours. 24
Seeking health information is particularly important to behaviour change. Studies find positive associations between individuals who actively seek health-related information and those who engage in ‘health-conscious’ behaviours.25,26 Health-information seeking can also lead to proactive behavioural changes as responses to perceived health issues. 26 Health-information-seeking behaviour is suggestive of an individual’s cognitive dissonance, as the individual may be seeking a solution for a perceived problem. 27 This may lead to proactive healthy behaviours, such as, efforts made to stop smoking. 28 Smokers who perceive negative health effects of smoking may seek additional information regarding smoking risks that could result in smoking reductions or cessation.
Health beliefs
Information can shape an individual’s beliefs. 29 Health beliefs result from an individual’s subjective assessment of existing information. Information is interpreted differently by individuals, and interpretation can vary based on environmental, cultural, societal, and other contextual factors. 24 An individual’s health beliefs, in turn, can affect perceptions of health risks. Perceived health risks affect whether and how an individual changes behaviour to promote health. 26
The Health Belief Model (HBM) is frequently used to understand health behaviour. This psychological model describes health behaviours and health-related decision-making by focusing on individuals’ beliefs. 30 Its central concept is that health behaviours are determined by personal beliefs as they relate to health issues. 31 The HBM has been used extensively in the area of smoking cessation to design programmes and health promotion efforts and to guide research.32-35
An individual’s health beliefs will affect how he or she perceives potential health risks and engages in health behaviour change. 36 Individuals who view prevention negatively are less likely to adhere to prevention recommendations. 37 In contrast, positive health beliefs may encourage individuals to seek health information and be proactive in their care. The willingness to engage in one’s care proactively has significant health consequences. 6 Persons with negative health beliefs such as ‘everything causes cancer’, which can imply that the risk of cancer is inevitable, appear more likely to engage in health-compromising behaviours like smoking and less likely to engage in health-promoting behaviours like exercise or healthy eating. In the context of smoking, if a smoker does not believe that smoking is bad for health, the smoker will be unlikely to participate in cessation activities. 38
Intention to quit smoking
A healthy lifestyle includes adoption of multiple protective behaviours, including, smoking avoidance, in an attempt to reduce the risk of illness. 6 Intention to quit smoking represents a positive behavioural intention. 15 Smokers, in an attempt to quit, go through several stages of lifestyle change behaviour. After they pass through a stage of not being prepared to quit, smokers contemplate an ‘intention to quit’ smoking. 39 The third stage is to prepare to quit. 39 While ‘intention to quit smoking’ is not the same as the engaged behaviour of nonsmoking, it appears strongly associated with quit attempts and cessation. 39
Methods
Sample and design
This study uses data collected in the fourth cycle of the Health Information National Trends Survey (HINTS), which was established by the US National Cancer Institute in 2003. The HINTS is a probability-based survey that collects nationally representative data about the use of cancer-related information in American adults age 18 or older. The HINTS cycle 4 data were conducted using a single-mode mail method, collected from August through November 2014. Of the approximately 14 000 people contacted, 3677 responded (26.26% response rate). Additional information about HINTS is available on hints.cancer.gov.
In using these data, we adjusted for potential nonresponse bias of people who did not take the survey through propensity score weights in the regression analysis. To calculate propensity score weights, first we generated propensity-matching scores and then calculated the propensity by getting the inverse of propensity scores for people who did not take HINTS (Applied Survey Methods, 2017). The response rate after propensity weighting was 34.44%. Exclusion criteria for our sample included nonsmokers (ie, answered ‘not at all’ to whether they currently smoke every day or on some days). The final analytic sample contained 494 observations of individuals who reported currently smoking every day or on some days.
Measures
Dependent variable
Our dependent variable was intention to quit smoking. It was determined from a HINTS question that asked if an individual had an intention to quit smoking within the next 6 months. This variable was dichotomous: either (1) intention to quit or (2) no intention to quit smoking.
Independent variable
The independent variable was health-information seeking. It was determined by response to whether a smoker looked for information on health and medical topics from any source. This variable was also dichotomous. Current smokers answered either ‘yes’ or ‘no’.
Mediator variable
Health beliefs was the mediator variable. It represents smokers’ agreement with two beliefs about cancer: (1) everything causes cancer and (2) prevention of cancer is not possible. The actual questions were worded as follows:
Health Belief No 1: ‘It seems like everything causes cancer’.
Health Belief No 2: ‘There is not much you can do to lower your chances of getting cancer’.
Respondents expressed agreement with each question on a scale of strongly agree (1), somewhat agree (2), somewhat disagree (3), or strongly disagree (4). We combined ‘strongly agree’ and ‘somewhat agree’ responses into the first category ‘agree’. We combined ‘somewhat disagree’ and ‘strongly disagree’ responses into the second category ‘disagree’. Missing responses for the health beliefs questions were coded as a third category, ‘missing’ because those respondents took the survey but did not respond to the particular health beliefs questions. The above categorizations were done to form more distinct demarcations between respondents who agreed, who did not choose to respond to the health beliefs questions, and the ones who disagreed. In addition, test reliability tends to decrease with too many response categories, which necessitated the use of fewer categories, and fewer categories simplified reporting and interpretation. Internal consistency of the two health beliefs was analysed, resulting in a Cronbach’s alpha of 0.48. This Cronbach’s alpha was less than the recommended level (0.7); therefore, the two beliefs could not be part of the same scale, and two separate models for each belief were used.
Control variables
Factors such as age, marital status, education, race, and occupation are associated with smokers’ intention to quit.40,41 Therefore, we used the following variables as controls in our study: age, employment status, marital status, educational attainment, race, and health insurance. Age was a continuous variable. Occupation status was modified into 3 categories: employed (0); unemployed, homemaker, student (1); retired, disabled, and other (2). Marital status was collapsed in 3 categories: married and living together (0); divorced, separated or widowed (1); and single (2). We created 4 categories of education: less than high school graduate (0); high school graduate (1); some college (2); and college graduate (3). Race was modified into 2 categories: white (0) and nonwhite (1). There were 2 categories of health insurance: insured (0) and uninsured (1).
Analysis
To explore whether health beliefs mediate the relationship between health-information seeking and intention to quit smoking, we used Baron and Kenny’s 42 method to test mediation. First, we regressed health beliefs on the independent variable (ie, health-information seeking) and assessed significance

Next, we conducted a second regression analysis to establish whether health-information seeking is predictive of intention to quit smoking. The equation was

The direct effects were significant, so we conducted a third regression analysis that regresses the intention to quit smoking on health-information seeking but also includes health beliefs as mediators. The equation was

To estimate the standardized regression coefficients and odds ratio, ordinal logistic regressions were used when health beliefs were the outcome variable (equation (1)) and logistic regressions were used when intention to quit smoking was the outcome variable (equations (2) and (3)). Only odds ratios are reported. We analysed 2 separate models for each health belief. Responses were weighted using probability-based weights based on the probability of being sampled as a survey respondent. To support results from the Baron and Kenny 42 method, we also ran the Sobel-Goodman test to assess what percentage of the total effect is mediated. All analyses incorporated survey weights using procedures of Stata 13.
Results
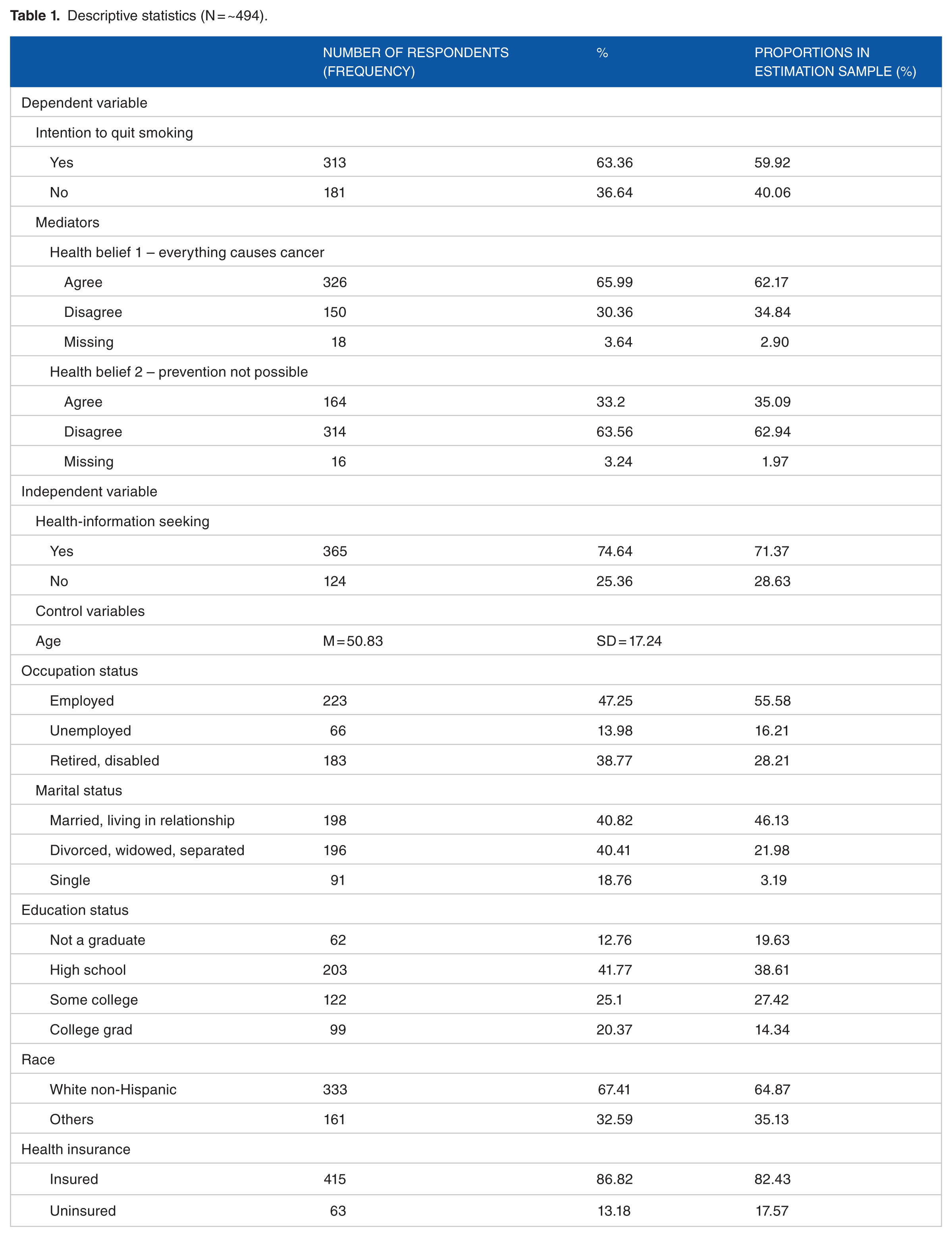
Descriptive statistics of our sample indicate that the average age of smokers was 51 and about half were employed. The number of smokers who were married was almost equal to the number who were divorced, widowed, or separated. Most smokers had only a high-school education, were white, and had health insurance. Approximately 63% smokers reported an intention to quit smoking. More than half of smokers agreed that everything causes cancer and disagreed that prevention of cancer is not possible. About 73% of smokers sought information on health and medical topics (Table 1). A comparison of the distribution in the actual sample and the estimation sample, that was created by propensity score matching, to account for nonresponse bias, is presented in Table 1. It indicates that both of the distributions are very similar.
Descriptive statistics (N = ~494).
Multivariable analysis
We conducted multivariable analyses to examine the relationship between health-information seeking and health belief 1 (ie, ‘everything causes cancer’). In model 1, respondents who agreed to health belief 1 were used as the reference group and compared to the respondents who disagreed to health belief 1 (Figure 1). We found no significant association between health-information seeking and health belief 1 (everything causes cancer) for model 1 (Table 2). In model 2, we found no significant association between health-information seeking and health belief 2, when respondents who disagree to health belief 2 (ie, ‘prevention of cancer not possible’) were compared with respondents who agree to health belief 2 (Table 2; Figure 2).

Model 1 – Mediation analysis investigating the association between health-information seeking and intention to quit smoking through health belief 1: ‘everything causes cancer’.
Regression results of the relationship between health-information seeking and health beliefs (N = 494).

Abbreviations: CI, confidence interval; OR, odds ratio.
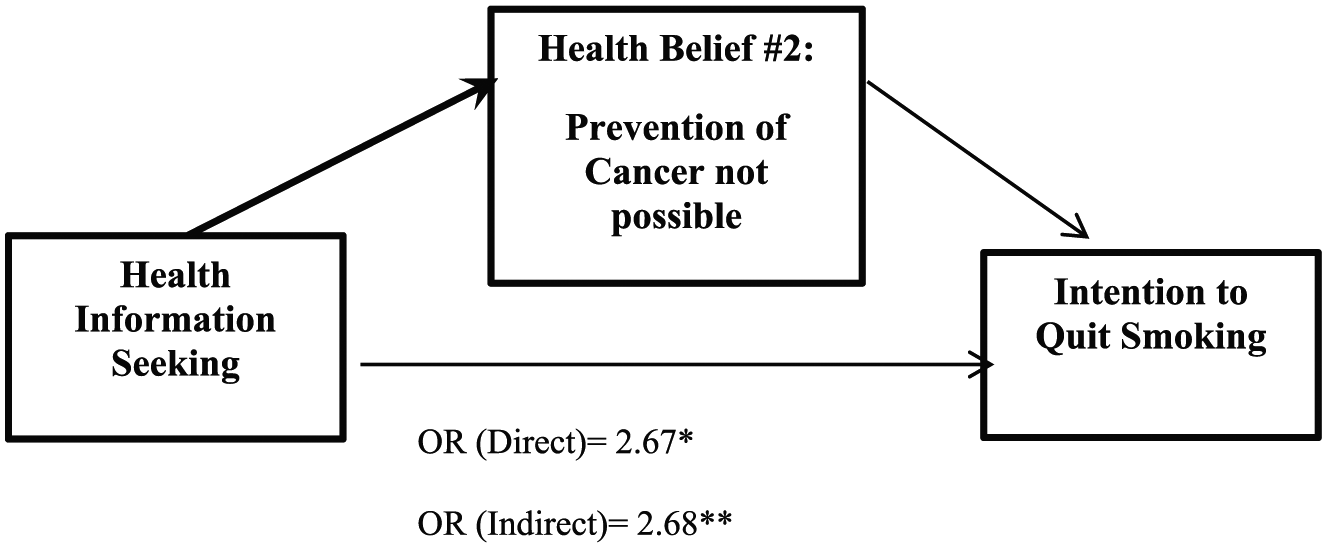
Model 2 – Mediation analysis investigating the association between health-information seeking and intention to quit smoking through health belief 2: ‘prevention of cancer not possible’.
Regression results of the direct relationship between health-information seeking and intention to quit smoking reveal that smokers who seek health information have a 2.67 times higher odds of intending to quit smoking compared to smokers who do not seek health information (Table 3).
Regression results of the direct relationship between health-information seeking and intention to quit smoking (N = 494).

Abbreviations: CI, confidence interval; OR, odds ratio.
P < .05.
Finally, as the last step in mediation analysis as suggested by Baron and Kenny, 42 we examined the indirect effect of health-information seeking on intention to quit smoking through health beliefs. In model 1, the intention to quit smoking is regressed both on health-information seeking and health belief 1 (ie, ‘everything causes cancer’) and health belief 2 (ie, ‘prevention of cancer not possible’), respectively. We expected the size of the coefficient to decrease or become nonsignificant to show true mediation. However, our results reveal that when the mediators are controlled for, the relationship between health-information seeking and intention to quit smoking still remains significant, with no substantial reduction in the size of the coefficient. Therefore, we can conclude that health beliefs do not have an intervening effect between health-information seeking and intention to quit (Table 4).
Regression results of the indirect relationship between health-information seeking and intention to quit smoking through model 1: health belief 1 – everything causes cancer, and model 2: health belief 2 – prevention of cancer not possible (N = 494).

Dependent variable is intention to quit smoking. Abbreviations: CI, confidence interval; OR, odds ratio.
P < .05; **P < .01.
Even after controlling for health beliefs, we found an association between health-information seeking and intention to quit smoking. Specifically, for model 1, after controlling for health belief 1 (ie, ‘everything causes cancer’), smokers who sought information had 2.84 times higher odds of intending to quit than smokers who did not seek information. For model 2, after controlling for health belief 2 (ie, ‘prevention of cancer not possible’), smokers who sought information had 2.68 times higher odds of intending to quit than smokers who did not seek information. In addition, results from the Sobel-Goodman test of mediation show that the mediation effect of health beliefs was not significant. Approximately 2% and 3% of the total effect of health-information seeking on intention to quit smoking was mediated by believing that ‘everything causes cancer’ and ‘prevention of cancer is not possible’, respectively (Table 4).
Discussion
This study hypothesized that health beliefs would mediate the relationship between health-information seeking and intention to quit smoking. However, we found that despite the negative aspects of health beliefs, health-information seeking behaviour influences smokers’ intentions to quit. Health beliefs about cancer, such as nothing can be done to prevent cancer, and everything causes cancer, appear not to play a mediating role. In other words, smokers who seek information would be more inclined to intend to quit, regardless of their beliefs about cancer. Our findings are consistent with this literature because they indicate that smokers who seek health information are at higher odds of intending to quit smoking than smokers who do not. Ample research suggests that information seeking can contribute to health-promoting behaviour.17,20,43 In our analysis, 73% of the smokers sought health information on some health or medical topic. But an important question remains how to encourage smokers to seek information about smoking in particular because evidence supports a link between seeking information about smoking and an interest in smoking cessation. 28
However, our findings of no significant association between health-information seeking and health beliefs and that health beliefs do not appear to have an intervening effect between health-information seeking and intent to quit are noteworthy. At least 2 cancer-related health beliefs (ie, ‘everything causes cancer’ and ‘prevention of cancer is not possible’) may not meaningfully connect to the health-promoting behaviour of seeking health information. This is surprising because the HBM emphasizes the role of personal beliefs in influencing health behaviours. 30 Thus, one could expect beliefs about cancer to affect a behaviour relevant to smoking cessation (ie, health-information seeking). But our analysis suggests that, at least these 2 health beliefs appear to play a limited role. This finding bolsters the significance of the act of seeking information, regardless of pre-existing beliefs. This finding asserts that health-information seeking about risks and disadvantages of smoking is imperative, despite pre-existing health beliefs, especially if those beliefs are negative. It lends additional support to cessation efforts that encourage smokers to act affirmatively on their interest in seeking health information. Of course, because other factors may be relevant, future research should investigate additional possible mediators, such as provider-patient communication about a healthy lifestyle, which could play an intermediary role between health-information seeking and intention to quit smoking.
Our findings are important for existing smoking cessation efforts. Multiple existing efforts aim to encourage smokers to quit. They include education-related interventions such as mass media campaigns, physician-smoker communications, news coverage, and interpersonal communication. As McGoldrick and Boonn 44 explain, they also include federal, state, local, and organizational policies that aim to discourage smoking, including taxes on cigarettes, warning labels on cigarette packs, and laws and policies promoting smoke-free environments. Our findings support more systematically deploying these efforts to encourage proactive information seeking by smokers. This may include mass media campaigns that urge smokers to speak with health care providers or affirmatively to seek out quit lines, labels that outline ways to access cessation resources, and smoke-free environments signage nudging smokers to seek cessation information.
Determining how best to encourage smokers to seek smoking-related information would require a combination of research and practice. This is a critical avenue of research and practice because it has the potential to increase the ability of cessation efforts to lead to successful quits. Achieving this would involve better understanding what types of cues and motivators (eg, friends, family, and a desire to make healthy lifestyle changes) encourage smokers to seek smoking-related information. Qualitative studies involving in-depth interviews of smokers could explore cues and motivators, while quantitative studies could investigate differences in quit outcomes based on various motivators and cues.
Additional implications for cessation can be gleaned from the characteristics of smokers in this study. First, almost three-quarters of smokers agree that ‘everything causes cancer’ and disagree that ‘preventing cancer is not possible’. This combination may evidence tensions around perceived susceptibility, perceived benefits, and self-efficacy, 3 concepts crucial for behaviour change under the HBM. 31 The belief that preventing cancer is possible is consistent with lower perceived susceptibility, higher levels of perceived benefit from prevention-related actions, and higher levels of self-efficacy. In contrast, the belief that everything causes cancer is consistent with higher perceived susceptibility, lower levels of perceived benefit from prevention-related actions, and lower levels of self-efficacy. Additional research could help elucidate how and why many smokers simultaneously adhere to health beliefs that may be in tension and thereby help with future HBM applications for cessation. To answer these questions, qualitative studies in particular may be of merit.
Finally, our finding that most smokers have health insurance is important for policy and practice. Brown and Wei 45 found that newly acquired access to private insurance may be connected to increased smoking cessation efforts. For the 17.57% of uninsured smokers, access to private insurance may be a useful avenue for cessation. For most smokers who are insured, there may be opportunities to capitalize on existing insurance policies to incentive seeking smoking-related information. For example, the Patient Protection and Affordable Care Act 46 requires many health insurance plans to cover tobacco use counselling and intervention efforts with no cost-sharing by the patient. For smokers covered by such plans, efforts to inform them of the availability of these services could enhance information seeking.
While this study contributes to the extant literature on predictors regarding intention to quit smoking, it is important to acknowledge some limitations. This study used a cross-sectional design, which limits the generalizability of our findings. In addition, in the literature, it has been argued that self-reported surveys may be inclined to a methodological issue, common method bias, which may inflate or deflate the associations among variables. In our study, to alleviate the issues due to common method bias, we ensured that propensity score matching was done and anonymity of respondents was maintained. The questions regarding health beliefs deal with cancer; however, there are other environmental and hereditary factors that can impact the risk of developing cancer besides smoking. The question on health-information seeking did not specify whether the information sought was unique to smoking. Although the response rate to this cycle of HINTS was similar to previous years (27%), further efforts are needed to capture nonresponders in future cycles.
Conclusion
Our study highlights the importance of health-information seeking – irrespective of cancer-related negative health beliefs – to attempting to quit smoking. Our study’s findings have direct implications for policy and practice. Policymakers and practitioners need to determine optimal ways to encourage smokers to seek smoking-related information. Such efforts will support achieving and maintaining smoking cessation. Cessation programmes and policies regarding smoking cessation should encourage smokers to seek health information regarding the disadvantages of smoking so that their intention to quit can be augmented, which increases the likelihood of converting smokers to nonsmokers.
Footnotes
Acknowledgements
The authors would like to thank the University of Nevada Las Vegas for their support in accomplishing this study. The authors would like to acknowledge the UNLV University Libraries Open Article Fund for supporting the publication fees for this article.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors were supported by the UNLV University Libraries Open Article Fund for the publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
SU conceptualized the study, and analyzed the data. SU and JL wrote the paper. MG revised and edited the paper.