
Abstract
Not much is known about disease prevalence, treatment outcomes, trained manpower, programs, and patients’ awareness of diseases from South Asia, compared with the Western world. While other aspects are improving, the quantitative evaluation of awareness of diseases is lagging. Compared with other diseases, the situation for mental health disorders and addiction is worse. While no single study can fully quantify all aspects of awareness, a good starting point is to understand if increasing the number of mental health facilities is beneficial by understanding people’s perception toward the likelihood of contracting various diseases, their preferred approach to treatment, and their perception of whether there are enough current facilities. We surveyed over 8000 families across several states of India and asked if they would treat a particular problem at home, visit a local healer, seek religious council, or go to a modern hospital for treatment. Our questions also included non-medical options to assess how likely people are to avoid trained medical help. We also asked people about their perceived likelihood of a family member ever suffering from (1) diarrhea, (2) high fever, (3) alcoholism, and (4) schizophrenia and other mental health problems. We reversed the order of diseases in our questions for a fraction of the population to evaluate the effect of order of questioning. Finally, we asked, if people feel they have enough local healers, religious places, general hospitals, de-addiction centers, and mental health facilities. Despite the taboo around mental health, many people claimed that their family members were unlikely to contract mental health or addiction problems, people recognized the severe paucity of mental health facilities and de-addiction centers. This raises hope for improving the mental health situation in India. We also found a significant relation between education levels and choices people make, underscoring the positive role education has in improving mental health.
Keywords
Introduction
Three-quarters of the global mental health burden is in low- and middle-income countries. Awareness and community participation are vital to reduce the mental health burden. In India, focused studies show a direct link between community participation and mental health, 1 indicating that wealth and longevity are significantly lower for people with mental health ailments. Stigma and discrimination against mental health patients is common, more so for women than men and the stigma is not just a rural phenomenan. 2
In addition to the problems with perception of mental health problems and community participation, there are equally severe issues of a lack of facilities and neglect of mental health problems by policymakers. Proportionate to the overall health burden and availability of economic interventions, governments tend to spend lower on mental health than other ailments in low- and middle-income countries. 3 In addition to resource limitation, their uneven distribution and a lack of transition from institution care to community care are other problems of poor countries. 4
There are several barriers to the improvement of mental health in low- and middle-income countries. Adequate and cheap medication alone cannot fix the epidemic of mental health problems, which would require broader interventions. 5 In addition to good mental health facilities, de-addiction centers, and trained ground level health workers, a cultural shift is also greatly needed. 5 That said, in our opinion, without adequate centers for de-addiction and specialized mental health hospitals, it is difficult to improve the mental health situation of low- and middle-income countries. We want to understand how receptive the population of India is to an increase in such centers. Given the stigma associated with mental health, 6 it is not obvious how people would respond to whether there is a need for facilities, what their preference of treatment would be, or if they would be willing to even accept the likelihood of themselves or their family members developing mental health problems. To address these problems, we conducted one of the largest nation-wide surveys.
Materials and Methods
The survey for this study was conducted by knocking door to door. Surveyors made an effort to sample from all strata of society from several states of India. To ensure that surveyors recorded the data properly, people’s names and phone numbers were also recorded and a small group of authors were assigned to call and verify the authenticity of the data. In the supplementary material containing all the raw data (supplementary data 1), the identity and contact information has been removed for privacy reasons. Consent of respondents was taken for the data to be used for research purposes only and they were informed that their phone numbers would not be stored for long term, shared with anyone, or used to make calls to them except for making a single call to verify the entry. In a pilot study, we found respondents were more willing to discuss the highest educational qualification in their family than overall or individual income; hence, to assess social standing of the person, we used education as a proxy. We did not explicitly collect information about ethnicity in this study.
The surveyors asked the following questions:
1A. If a member of your family were to contract a high fever, would you a. Treat it at home. b. Go to a local healer. c. Visit a religious preacher. d. Visit a doctor.
1B. Do you think it is likely that member of your family would contract high fever? a. Yes b. No
2A. If a member of your family were to contract diarrhea, would you a. Treat it at home. b. Go to a local healer. c. Visit a religious preacher. d. Visit a doctor.
2B. Do you think it is likely that member of your family would contract diarrhea? a. Yes b. No
3A. If a member of your family were to contract an alcohol addiction would you a. Treat it at home. b. Go to a local healer. c. Visit a religious preacher. d. Visit a doctor.
3B. Do you think it is likely that member of your family would contract an alcohol addiction? a. Yes b. No
4A. If a member of your family were to contract schizophrenia or other mental ailment would you a. Treat it at home. b. Go to a local healer. c. Visit a religious preacher. d. Visit a doctor.
4B. Do you think it is likely that member of your family would contract schizophrenia or other mental ailment? a. Yes b. No
5. Do you think your neighborhood has adequate a. Religious places and holy people? b. Local healers? c. General hospitals? d. De-addiction centers? e. Mental health facilities?
6. What is the maximum educational qualification in your immediate family?
Half the people surveyed were asked Question 1 to 4 with first question first and the fourth later and the other half with fourth first and first later to eliminate any effect from the order of questions.
We discarded any incomplete survey responses from our final responses and did not try to complete the responses in our confirmation call. The data were collected from 2017 June to 2018 January. We received 8663 complete responses from across India. We analyzed data only from the States and Union territories of India, where we could get more than 30 responses. These were Jharkhand, Madhya Pradesh, Chhattisgarh, Punjab, Uttarakhand, Gujarat, Bihar, Kerala, Odisha, Tamil Nadu, Assam, Haryana, Uttar Pradesh, Andhra Pradesh, Telangana, Rajasthan, Delhi, Maharashtra, Karnataka, and West Bengal. For plotting data on an Indian map, results from Andhra Pradesh and Telangana were combined, as the Python library used to plot does not contain the updated list of states.
For the analysis of a questions 1A, 2A, 3A, and 4A, various responses (a, b, c, d, along with their variations, eg, a, ba, cda, and bc) were analyzed according to the qualification of the person interviewed. In addition to plotting, their distribution connections were made in the diagram to visualize response for Circos plot (http://circos.ca/). For analysis of a question Q1B, 2B, 3B, 4B binary form 1 and 0, respectively, was taken for yes and no and mean value of questions for each state was calculated and plotted accordingly. For the analysis of a question Q5, counts for every option a, b, c, d, and e with their variation (a,d; b,c,d; a,e etc) were analyzed for each state. The count was then divided by the total number or response from their respective state to find the mean for an option (a,b,c,d). The means of responses of appropriate question are plotted on India’s map with a corresponding color intensity. States that have less than 30 points were left out of the analysis and are plotted in gray.
Results
We broke our analysis into response to a disease, acceptability of the likelihood of contracting a disease, and perceived inadequacy of facilities.
People claim openness in approaching a doctor for all health issues but likelihood of other alternatives depends on the disease and education level
For all 4 categories, diarrhea (Figure 1), high fever (Figure 2), alcohol addiction (Figure 3), and schizophrenia and mental health (Figure 4), people were most likely to choose a doctor over other alternatives of treating the problem at home, visiting a local healer, or visiting a religious preacher. For diarrhea (Figure 1), a large number of highly educated people claimed that they would treat it at home, not an unusual trend of self-medication. For high fever, a large fraction chose home treatment in addition to a major fraction visiting a physician (Figure 2). For both mental health–related questions, the higher educated population preferred to visit a physician (Figures 3 and 4). From Figures 1 to 4, a clear pattern emerged that the less educated are more likely to seek religious help. Also, for mental health disorders, even the higher educated strata seeked religious help. These data are plotted in a Circos plot in Figure 5.
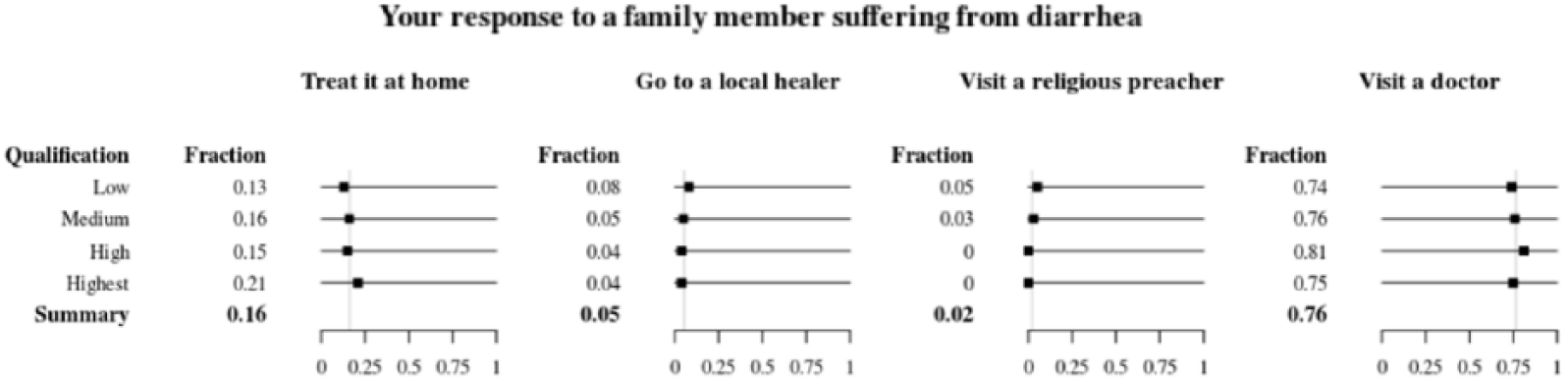
People’s preference of treating diarrhea.

People’s preference of treating high fever.

People’s preference of treating alcohol addiction.

People’s preference of treating schizophrenia and other mental health disorders.

Evaluation of people’s responses to different diseases as a function of educational status.
Accepted likelihoods for acquiring mental health and addiction problems are lower than for diarrhea and high fever
We analyzed the accepted likelihood of developing diseases in various states and found that people said that they or their family were unlikely to ever contract schizophrenia or other mental health disorders, followed by a somewhat higher acceptability of the likelihood of alcohol addiction. In comparison, the acceptability of contracting diarrhea or high fever was much higher (Figure 6 and Supplementary Figure 1).

Accepted likelihood of different diseases, presented as a heat map.
Adequate facilities
If a person’s response was that they were unlikely to ever contract a mental health disorder and they were being honest to themselves, one would imagine that they would not find a need for facilities that deal with these problems. However, this was not the case. In fact, most of those surveyed felt the need for de-addiction centers and mental health hospitals (Figure 7). That said, a very high fraction of people also felt a need for general hospitals, local healers, and religious places. We assumed that with so many religious places in India, this would not be the perception and were surprised by this result. A need for local healers and general hospitals is not surprising, given the known gap between facilities and demand. The silver lining from this particular line of questioning is that people clearly would like to see more de-addiction centers and more mental health facilities. Also, our analysis shows that people who are more educated are more likely to seek medical advice for mental health issues (Supplementary material 2).

Perceived abundance of different facilities.
Discussion
Our study, while confirming old ideas that there is a stigma related to mental health issues, shows that across India, people feel the need for more mental health care facilities and de-addiction centers.
The gap between availability and need for health services, known as the treatment gap, in low- and middle-income countries, tends to be around 75%. 7 We did not set out to measure the treatment gap for various diseases, this would be a future undertaking; instead, we focused the gap between people’s acceptance of the likelihood of contracting a disease versus their perceived need for specialized health care facilities. Our data clearly point toward the populations’ desire to see more mental health care facilities and de-addiction centers. We are, however, not proposing a simplistic solution of simply increasing the quantity of such centers.
While increasing the number of such centers is necessary, equally needed is an increase in the number and training of non-specialist mental health care professionals. 3 It is possible to achieve these goals in India with task sharing between specialists and community workers. 8 This type of distribution already works well with non-specialists for addressing perinatal depression in low- and middle-income countries. 9 A large number of traditional medicine practitioners can and should be forced to improve their practices with better regulation and formal training. We speculate that if this training also involves sensitization and training to properly deal with mental health problems, we could better distribute the task of managing the burden of mental health issues. More importantly, what has been already documented in a limited setting is that training primary care physicians in mental health makes a big difference. 10 We think that a systematic evaluation of which node of the network and which strategic allocation of resources is the best solution for a particular cultural context is a much needed analysis. We also think that an evaluation of religious council or elders’ advice by population should be systematically studied. If, in fact, a sizable population is going to religious preachers and elders, a policy initiative might be considered to sway their choice to instead go to primary health care physicians or even to provide community elders and religious preachers with proper training. Direct community outreach projects run by government or non-government organizations have shown promise in parts of India 11 indicating a strong need for the systematic evaluation of cost and success of such approaches and their possible integration with other programs. Community mental health programs are promoted all over the world, and there have been some interesting case studies from India. 12 In addition to community interventions, a diametrically opposite focused approach, which previously has been largely restricted to wealthy countries, is also being promoted for low- and middle-income countries. 13 In totality, our study shows people’s willingness to have more mental health facilities. It also suggests the need for better community education and training at a grassroots level. We would love to see how the synthesis of various approaches takes shape in the years to come.
Our study broaches on the subject of stigma but does not study it in any depth. By asking people about the likelihood of catching diseases and then whether they have adequate facilities, we do establish a mismatch, which is indicative of stigma. However, if we were to set out to study stigma, we would do a more disease-specific and stigma-centric study of patients, families, general public, local health care workers, general physicians, and specialist physicians. The fact that India has a very high stigma associated with mental health has been well established. 6 Also, it is unfortunately the case that not much is being done to deal with this stigma. 14 Stigma and completely uninformed views of mental health are prevalent in urban and highly educated areas of India as well. 2 A sense of alienation in the patient population, in addition to discrimination, contributes to the isolation of patients in India. 15 Differences in male and female patient experience for schizophrenia have been documented in India. 1 Stigma is not only to blame as a complete lack of realization that mental health problems are real health problems is also part of rural understanding in parts of India. 16 This is not seen only in the general public, even health care professionals are known to exhibit negative attitudes toward mental health patients and a systematic evaluation of health care professional attitudes is much needed for better policy formulation. Stigma has been associated with an under-reporting of mental health problems, seeking less treatment after diagnosis 17 and a battery of systematic studies for the Indian cultural context are long overdue. We hope that our study, which clearly lays out people’s understanding of the need for more mental health and de-addiction facilities, also underscores an urgent need to work toward an understanding of what is driving the stigma of mental health issues and eliminate it aggressively through educational, medical, cultural, and even judicial and political means.
Supplemental Material
Figure_1_supplementary – Supplemental material for Acceptability of Mental Health Facilities and De-addiction Centers in India
Supplemental material, Figure_1_supplementary for Acceptability of Mental Health Facilities and De-addiction Centers in India by Pahul Preet Singh, Ishan Goel, Amit Mondal, Farooq Ali Khan, Ashish Kumar Singh, Preeti Dubey, Sushma Chaudhary, P Venkata Anil Kumar Reddy, Viola Rodrigues, Vidhi Bassi, Karan Ahuja, Abhidith Shetty, Anjan Kumar Sahu, Karan Jodha, Nilesh Singh, Suprabhat Das, Rimi Sharma, Ria Bagaria, Sushmitha Poojary, Shrey M Gohil, Abhilash Bonu, Sushmita Vazirani, Leila Esfandiari, Sunil Shukla, Shubha Shukla and Sukant Khurana in Journal of Experimental Neuroscience
Supplemental Material
Supplementary_Material – Supplemental material for Acceptability of Mental Health Facilities and De-addiction Centers in India
Supplemental material, Supplementary_Material for Acceptability of Mental Health Facilities and De-addiction Centers in India by Pahul Preet Singh, Ishan Goel, Amit Mondal, Farooq Ali Khan, Ashish Kumar Singh, Preeti Dubey, Sushma Chaudhary, P Venkata Anil Kumar Reddy, Viola Rodrigues, Vidhi Bassi, Karan Ahuja, Abhidith Shetty, Anjan Kumar Sahu, Karan Jodha, Nilesh Singh, Suprabhat Das, Rimi Sharma, Ria Bagaria, Sushmitha Poojary, Shrey M Gohil, Abhilash Bonu, Sushmita Vazirani, Leila Esfandiari, Sunil Shukla, Shubha Shukla and Sukant Khurana in Journal of Experimental Neuroscience
Supplemental Material
Supplementary_material_2 – Supplemental material for Acceptability of Mental Health Facilities and De-addiction Centers in India
Supplemental material, Supplementary_material_2 for Acceptability of Mental Health Facilities and De-addiction Centers in India by Pahul Preet Singh, Ishan Goel, Amit Mondal, Farooq Ali Khan, Ashish Kumar Singh, Preeti Dubey, Sushma Chaudhary, P Venkata Anil Kumar Reddy, Viola Rodrigues, Vidhi Bassi, Karan Ahuja, Abhidith Shetty, Anjan Kumar Sahu, Karan Jodha, Nilesh Singh, Suprabhat Das, Rimi Sharma, Ria Bagaria, Sushmitha Poojary, Shrey M Gohil, Abhilash Bonu, Sushmita Vazirani, Leila Esfandiari, Sunil Shukla, Shubha Shukla and Sukant Khurana in Journal of Experimental Neuroscience
Footnotes
Acknowledgements
In addition to authors, whose role was data collection (more than 400 entries each), there were other citizen scientists who were involved in pilot studies (around 100 data points collected by each). We are very thankful to them: Aayushi Mehendiratta, Afshan Fathima, Anil Kumar Kummari, Chitra Prasad, Gargi, Hritvik Tripathi, Mani Pranay, Moumita Das, Neha Garg, Raja Shekhar, Ronuj Doley, Runa Pinto, Samanway Shree Pandey, Siri Manasa, Snehanjali Majumder, Sumith Tiwari, Vaishnavi R, Viplove Pradhan, Yash Saxena, and Arshdeep Sandal. Survey was conducted by volunteer citizen scientists.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
SK designed and mentored the project. He also wrote this paper with help of other coauthors: SS and S aided SK in overseeing the project: PPS and IG collated and analyzed the data; VR, FAK, AKS, PD, SC, and SS were involved in monitoring the collection of the data and helped with analysis; AM, PVAK R, VB, KA, AS, AKS, KJ, NS, SD1, RS, RB, SP, SMG, AB, SV, LE, and SS conducted the door to door survey.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.