
Abstract
Background:
In Ethiopia, teachers and bankers together represent a significant portion of the urban professional workforce approximately 900 000 teachers and 130 000 banking employees, accounting for nearly 7% of total employment. The nature of their work involves prolonged sitting, limited physical activity, and high mental workloads, which increase the risk of overweight and obesity. Bankers spend long hours at desks or computers, while teachers face extended classroom hours and administrative duties, often with limited access to recreational facilities. Unlike professionals in high-income countries, Ethiopian bankers and teachers generally have fewer workplace wellness programs, limited occupational health services, and lower awareness of lifestyle-related health risks. Adult overweight and obesity have risen sharply, exceeding 8% nationally and 20% in urban areas, posing a growing public health concern.. However, there is a lack of data on the lifestyle behaviors and health status, including factors related to overweight and obesity, among bankers and teachers in Ethiopia We investigated Factors associated with overweight and obesity among bankers and teachers in southern Ethiopia.
Methods:
We conducted a comparative cross-sectional study in Wolaita Sodo city from August 1st to 30th, 2022. A stratified sampling technique was used to select 227 bankers and 287 teachers. Data was collected using a modified version of the World Health Organization’s Stepwise approach to chronic disease risk factor surveillance tool. We used an ordinal logistic regression analysis to determine the factors associated with overweight/obesity.
Results:
The prevalence of overweight was 44.4% and 21.8% among bankers and teachers, respectively, while the prevalence of obesity was 14% and 4.37%. Among bankers, low physical activity (aPOR: 5; 95% CI: 1.73, 14.6), being female (aPOR: 2.82; 95% CI: 1.51, 5.27), marital status (aPOR: 2.62; 95% CI: 1.27, 5.43), snack intake habits (aPOR: 3.1; 95% CI: 1.37, 7.16), higher monthly income (aPOR: 2.47; 95% CI: 1.11, 5.50), and alcohol consumption (aPOR: 2.73; 95% CI: 1.45, 5.14) were significantly associated with overweight/obesity. For teachers, female sex (aPOR: 2.1; 95% CI: 1.18, 4.0), marital status (aPOR: 5.1; 95% CI: 2.13, 12.4), and low physical activity (aPOR: 3.38; 95% CI: 1.31, 8.70) were significant factors .
Conclusion:
Overweight and obesity are more prevalent among bankers than teachers in southern Ethiopia. Factors such as low physical activity, female gender, higher income, snacking habits, and alcohol consumption were strongly associated with overweight and obesity. Targeted workplace health promotion and non-communicable disease prevention strategies are urgently needed to address these risks among sedentary professionals.
Background
Obesity and overweight refer to abnormal or excessive fat accumulation, which is a cluster of risk factors for non-communicable diseases. A body mass index (BMI) > 25 and >30 is considered overweight and obese, respectively. 1 An estimated 2.5 billion individuals worldwide are overweight or obese, attributed to an estimated 3.7 million noncommunicable disease (NCDs) related deaths.1,2 In middle- and low-income countries, the prevalence of overweight is alarmingly rising due to the rapid nutrition transition, mainly among urban inhabitants and affluent people. 3
Professionals such as bankers and teachers represent a significant subpopulation of the urban middle-class who are increasingly exposed to an obesogenic environment characterized by sedentary work, high-calorie diets, stress, and limited physical activity. 4 Bankers, for instance, spend the majority of their working hours sitting, performing desk-bound duties, and engaging in screen-based activities with minimal physical activity. This sedentary job pattern, together with income-associated eating habits such as increased consumption of processed foods and sugary drinks, puts them at higher risk of overweight and obesity.5,6 Similarly, long teaching hours, stress, insufficient breaks, and poor workplace health promotion policies are frequently seen, potentially impeding their ability to maintain a healthy lifestyle. 7
In Ethiopia, recent national surveys and sub-national studies have indicated a growing trend in overweight and obesity, particularly among urban dwellers and working adults.8,9 The 2016 Ethiopia Demographic Health Survey (EDHS) reported that the prevalence of overweight or obesity among women in urban areas was over 21%. 8 The prevalence of overweight and obesity among working adults ranges from 24.4% in Addis Ababa to 48.6% in Gondar City, Ethiopia.10,11 Furthermore, socio-demographic variables such as female sex, 12 older age, 13 educational status, 14 dietary diversity score, 15 wealth status, 16 low physical activity,17,18 urban dwellers, 19 alcohol intake,6,13,16 year of work and having a private car. 5 On the contrary, eating fruit and vegetables and smoking both significantly decrease the likelihood of being overweight or obese.7,20
Alarmingly, overweight and obesity are significant contributors to the rising burden of non-communicable diseases (NCDs),21 -23 including hypertension, coronary heart disease, type 2 diabetes mellitus, joint and muscular disorders, respiratory problems, and cancer. 21 NCDs are anticipated to suppress infectious diseases by 2030.24,25 Obesity is a major cause of disability-adjusted life years and an important risk factor for premature death. 21
Despite these growing challenges, there is a paucity of data focusing specifically on occupational subgroups most at risk, such as bankers and teachers. Previous studies in Ethiopia have tended to generalize overweight and obesity prevalence across urban populations without adequately exploring the differential risks and contributing factors in specific professional settings.9,13,15,26,27 This limits the development of tailored interventions that address the unique occupational and behavioral context of these groups. Identifying modifiable risk factors within these professional groups is essential for informing targeted public health interventions and workplace wellness programs that can contribute to the prevention and control of overweight and obesity among working Ethiopian adults. Therefore, this study aimed to investigate the factors associated with overweight and obesity among bankers and teachers in Wolaita Sodo city, southern Ethiopia.
Methods and Materials
Study Area and Period
The study was conducted in Wolaita Sodo city, southern Ethiopia, which is 330 km south of Addis Ababa, the capital city of Ethiopia. Wolaita Zone is one of the administrative zones in the South Ethiopia Regional State, and it has 16 districts and 8 town administrations. Wolaita Sodo approximately 6.9° north of the equator and 37.75° east of the Prime Meridian. The city serves as the administrative and economic hub of the Wolaita Zone in southern Ethiopia. It is situated at an elevation ranging between 1600 and 2100 m above sea level. The city consists of 1 public university, two public and 6 private colleges, 17 primary schools, 15 kindergartens, 4 public and 2 private preparatory schools, and 7 public and 3 private high schools. Additionally, the city consists of 32 different bank branches. This study conducted in randomly selected 5 different bank branches and 5 schools. There are 397 teachers and 315 bankers in those selected schools and banks. The study was conducted from August 1 to 30, 2022.
Study Design and Population
We conducted a comparative cross-sectional study among bankers and teachers. The source populations were all bankers and teachers who were working at the schools and banks in Wolaita Sodo city. The study included randomly selected bankers and teachers who worked in banks and governmental schools in Wolaita Sodo city. Participants who had worked for less than 6 months or who were pregnant were excluded from the study. Additionally, those with known non-communicable diseases and on long-term medications (that could affect body weight) were excluded from the study.
Sample Size Determination
The sample size was calculated using the double population proportion formula in Epi Info, considering a 95% confidence interval, 80% power, a 1:1 ratio of P1 to P2, where P1 = 77.7% (proportion of overweight/obesity among bankers) and P2 = 62.6% (proportion among teachers) based on a previous study in Tanzania. 5 A design effect of 1.5 and a 10% non-response rate were included. The calculated sample size was 514.
Sampling Technique
Study participants were recruited using a 2-stage sampling procedure. In the first stage, 5 branches out of 32 banking branches and 5 schools out of 28 (approximately 20% of clusters, in line with WHO recommendations) were purposively selected based on the size of their staff. The 5 selected banks were Commercial Bank of Ethiopia (CBE), Wolaita Sodo and Dicha branch, Nib, Dashen, and Awash Bank Sodo branch, and the 5 schools (Ligaba Beyen, Bogale Walalo, Ototna, Wana Wagesho, and Gugtuto Secondary and Preparatory School) were selected to achieve the primary sampling units. In the second stage, the total sample size of 514 participants was proportionally allocated, with 227 bankers and 287 teachers distributed according to the number of staff in each selected setting. Within each institution, a simple random sampling technique was employed: each eligible staff member was assigned a unique code, and participants were randomly selected by drawing codes until the allocated sample size for that setting was achieved (Figure 1).
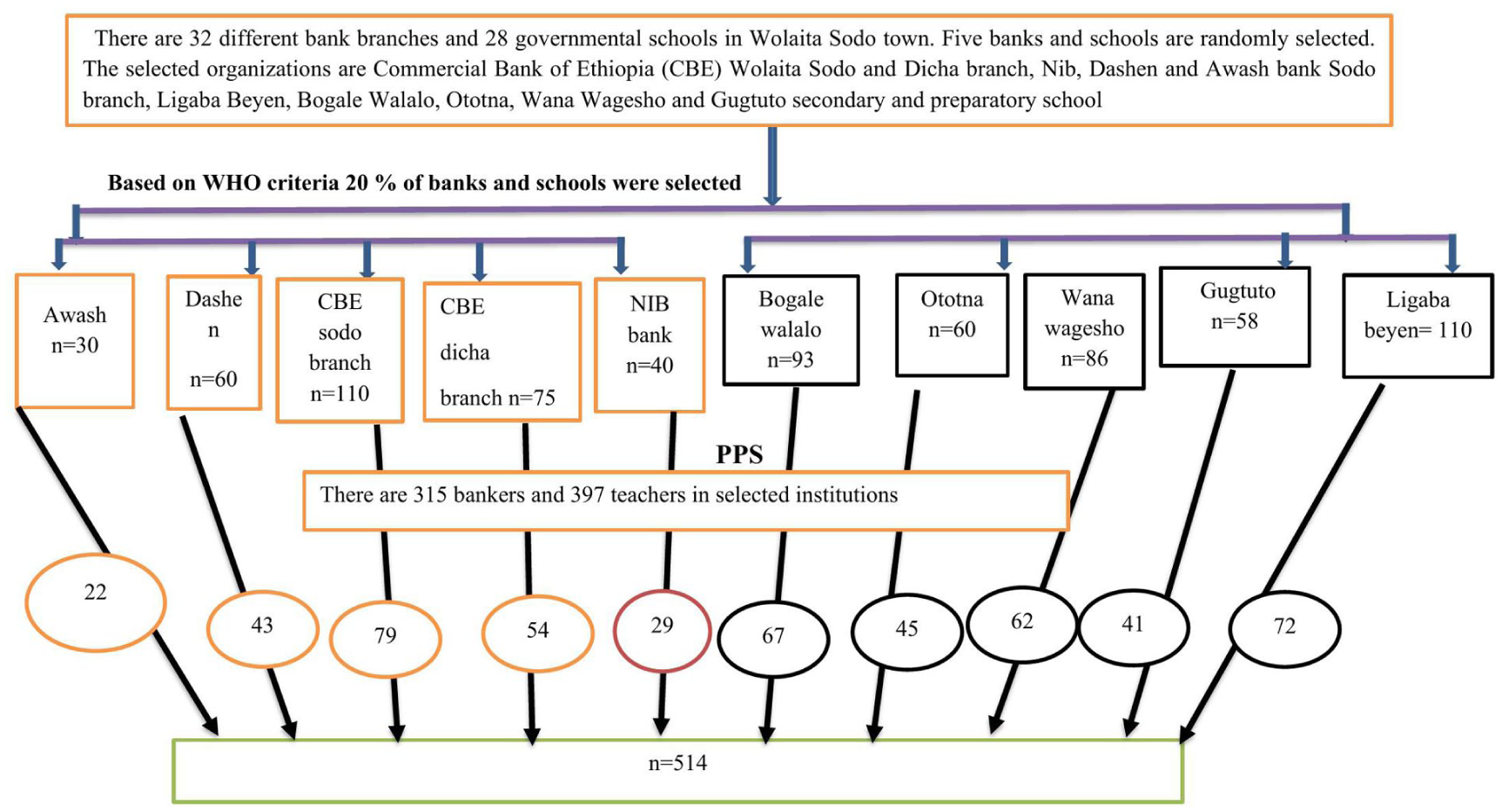
Schematic presentation of sampling procedure to assess the prevalence and factors associated with overweight and obesity among teachers and bankers in Sodo city, south Ethiopia, 2022.
Variables of the Study
The dependent variable of the study was the level of nutritional status among bankers and teachers (normal, underweight, overweight, and obese). Independent variables include age, sex, marital status, occupation, educational status, and monthly income, and behavioral and lifestyle factors (physical exercise, dietary habits, and alcohol intake).
Operational Definitions and Measurements
Data Collection Tool and Procedure
Data were collected using a structured and pre-tested questionnaire, adapted from the WHO STEPwise approach to chronic disease risk factor surveillance (STEPS) tool.13,28 The questionnaire was translated from English to Amharic by a bilingual expert and back-translated into English by a second independent expert. Discrepancies were resolved by the translators and research team to ensure accuracy, clarity, and faithful representation of the original content. . The questionnaire included 3 main sections: Socio-demographic information (age, sex, marital status, education, income), Lifestyle behaviors (physical activity, smoking, alcohol consumption, eating habits), occupational characteristics (working hours, administrative vs teaching tasks, breaks). Participants were informed about the study objectives, confidentiality, and their right to withdraw at any time. Five BSc nurses collected the data under the supervision of a public health expert.
Anthropometric Measurements
The weight was measured using the SECA 874 flat weighing scale, Hamburg, Germany, to the nearest 100 g. Height was measured to the nearest 0.1 cm using a standing height board. Body mass index (BMI) was determined by dividing body weight in kilograms by height in square meters (kg/m2). Participants were categorized as underweight, normal, overweight, or obese, using BMI values of 18.5, 18.5-24.9, 25-29.9, and 30 kg/m2, respectively. 29
Assessment of Dietary Habits
Dietary habits were assessed using a Food Frequency Questionnaire (FFQ), with participants reporting the frequency of consumption of key food items, including fruits, vegetables, snacks, and sugary drinks over the past 1 month. 13
Physical Activity
The intensity, duration, and frequency of physical activity in work, transportation, and leisure situations were estimated using the Global Physical Activity Questionnaire. Days, hours, and minutes of physical activity lasting at least 10 minutes each day were included in the data. Energy expenditure was measured using the metabolic equivalent (MET). Using the standard classification technique, individuals were categorized as high, moderate, or low in terms of their degree of physical activity. 28 A vigorous physical activity includes running, jogging, high-intensity aerobic classes, or competitive full-field sports, while low physical activity refers to people who exercise little. Moderate physical activity includes brisk walking or hiking, low-impact aerobics classes, and recreational team sports.
Alcohol Intake
Alcohol intake was assessed qualitatively via a yes/no question about consumption in the past 30 days. Participants were classified as current alcohol consumers or non-consumers. 6
Data Quality Assurance
A pre-test of the tool was conducted using 5% of the study participants. Data collectors and supervisors received a 1-day training on the study’s goals, data gathering techniques, inclusion and exclusion standards, and data completeness. To ensure data accuracy, anthropometric measuring instruments were calibrated before measurement. Supervisors provided daily remarks on error elimination and corrective actions, and cross-checked data collectors for consistency and completeness.
Data Processing and Analysis
The Open Data Kit (ODK) was used to gather the data, and analyzed using STATA Version 16 software. The lifestyle and descriptive character of the subjects were described using descriptive statistics such as dispersion, central tendency measures, and frequency distributions. We used an ordinal logistic regression model to find factors that are associated with the level of nutritional status. The ordinal logistic regression model was used because the nutritional status determined by using BMI is ordinal data (normal vs overweight vs obese). Chi-square and parallel line tests were used to verify the proportional odds model’s (POM) assumptions. Bivariable analysis was used to assess factors associated with nutritional status, with variables with a P-value <.25 included in the multivariable POM to control potential confounders. With significance at a P-value <.05, the strength of the statistical association among explanatory and outcome variables was assessed using an adjusted proportional OR with a 95% CI.
Results
Participants Characterizations
Socio-Demographic and Economic Characteristics
The study included 504 participants in total (297 teachers and 207 bankers), yielding a 98% response rate. The mean age (SD) of teachers was 32.2 (±5.9) years, and it was 33.9 (±5) years for bankers (P < .001). One hundred twenty-nine (43.4%) teachers and 69 (33.3%) bankers were aged less than 30 years (P = .042). One hundred eighty-two (61.3%) teachers and 128 (61.8%) bankers were males. Ninety-eight (36%) teachers and 165 (79.7%) bankers earned more than 10000 Ethiopian birr per month (P < .001). Fifty-seven (19%) of teachers, and 74 (35.7%) have a master’s degree. Nearly a quarter (22.5%) of teachers and 34 (16.4%) bankers have a family size of 5 and above (P = .001; Table 1).
Socio-demographic and Economic Characteristics of the Study Participants, Wolaita Sodo City, Southern Ethiopia, 2022 (n = 504).

Lifestyle Characteristics
One hundred seventy-six (59.3%) and 144 (69.5%) of bankers had a low physical activity level (P = .054). One hundred fourteen (38.4%) teachers and 86 (41.5%) bankers had consumed alcohol. More than half of 171 (57.8%) teachers and 115 (55.5%) bankers typically eat 3 meals a day, and 31% and 48.3% of teachers and bankers, respectively, take an additional snack. More than half (58.2%) of teachers and 162 (41.7%) bankers reported frequently eating away from home, whereas 58.8% and 41.1% of teachers and bankers, respectively, consume fast foods once per week (Table 2).
Lifestyle Characteristics of the Study Participants, Wolaita Sodo City, Southern Ethiopia, 2022 (n = 504).

Prevalence of Overweight and Obesity
The overall prevalence of overweight and obesity among teachers and bankers was 157 (31.1% [95% CI: 27.2, 35.3]) and 42 (8.3% [95% CI: 6.2, 11]). The prevalence of overweight was 44.4% [95% CI: 37.6, 51.2], and obesity was 14% [95% CI: 9.26, 18.7] among bankers. While the prevalence of overweight was 21.9% [95% CI: 17.1, 26.5] and obesity was 4.4% [95% CI: 2.04, 6.70] among teachers. The chi-square (χ²) test was used to assess the association between nutritional status and Job of participants (χ² = 54.4, P < .001), indicating a statistically significant difference (Figure 2).
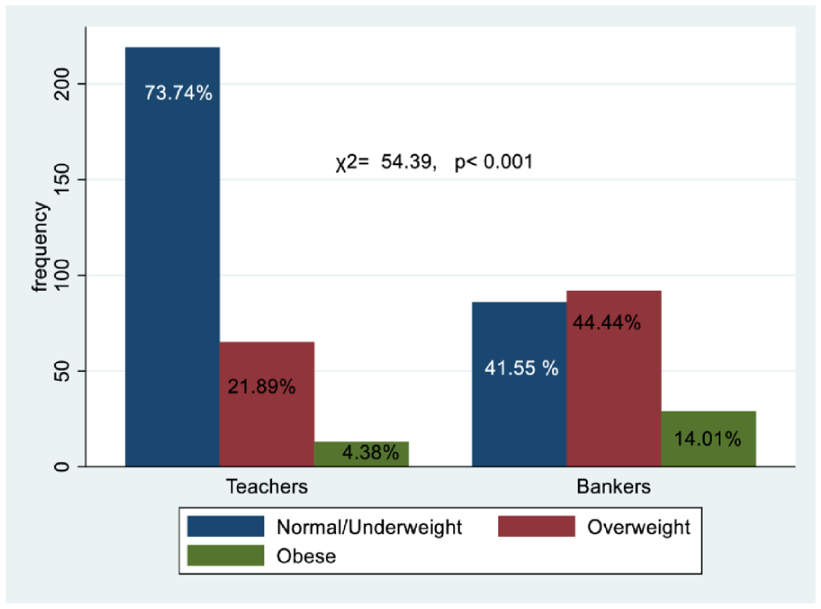
The level of nutritional status of Teachers and Bankers in Wolaita Sodo city, Southern Ethiopia, 2022 (n = 504).
Factors Associated with Overweight and Obesity Among Teachers
In the bivariable proportional odds model, age, sex, marital status, physical activity level, monthly income, away-from-home eating, and snack intake were associated with overweight and obesity. While in the final POM, sex, marital status, and physical activity level were independent risk factors for overweight and obesity among teachers.
At the 5% level, the chi-squared test of parallelism demonstrated that the ORs for the final model were constant across all nutritional status cutoff points (
Factors Associated with the Level of Nutritional Status Among Teachers, Wolaita Sodo, Southern Ethiopia, 2022 (n = 297).

Abbreviations: cPOR, crude proportional odds ratio; aPOR, adjusted proportional odds ratio, currently unmarried (single, divorced, and separated).
Significant at a P-value <.05 level.
Significant at a P-value <.001 level, Variables with P-value >.25 in the bivariate analysis were excluded from the multivariable logistic regression model, hence the blank cells.
Factors Associated with Overweight and Obesity Among Bankers
In the bivariable proportional odds model, age, sex, marital status, family size, educational status, physical activity level, monthly income, alcohol consumption, and snack intake were associated with overweight and obesity. While in the final POM, sex, marital status, and physical activity level were independent risk factors for overweight and obesity among bankers. The chi-squared test of parallelism showed that the ORs were constant across all cutoff points of nutritional status for the final model at a 5% level (
The results of POM revealed that the likelihood of being overweight or obese was 2.82 times (aPOR: 2.82; 95% CI: 1.51, 5.27) higher among females compared to males. Likewise, married participants were 2.62 times more likely to be overweight or obese (aPOR: 2.62; 95% CI: 1.27, 5.43) compared to their counterparts. The odds of being in the higher order of nutritional status (overweight or obesity) was 5 times (aPOR = 5; 95% CI: 1.73, 14.6) and (aPOR = 3.99; 95% CI: 1.19, 13.3) higher among those engaged in low and moderate physical activity levels compared to participants who had high physical activity levels.
In addition, the risk of being in the higher order of nutritional status (overweight or obesity) was 3.1 times (aPOR = 3.1; 95% CI: 1.37, 7.16) higher among participants who had snack intake habits compared to those who had no habit of snack intake. The odds of obesity or overweight were 2.73 times (aPOR = 2.73; 95% CI: 1.45, 5.14) higher among participants who consumed alcohol compared to their counterparts. Moreover, the odds of being overweight or obese were 2.5(aPOR = 2.47; 95% CI: 1.11, 5.50) times higher among those participants who earn a high monthly income as compared to their counterparts (Table 4).
Factors Associated with the Level of Nutritional Status Among Bankers, Wolaita Sodo, Southern Ethiopia, 2022 (n = 207).

Abbreviations: cPOR, crude proportional odds ratio; aPOR, adjusted proportional odds ratio, currently unmarried (single, divorced, and separated).
Significant at a P-value <.05 level.
Significant at a P-value <.001 level, Variables with P-value >.25 in the bivariate analysis were excluded from the multivariable logistic regression model, hence the blank cells.
Discussion
The study found the prevalence of overweight and obesity among bankers was 44.4% and 14%, respectively, whereas it was 21.8% and 4.3% for teachers. The finding was consistent with a study conducted in Tanzania, which found that the prevalence of overweight was higher among bankers than teachers. 5 The higher prevalence of overweight and obesity among bankers may be attributed to several interconnected factors, including occupational, behavioral, and socioeconomic factors. Banker often engages in prolonged sedentary work, spending over 8 hours a day in front of or at customer service desks, with limited physical activity. This can lead to higher work-related stress, poor dietary choices, and reduced physical activity. Additionally, socioeconomic factors, such as higher incomes and access to calorie-dense convenience foods and sedentary leisure activities, also contribute to overnutrition.
Overall, 39.4% of bankers and teachers were overweight or obese (31.1% overweight and 8.3% obese). The finding was lower than a study conducted in Nigeria (48.9%), 12 Ghana (55.6%), 6 Tanzania (68.9%), 5 Brazil (47.2%), 7 India 47.9%, 30 and 59.1% in a German kindergarten teacher. 31 This might be due to the differences in culture, socioeconomic status, study population, levels of physical activity, and genetics. However, the finding was higher than a study conducted in Addis Ababa city (24.4%), 11 Hawassa city (28.2%), 13 and Dessie town (28.5%). 16 The higher prevalence of overweight or obesity among bankers and teachers may be due to sedentary behaviors, work nature, and socio-economic status, which may encourage less physical activity and unhealthy diets. 6
The study found that being overweight or obese had a significant association with being a woman. This finding was corroborated by a study done in Hawassa, 13 Nigeria, 12 and Tanzania. 6 This could be because biological factors, including less lean mass and more fat mass, and sex hormones during childbearing, increase the risk of excess weight gain.32,33
Low levels of physical activity significantly raise the risk of being overweight or obese. This result is supported by other similar studies done in Hawassa, 13 Nigeria, 12 Ghana, 6 and Brazil. 34 The possible reason explained by muscular contraction during physical activity is that it burns energy, and being physically inactive is a risky health behavior, which is one of the greatest contributors to obesity. 35 Additionally, we found that moderate-level physical activity was significantly associated with overweight/obesity among bankers, whereas this association was not statistically significant among teachers. This difference may reflect the interplay between occupational sedentary behavior, physical activity patterns outside of work, and overall energy expenditure in these 2 professions.
In our study, alcohol consumption was significantly associated with overweight and obesity, consistent with studies conducted at Dessie Town, 16 Addis Ababa, 9 and Accra, Ghana. 6 Alcohol consumption may lead to excessive energy intake, reduce physical activity, weight gain, increased hunger, and hindered fat burning, resulting in overeating and weight gain. 36 The study found that snacking habits among participants were 3 times more likely to lead to overweight. The finding is supported by another study conducted at Dessie Town. 16 The odds of being overweight or obese were 2.45 times higher among participants with high monthly income compared to their counterparts. The result is supported by other studies done in Hawassa City, 13 Dessie town, 16 Ethiopia, 19 and Kenya. 37
Moreover, participants with a higher monthly income had 2.5 times greater odds of being overweight or obese compared to those with lower income. This aligns with findings from other urban areas in Ethiopia, such as Addis Ababa and Hawassa, where sedentary occupations and higher income levels were associated with increased obesity risk.13,38,39 These suggest that higher income levels may facilitate access to energy-dense foods and sedentary lifestyles, contributing to increased obesity risk.
Limitations of the Study
Several limitations should be acknowledged. First, the study used a cross-sectional design, which limits the ability to establish causality between occupational factors and overweight/obesity. Second, the study population was restricted to teachers and bankers in Wolaita Sodo City, which may limit the generalizability of the findings to other occupational groups or rural settings. Third, data were collected over a short period of 1 month, which may not capture seasonal variations in dietary habits or physical activity. Additionally, some behavioral variables, such as diet and alcohol intake, relied on self-report, which may introduce recall or social desirability bias. Finally, certain potentially relevant variables, including years of work experience, family history of obesity, and detailed workplace wellness interventions, were not collected, which may have affected the ability to fully explain observed associations.
Conclusion
The study found a higher prevalence of overweight and obesity among bankers compared to teachers in Wolaita Sodo City. Key factors associated with increased risk included female sex, low physical activity, unhealthy dietary habits, alcohol consumption, marital status, and higher monthly income. These findings highlight the need for targeted workplace interventions and public health strategies aimed at promoting healthy lifestyles among urban professionals. Implementing occupational health programs, wellness initiatives, and health education tailored to the specific challenges faced by bankers and teachers could help reduce the burden of overweight and obesity and prevent associated non-communicable diseases.
Footnotes
Acknowledgements
We would like to thank the schools and bank staff for providing me necessary information regarding my topic of study. Our special thanks go to the data collectors for their cooperation during data collection. Finally, we would like to thank the study participants for their kind participation and cooperation.
Author’s Note
Awoke Abraham is now affiliated with Public Health Research, School of Public Health, Walailak University, Nakhon Si Thammarat, Thailand.
Ethical Considerations
The study was approved by the Institutional Review Board/IRB of Wolaita Sodo University, College of Medicine and Health Science (Ref CRCSD 123/02), and conducted according to the principles of the Declaration of Helsinki. Written consent was obtained from participants. They were informed of the voluntary nature of participation and were assured of confidentiality. Personal identifiers were not included in the data collection format to maintain confidentiality and privacy. Obese participants were educated on obesity’s health implications, regular physical activity, and healthy eating habits, and introduced to dietitians for weight management.
Consent for Publication
Not applicable.
Author Contributions
ME contributed to the conception, design, and supervising data collection, analysis, and interpretation, DDA contributed to the design, analysis, and interpretation, and ZB, AA, and AG conducted the analysis, interpreted the findings, and wrote the manuscript. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Almost all the data are included in this study. However, additional data will be available from the corresponding author upon reasonable request.
Trial Registration
Not applicable.