
Abstract
Background:
As a worldwide pandemic, metabolic syndrome (MetS) is related with high disease burden. The emergence of multiple chronic diseases can be attributed to unfavorable dietary and lifestyle choices made by individuals, with hyperinsulinemia and insulin resistance as the underlying causes. Current study sought to assess the relationship between the Empirical Dietary Index for Hyperinsulinemia (EDIH) and the Empirical Lifestyle Index for Hyperinsulinemia (ELIH) and MetS risk factors.
Methods:
This cross-sectional study involved 339 individuals between the ages of 20 and 50, who were either obese or overweight, and were recruited from Tabriz, Iran. In this study, a validated semi-quantitative Food Frequency Questionnaire (FFQ) with 168 questions was used to assess individuals’ food consumption. Blood tests were performed to assess total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), triglyceride (TG) levels, as well as blood glucose and insulin levels.
Results:
After multivariable adjustment, among tertiles of EDIH, systolic blood pressure (SBP) and TG were significantly different. Also, SBP, diastolic blood pressure (DBP), and HDL-C significantly differed across tertiles of ELIH. In multivariate-adjusted models, individuals classified in the highest tertile of EDIH demonstrated elevated ORs in relation to FBG levels [OR: 1.035 (1.004-1.068; P < .05)], and the second tertile of ELIH was inversely associated with SBP [OR: 0.966 (0.935-0.999; P < .05)], DBP [OR: 0.972 (0.948-0.997; P < .05)], TG in the model I [OR: 0.991 (0.983-0.999; P < .05)], and model II [OR: 0.991 (0.983-0.999; P < .05)].
Conclusion:
Considering the findings of our study, higher insulinemic dietary potential, indicated by EDIH, can be related to higher odds of FBG and decreased odds of TG as risk factors of MetS. Furthermore, our findings suggest that individuals with a higher ELIH may potentially exhibit lower SBP and DBP levels. Nevertheless, further experimental and long-term investigations are necessary to fully comprehend this association.
Background
Metabolic syndrome (MetS), a prime instance of non-communicable conditions brought on by modern lifestyle choices, is rising worldwide. A cluster of cardiovascular risk factors such as abdominal obesity, insulin resistance, hypertension, impaired glucose metabolism, and dyslipidemia define MetS. 1 MetS raises the likelihood of developing cardiovascular diseases by twofold and the risk of type 2 diabetes by fivefold. Individuals with metabolic syndrome also have a more extensive disease burden on healthcare systems than those without metabolic syndrome. 2 In this regard, MetS can be controlled and precluded by improving modifiable lifestyle risk factors such as diet.3-5
According to recent research, a well-balanced diet can also alter insulin homeostasis. 6 Unbalanced insulin levels (including hyperinsulinemia) are a critical factor in the development of MetS. 7 Poor dietary and lifestyle choices are related to developing several chronic diseases, with hyperinsulinemia and insulin resistance being the underpinning mechanisms. 8 Over the past few years, Tabung et al 9 have developed indices to evaluate the possible insulinemic effects of a diet and lifestyle, including the Empirical Dietary Index for Hyperinsulinemia (EDIH) and the Empirical Lifestyle Index for Hyperinsulinemia (ELIH). Numerous studies investigated these indices in relation to the risk of colorectal cancer,10,11 digestive system cancers, 12 multiple myeloma,13,14 prostate cancer,15,16 type 2 diabetes,17-19 hepatocellular carcinoma, 20 insulin-related disorders, 21 pancreatic cancer, 22 obesity phenotypes, 23 breast cancer,24,25 chronic kidney disease, 26 non-alcoholic fatty liver disease, 27 endometrial cancer, 28 postmenopausal women’s overall and site-specific cancers, 29 and in association with weight gain in adults, 30 survival rates for colon cancer patients,8,31 and inflammation. 32
However, no research has been done on the effect of diet and lifestyle insulinemic potential on MetS risk factors. With the escalating prevalence of MetS, the present study aimed to explore the relationship between dietary and lifestyle indices associated with hyperinsulinemia and the risk factors of MetS in adults with overweight and obesity residing in Tabriz, Iran.
Methods
Participants
In Tabriz, Iran, 339 people with overweight and obesity participated in this cross-sectional study (Figure 1). Participants for this study were selected from research conducted at Tabriz University of Medical Sciences, spanning two different studies.33-35 The inclusion criteria for participants in this study required them to be within the age range of 20 to 50 years and have a body mass index (BMI) exceeding 25 kg/m2. Pregnancy, breastfeeding, and menopause, as well as hepatic and renal illnesses, cancer, cardiovascular diseases, diabetes mellitus, recent bariatric surgery, malabsorptive disorders, and weight-altering medicines or supplements, were exclusion criteria. All the patients gave their written informed consent to participate in the study, and the Ethics Committee of Tabriz University of Medical Sciences, Iran, approved the study protocol (code: IR.TBZMED.REC.1396.768 and IR.TBZMED.REC.1398.460).

Study Flowchart.
Baseline profile and body measurements
A detailed description of the methods has been published previously. 36 In summary, we used a questionnaire to collect sociodemographic information. Then, we calculated the socioeconomic status (SES) score. Weight, height, body composition, waist circumference (WC), hip circumference (HC), and blood pressure were also measured. Further, physical activity was assessed via a short form of the International Physical Activity Questionnaire (IPAQ). 37
Dietary assessment
A qualified nutritionist utilized a validated semi-quantitative Food Frequency Questionnaire (FFQ), 38 to ask participants about their yearly food diary. Participants detailed their daily, weekly, monthly, or yearly food intake, specifying both types and quantities. The amount of food consumed per serving was converted into grams per day using standard common portion sizes. 39 Daily dietary consumption was analyzed using the USDA database.
Dietary score calculation
EDIH and ELIH are empirically derived dietary and lifestyle indices that evaluate insulinemic potential, developed and validated by Tabung et al. 9 Higher scores denote more insulinemic diets or lifestyles, and lower values denote less insulinemic potential. Each food category had a specific weight and a positive or negative influence on the determined score in the calculation of EDIH and ELIH. Red meat, poultry, fish, processed meat, high-energy drinks, margarine, butter, low-fat dairy, French fries, eggs, and tomatoes were all positive determinants of EDIH calculation. On the other hand, green and leafy vegetables, whole fruits, high-fat dairy, and coffee were negative factors. Furthermore, fruit juice, margarine, red meat, butter, and BMI were positive contributors to ELIH calculation. In contrast, high-fat dairy items, physical exercise, snacks, whole fruits, and salad dressing, were negative determinants. We excluded wine and liquor (due to forbidden consumption in Iran) and cream soups (owing to lack of data) from the final calculations.
Biochemical evaluation
The measurement of the anthropometric and biochemical parameters has been previously described. 3 Fasting blood glucose (FBG), triglyceride (TG), serum total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), and insulin concentrations were measured, and low-density lipoprotein cholesterol (LDL-C) levels were determined using the Friedewald equation.
Statistical analyses
SPSS version 26.0 was used to analyze the data, and a significance level of P < .05 was deemed statistically significant. For categorical data, the frequency (%) was noted, and for continuous variables, the mean and standard deviation (SD) were provided. Chi-square and one-way analysis of variance (ANOVA) tests were employed to examine the disparities in discrete and continuous variables among the various tertiles of EDIH and ELIH. The study employed multinomial logistic regression to establish odds ratios (ORs) and 95% confidence intervals (CIs) to assess the presence of risk factors of MetS and to explore the associations between EDIH and ELIH tertiles and various biochemical variables.
Results
Our study included 339 obese and overweight individuals with a mean age and BMI of 40.78 ± 9.23 years, and 32.63 ± 4.81 kg/m2, respectively. Baseline characteristics and anthropometric parameters across different tertiles of EDIH and ELIH are listed in Tables 1 and 2 respectively. Age, weight, BMI, WC, HC, FFM, and BMR significantly differed across tertiles of EDIH. Also, among tertiles of ELIH, age, weight, height, BMI, SES score, WC, HC, and FM were significantly different.
Demographic and anthropometric characteristics of participants across different tertiles of EDIH.

Abbreviations: BMI, body mass index; BMR, basal metabolic rate; FM, fat mass; FFM, fat free mass; HC, hip circumference; WC, waist circumference; WHR, waist to hip ratio.
All data are expressed as mean (±SD).
P-values derived from one-way ANOVA.
Bolded values are statistically significant.
Demographic and anthropometric characteristics of participants across different tertiles of ELIH.

Abbreviations: BMI, body mass index; BMR, basal metabolic rate; FM, fat mass; FFM, fat free mass; HC, hip circumference; WC, waist circumference; WHR, waist to hip ratio.
All data are expressed as mean (±SD).
P-values derived from one-way ANOVA.
Bolded values are statistically significant.
Table 3 shows that systolic blood pressure (SBP) (P = .01), diastolic blood pressure (DBP) (P = .004), and TG (P = .023) were significantly higher in the first tertile of EDIH. After multivariable adjustment, DBP was no more significant. In the first tertile of ELIH, SBP (P = .043) and TG (P = .019) were higher, while FBG was higher in the third tertile (P = .001). After adjustment for multiple variables, SBP (P = .008) and DBP (0.049) were higher in the first tertile, and HDL-C (P = .023) was significantly different across tertiles of ELIH, and no other significant differences were seen (Table 4).
Cardiometabolic parameters of study participants by tertiles of EDIH.

Abbreviations: DBP, diastolic blood pressure; HDL, high density lipoprotein; LDL, low density lipoprotein; SBP, systolic blood pressure; TC, total cholesterol; TG, triglyceride.
All data are expressed as mean (±SD).
All variables were adjusted for demographic characteristics including age, sex, socioeconomic status, and physical activity.
P-values derived from one-way ANOVA.
Bolded values are statistically significant.
Cardiometabolic parameters of study participants by tertiles of ELIH.

Abbreviations: DBP, diastolic blood pressure; HDL, high density lipoprotein; LDL, low density lipoprotein; SBP, systolic blood pressure; TC, total cholesterol; TG, triglyceride.
All data are expressed as mean (±SD).
All variables were adjusted for demographic characteristics including age, sex, socioeconomic status, and physical activity.
P-values derived from one-way ANOVA.
Bolded values are statistically significant.
Dietary intake of ELIH and EDIH components are represented in Tables 5 and 6, respectively. In the first tertile of ELIH, the consumption rate of red meat, high-fat dairy products, whole fruit, fruit juice, and salad dressing was significantly higher. Subjects in the first tertile of EDIH had greater consumption of red meat, whole fruit, green leafy vegetables, and French fries. However, participants in the third tertile of EDIH had a higher intake of processed meat, poultry, eggs, high-energy beverages, and butter.
Consumption rates of ELIH components (serving/1000 kcal).

All data are expressed as mean (±SD).
P-values derived from one-way ANOVA.
All variables were adjusted for dietary energy intake.
Bolded values are statistically significant.
Consumption rates of EDIH components (serving/1000 kcal).

All data are expressed as mean (±SD).
P-values derived from one-way ANOVA.
All variables were adjusted for dietary energy intake.
Bolded values are statistically significant.
The ORs (95% CIs), both crude and adjusted for multiple variables, for MetS risk factors among different tertiles of EDIH and ELIH scores are demonstrated in Tables 7 and 8. Subjects with medium EDIH scores (second tertile) had a reduced chance of developing elevated SBP [OR: 0.979 (0.963-0.996; P < .05)] and DBP [OR: 0.975 (0.953-0.998; P < .05)] in the crude model. Individuals in the third tertile of EDIH had higher ORs of FBG in crude [OR: 1.039 (1.017-1.061; P < .05)] and the model I [OR: 1.035 (1.004-1.068; P < .05)] analyses. Additionally, TG in the second [OR: 0.997 (0.994-1000; P < .05)] and third [OR: 0.996 (0.993-0.999; P < .05)] tertiles of the crude model was inversely associated with EDIH score. No other significant associations were seen in crude and multivariable-adjusted models.
Crude and multivariable adjusted ORs and 95% CIs for cardiometabolic risk factors across different tertiles of EDIH.
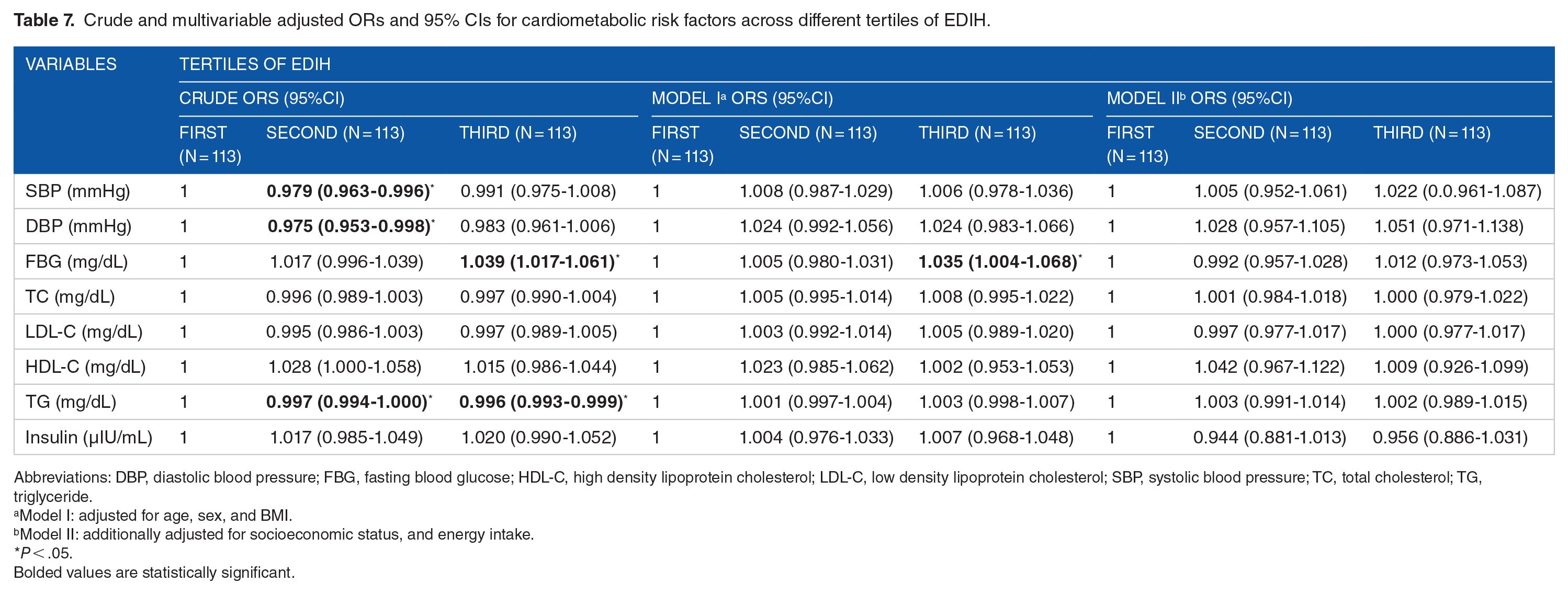
Abbreviations: DBP, diastolic blood pressure; FBG, fasting blood glucose; HDL-C, high density lipoprotein cholesterol; LDL-C, low density lipoprotein cholesterol; SBP, systolic blood pressure; TC, total cholesterol; TG, triglyceride.
Model I: adjusted for age, sex, and BMI.
Model II: additionally adjusted for socioeconomic status, and energy intake.
P < .05.
Bolded values are statistically significant.
Crude and multivariable adjusted ORs and 95% CIs for cardiometabolic risk factors across different tertiles of ELIH.
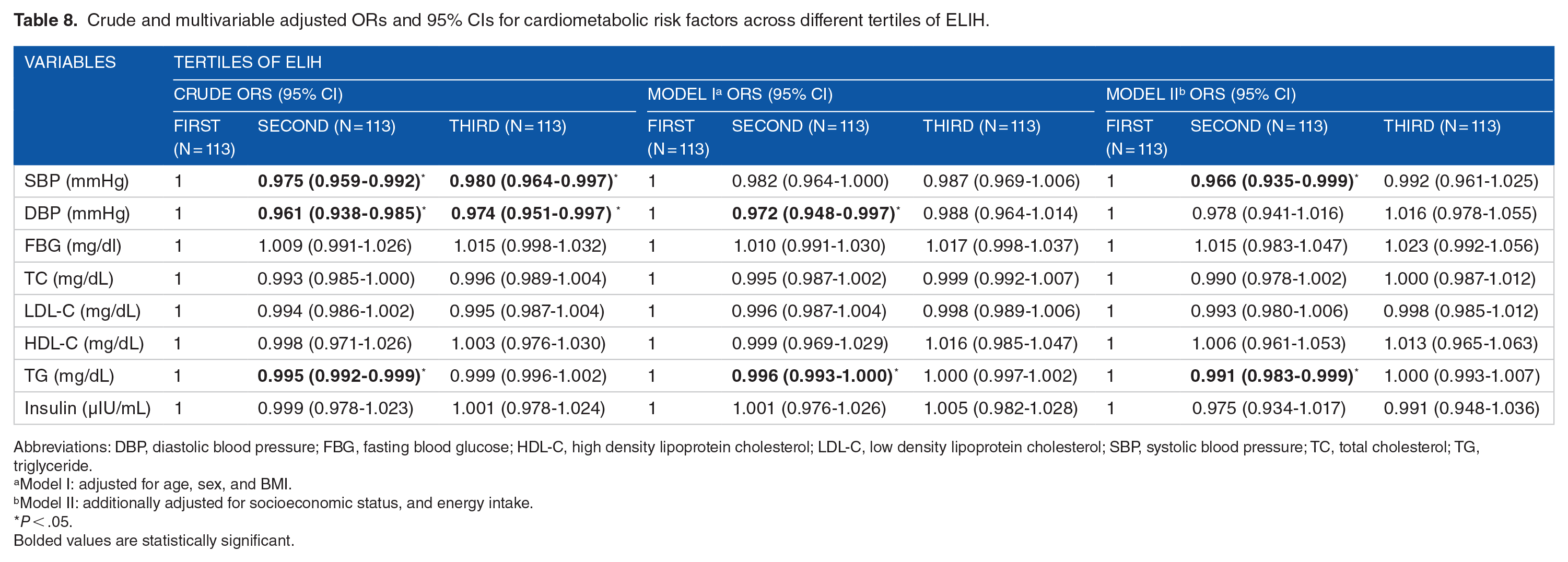
Abbreviations: DBP, diastolic blood pressure; FBG, fasting blood glucose; HDL-C, high density lipoprotein cholesterol; LDL-C, low density lipoprotein cholesterol; SBP, systolic blood pressure; TC, total cholesterol; TG, triglyceride.
Model I: adjusted for age, sex, and BMI.
Model II: additionally adjusted for socioeconomic status, and energy intake.
P < .05.
Bolded values are statistically significant.
SBP had an inverse relationship with the second [OR: 0.975 (0.959-0.992; P < .05)] and third [OR: 0.80 (0.964-0.997; P < .05)] tertiles of ELIH in crude model and was inversely associated with the second tertile of ELIH [OR: 0.966 (0.935-0.999; P < .05)] in multivariable-adjusted model II. Likewise, DBP was inversely associated with ELIH in the second [OR: 0.961 (0.938-0.985; P < .05)] and third [OR: 0.974 (0.951-0.997; P < .05)] tertiles in the crude model, but only in the second tertile [OR: 0.972 (0.948-0.997; P < .05)] in the multivariable-adjusted model I. Individuals in the second tertile of ELIH had decreased risk of hypertriglyceridemia in crude [OR: 0.995 (0.992-0.999; P < .05)] and model I with multivariable adjustment [OR: 0.996 (0.993-0.999; P < .05)] and model II [OR: 0.991 (0.983-0.999; P < .05)].
Discussion
In this cross-sectional study, conducted on Iranian adults with obesity and overweight, we assessed possible associations between the insulinemic potential of diet and lifestyle and risk factors of MetS. Our results demonstrated that higher EDIH and ELIH scores are associated with lower risk of elevated SBP, DBP, and TG levels. In contrast, a greater EDIH score is related to higher odds of FBG. Due to the paucity of research on the relationship of the insulinemic potential of diet and lifestyle with risk factors of MetS, drawing a scientific conclusion from the results poses a significant challenge.
Our findings represented that individuals in the third tertile of EDIH are more likely to have higher FBG. Likewise, Shi et al 32 demonstrated that EDIH is associated with increased glucose concentrations in postmenopausal women. In contrast to our findings, Teymoori et al 40 reported that individuals in the first tertile of the empirical lifestyle index for insulin resistance (ELIR), another score for the insulinemic potential of diet and lifestyle, had higher FBG. Nonetheless, we found that subjects with the lowest ELIH score (first tertile) had decreased FBG concentrations. Mokhtari et al 21 reported that individuals in the lower tertiles of ELIH had lower FBG than other tertiles. Conversely, participants in the lower tertiles of EDIH had higher concentrations of FBG.
In the present study, we observed that the insulinemic potential of diet could be associated with lower odds of TG and moderate insulinemic potential of lifestyle was related to lower odds of TG. In contrast with our findings, Shi et al 32 asserted that a greater EDIH index was related to greater TG concentrations. The study also revealed that a moderate insulinemic potential in both diet and lifestyle was associated with reduced SBP and DBP. However, no study has shown such a relationship or even the opposite.
A shift toward evaluating more complicated food intake patterns relative to disease risk has occurred due to decades-long reductionist approaches to diet and chronic disease research that focused on certain nutrients. 32 Evaluating nutritional intake as a whole diet rather than individual nutrients and food components is vital because it is usually complicated to disentangle the specific effects of a single nutrient or food; people consume a wide variety of foods that may interact or synergize with one another. 41 The EDIH and ELIH indices of dietary and lifestyle choices examine the long-term insulinemic potential of whole diets. 9 EDIH and ELIH both contain food groups with favorable and unfavorable health effects. Nevertheless, there are some food groups with significant impacts on risk factors of MetS which are not part of these indices, and it can be the reason for the differences in the results of this study with few other studies.
Although several studies demonstrated positive associations between the insulinemic potential of diet and lifestyle with different health conditions, as far as our knowledge extends, this study represents the first attempt to explore the link between dietary and lifestyle insulinemic potential and the risk factors associated with MetS. It should be noted that this research was carried out in northwest Iran, which has distinct dietary patterns, and extending the findings to other regions of the nation should be done with caution. Further, any possible measurement errors in the FFQ must be regarded. Although the role of possible confounders was controlled, the potential for confounding may not be removed entirely.
Conclusion
Our research revealed that a higher EDIH score is linked to greater chances of high FBG and lower odds of TG, and a moderate EDIH score was found to be associated with reduced odds of elevated SBP and DBP. Moreover, a moderate ELIH score was found to be associated with reduced odds of TG, and a higher ELIH is associated with lower SBP and DBP. Additional epidemiological investigations are required to explore the potential relationship between the insulinemic impact of diet and lifestyle and the risk factors associated with MetS, as well as to elucidate the underlying mechanisms involved.
Footnotes
Acknowledgements
The authors express their gratitude to all the study participants for their sincere cooperation. Additionally, the authors extend their thanks to the Research Undersecretary of Tabriz University of Medical Sciences for their financial support (Grant number: 74940).
Author Contributions
AH wrote the first draft of the manuscritp and performed the statistical analysis, MAF supervised the project and was involved in writing, analysising and revsing the mauscript. MAF was also invloved in data collection and hypothesis generation. Data validation and visulaization was perofrmed identically by both authors.
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study received a grant from the Research Deputy of Tabriz University of Medical Sciences (Grant number: 74940).
Ethical Clearance and Participant Informed Consent
Prior to their participation in the study, all subjects submitted a written informed consent. The study protocol was reviewed and approved by the ethics committee of Tabriz University of Medical Sciences (Registration number: IR.TBZMED.REC.1396.768 and IR.TBZMED.REC.1398.460). The study methods were carried out in accordance with the guidelines and regulations outlined in the Declaration of Helsinki. Written informed consent was obtained from the legal guardians of participants who were unable to provide consent due to illiteracy.