
Abstract
Objective:
Osteoarthritis (OA) as a common musculoskeletal disorder is the main cause of disability in the world. The present study aimed to evaluate the effects of pomegranate peel extract (PPE) on some inflammatory markers and matrix maloproteinase1 (MMP1) in women with knee OA.
Methods:
Sixty obese women with knee OA aged 38 to 60 years were included in this clinical trial. The women were allocated into intervention (n = 30) and placebo (n = 30) groups along with standard drug therapy receiving 500 mg PPE or placebo twice daily for 8 weeks, respectively. Three-day food records, anthropometric measurements, fasting blood samples, and physical activity questionnaires were gathered at the baseline and the end of the study.
Results:
The supplementation of PPE significantly reduced the serum high-sensitivity C-reactive protein (hs-CRP), nuclear factor kappa-light-chain-enhancer of activated B cells (NF-ĸB), MMP1, and monocyte chemoattractant protein-1 (MCP-1) levels of the patients within the intervened group (all, P < .05) and compared with the placebo (P = .002, .045, .040, and .003, respectively) at the end of the study. The serum NF-ĸB levels significantly increased within the placebo group at the end of the trial (P = .002). Changes in other variables in the placebo group were not significant (P > .05).
Conclusions:
The findings of this clinical trial indicated that PPE supplementation decreased serum inflammatory markers including hs-CRP, NF-ĸB, and MCP-1 and MMP1 levels in women with knee OA. PPE supplementation may be useful as a part of an integrated approach to modulating inflammatory complications in women with knee OA.
Keywords
Introduction
Osteoarthritis (OA) is the most prevalent musculoskeletal disorder and the main cause of disability around the world. 1 It is a complex clinical syndrome with chronic, painful, and disabling conditions that have a major impact on patients’ function and quality of life. 2 OA is more prevalent in the elderly population and women and the knee joints are the most affected, especially in women. 3 The global prevalence of knee OA in population-based studies was 16%. 4 In Iran, the prevalence of knee OA has been estimated at around 17%. 4
OA leads to articular cartilage erosion, subchondral bone resorption, and synovial membrane inflammation. 5 Inflammation contributes to the OA symptoms such as morning and inactivity stiffness, joint local warmness, tenderness, effusions, and pain. These pathological alterations are connected with extreme production of proinflammatory parameters such as high-sensitivity C-reactive protein (hs-CRP), nuclear transcription factor ĸB (NF-ĸB), interleukin-1β (IL-1β), tumor necrosis factor-α (TNF-α), and interleukin 8 (IL-8), and matrix metalloproteinase (MMP)-1 and MMP-13. Pro-inflammatory cytokines cause apoptosis and oxidative stress in OA. 6 Moreover, matrix metalloproteinases (MMPs) modulate extracellular matrix turnover.5,7,8 and disarrange the balance between degradation and synthesis of matrix components induces progressive joint destruction. 5
Various factors affect the pathophysiology of knee OA such as aging, knee injury, female gender, bone density, muscle weakness, overweight and obesity, and diet.9-11 Observational studies demonstrated that a higher intake of vegetables, plant-based foods, fruits, dietary fiber, and whole grains might reduce the odds of the development of knee OA.12-15 Recent studies reported a relationship between dietary polyphenols and decreasing the severity of OA complications.16,17
Pomegranate (Punica granatum L,) is one of the medicinal fruits and its peel and pulp are rich in soluble polyphenols, organic acids, and tannins. Several studies indicated the antioxidant and anti-inflammatory potential of the pomegranate components’ active ingredients.18,19 Pomegranate peel contains considerable amounts of phenolic compounds such as hydrolyzable tannins (punicalin, gallic, punicalagin, pedunculagin, and ellagic acid) and flavonoids (anthocyanins, catechins, and other complex flavonoids). 20 The pomegranate peel extract (PPE) comprises 10 times higher antioxidant activity, total flavonoid, and phenolic contents compared to the pulp extract. 21 Some findings suggested that PPE stimulated type I procollagen synthesis and inhibited the MMP-1 and monocyte chemoattractant protein-1 (MCP-1) production by dermal fibroblasts.22,23 MMP-1 modulates the turnover of extracellular matrix to speed up cartilage degradation and MCP-1 is a member of the beta chemokine family that its expression has been observed in chondrocyte degradation and disease progress of knee OA.24,25
Considering that, inflammation has a critical role in OA pathogenesis, PPE may attenuate related risk factors in OA. To our best knowledge, no study is available about the effects of PPE in this context in OA. Therefore, this clinical trial was performed to investigate the effects of PPE supplementation on some serum inflammatory biomarkers including hs-CRP, NF-ĸB, and MCP-1 and MMP-1 levels in women with knee OA.
Materials and Methods
Study design and subjects
The present randomized, double-blind placebo-controlled clinical trial was carried out among 66 women aged 38 to 60 years who attended the physical medicine and rehabilitation department in Tabriz, Iran. Reporting of the study was performed by adhering to the CONSORT guidelines. Individuals with mild to moderate knee OA were selected by considering the American College of Rheumatology criteria 26 by a convenience sampling method for this study. Women with body mass index (BMI) <30 kg/m2 or >35 kg/m2, liver and kidney diseases, diabetes mellitus, cardiovascular disease, any history of duodenal or peptic ulcers, intake non-steroidal anti-inflammatory drugs, smoking, take multivitamin-mineral, alcohol intake, having an allergy to pomegranate, or use of any other supplements during the study (8 weeks) and 4 weeks before the trial were excluded of this study.
The sample size concerning Babaeian et al. 27 reports for the serum hs-CRP concentration (mean ± SD) and considering α = 0.05, a confidence interval of 95%, and power of 80% were calculated to be 30 patients with knee OA per group. Finally, assuming a 10% dropout rate, 33 patients were considered for each group.
The patients were randomly allocated the groups via a block randomization technique created using the random allocation software (RAS). A flowchart of enrollment and follow-up of the participants is shown in Figure 1. All participants were matched for age and BMI and every 5 subjects was assigned to each group of the trial. An individual who had no clinical involvement in this study carried out the allocation, to maintain blinding.

Flow chart of the study.
The Ethics Committee of the Tabriz University of Medical Sciences approved the protocol of the current study (reference number: 9328, date: 2014-05-11). Also, the Iranian Registry of Clinical Trials registered it with the number IRCT201405183664N11. The current clinical trial was conducted considering the Helsinki guidelines. All patients were informed of the study procedure and before clinical trial enrolment signed a written informed consent. This research is part of a comprehensive study, in which data about the results of PPE on metabolic and other risk factors and clinical symptoms of participants has been published in advance.28-30
Extraction Procedures
Pomegranate was provided in Shiraz–Iran from December 2013 to February 2014. Three hundred Kg of pomegranate peels after juicing were manually separated and kept at 4°C. Pomegranate peel was dried by a vacuum 25 mmHg oven at 40°C to about 5% moisture content (dry basis). Then, dried peels were ground and extracted by the maceration method and ethanol-water 80%. The extract was filtered by a large Whatman paper NO.41 and then to remove all the particles another filtration was carried out using a Whatman paper NO.42. The clear extract was dried under a vacuum at 50°C to obtain a fine brown powder. Five hundred mg of this powder (PPE) was encapsulated along with 50 mg of rice flour. The capsule placebo was filled with 550 mg of rice flour equal in size and color to the pomegranate pericarp extract capsule.
The extract ellagic acid content, as a polyphenol component of PEE, was analyzed in comparison to standard ellagic acid (Sigma, ⩾95%). The results of the analyses revealed that this extract on a dry basis contained 90% ellagic acid confirmed using the high-performance liquid chromatography analysis. 31
Supplementation
Participants of the intervention and placebo groups received 2 capsules daily of PPE (500 mg PPE twice per day) and the placebo, respectively, with their meals for 8 weeks. Moreover, standard drug therapy including 1 glucosamine 500 mg/day and acetaminophen 500 mg twice per day was administrated. Primary outcomes were serum Nf-ĸB or hs-CRP and the secondary outcomes were serum MCP-1 and MMP1. All data were kept by code and the physician, statistician, and investigator reminded blind until the end of the study. The patients, data analyzer, and evaluating physician were unaware of the groups and drug packs. All participants were instructed to keep their usual physical activity and diet during the study. Participants were followed up by bi-weekly visits and phone calls. Patients were asked to return all empty or filled packs to evaluate compliance and the status of supplement consumption. Participants were included in the final statistical analyses if consumed more than 90% of capsules.
The Assessments of Anthropometric, Dietary, and Physical Activity Levels
Body height and weight were measured using a mounting tape and calibrated Seca scale to the nearest 0.5 cm and 0.1 kg, respectively. BMI was obtained by dividing the weight in kilograms by the square of height in meters.
Dietary intake was evaluated by 3 food records of nonconsecutive days (1 weekend and 2 weekdays) at the baseline and end of the study. At the beginning of the trial, all participants were instructed on how to record their food intakes using a food scale. The average energy and macronutrient intakes for 3 days were analyzed via nutritionist 4 software.
To evaluate the physical activity of participants was used of a short International Physical Activity Questionnaire (IPAQ). IPAQ was designed and validated primarily for adults aged 15 to 69 years. 32 The physical activity levels of the participants were obtained with consideration of the energy requirements defined in metabolic equivalent (METS). The patients based on their physical activity levels were classified into 3 groups including low, moderate, and high physical activity levels.
Blood Sampling and Biochemical Measurements
Of all patients, a 10 ml fasting blood sample was achieved. Then, the samples were centrifuged and the serum was separated and immediately stored at −70°C. Serum NFĸB and MCP-1 levels were measured via enzyme-linked immunosorbent assay by a commercial kit (Hangzhou Eastbiopharm Co., LTD, China). Serum hs-CRP levels were obtained via immunoturbidimetric method 33 by a Biosystem kit (Biosystem, SA, Spain) and the active MMP1 of serum was quantified using the Human MMP-1 Enzyme immunoassay kit (Boster Biological Technology LTD, USA). All measurements of the patients, at the beginning and at the end of the study, were done by the same physician.
Statistical Analysis
Statistical analysis was performed by the SPSS software version 13.0. Ordinal and continuous variables were reported as median (interquartile range) (MED (IQR)) and mean ± standard deviation, respectively. For assessing the normality of the data distribution was used of the one-sample Kolmogorov–Smirnov test. Pre- and post-treatment differences in mean values among each group were obtained using the paired t-test or Wilcoxon test. An independent t-test or Mann–Whitney U test was used for analyzing the differences in mean values between the intervention and placebo groups. To compare the post-treatment values with adjustment for baseline values, energy intake, weight changes, disease duration, physical activity, and parity were used in the ANCOVA test. Statistically significant was recognized by a P-value < .05. The percentage change of each variable was calculated as follows: [(after mean value to before mean value)/before mean value] × 100.
Results
Thirty participants per group accomplished the study (Figure 1). Patients did not report adverse effects and supplements were intakes with high compliance (97%). The general characteristics of the participants are shown in Table 1. Weight, BMI, age, parity, and disease duration were not significantly different between the 2 groups at baseline (P > .05).
Baseline characteristics of women with knee OA.

Abbreviations: BMI, Body mass index; CI, Confidence interval; MD, Mean difference; OA, Osteoarthritis; PPE, Pomegranate peel extract.
Data are presented as mean ± standard deviation (SD). Disease duration is presented as median (interquartile range)
P < .05, Unpaired student t-test.
P < .05, Mann-Whitney test for disease duration.
The daily dietary intakes of subjects are presented in Table 2. There was a significant difference between the 2 groups in carbohydrate intake before and after intervention (P = .000 and P = .004, respectively). No significant changes were seen during the study in total energy, protein, and fat intakes in the groups (P > .05). The physical activity levels of the 2 groups were not significantly different before and after the intervention (P > .05) (Data are not presented).
Dietary energy and macronutrients intakes of women with OA at baseline and after 8 weeks intervention.

Abbreviations: CI, Confidence interval; MD, Mean difference; OA, Osteoarthritis; PPE, Pomegranate peel extract.
All values are presented as mean ± SD.
P < .05, paired t-test.
P < .05, independent t-test.
The serum hs-CRP, NF-ĸB, MCP-1, and MMP-1 levels before and after the trial are shown in Table 3. At the beginning of the study, no significant differences were found between the PPE and placebo groups for all variables (P > .05).
Serum inflammatory biomarkers and MMP-1 of women with OA at baseline and after 8 weeks intervention.
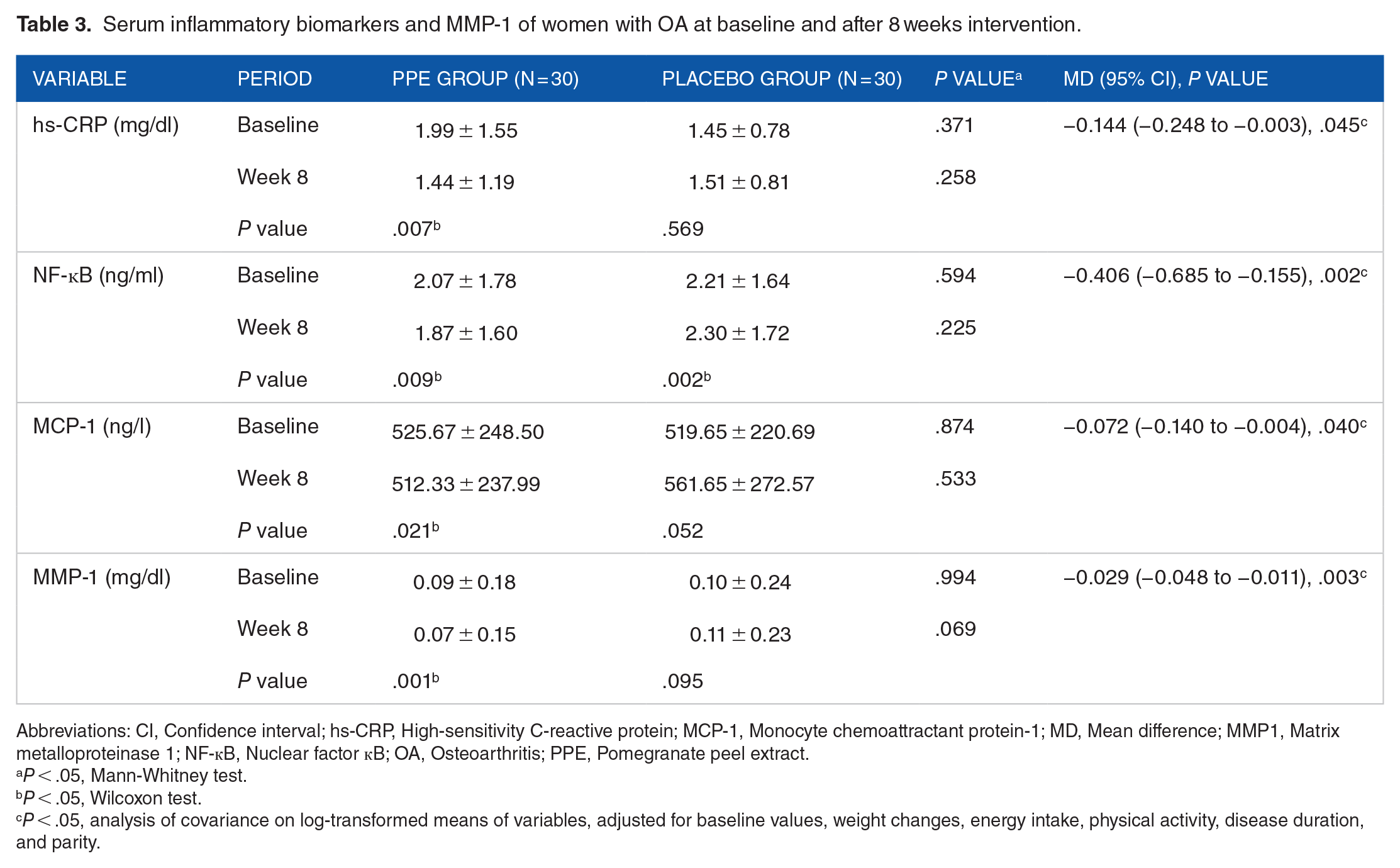
Abbreviations: CI, Confidence interval; hs-CRP, High-sensitivity C-reactive protein; MCP-1, Monocyte chemoattractant protein-1; MD, Mean difference; MMP1, Matrix metalloproteinase 1; NF-ĸB, Nuclear factor ĸB; OA, Osteoarthritis; PPE, Pomegranate peel extract.
P < .05, Mann-Whitney test.
P < .05, Wilcoxon test.
P < .05, analysis of covariance on log-transformed means of variables, adjusted for baseline values, weight changes, energy intake, physical activity, disease duration, and parity.
The serum levels of hs-CRP (by 38.19%, P = .007), NF-ĸB (by 10.69%, P = .009), MCP-1 (by 2.60%, P = .021), and MMP-1 (by 28.57%, P =.001) significantly reduced in the post-treatment compared with the baseline values in the PPE group. A significant enhancement was detected in the serum levels of NF-ĸB within the placebo group after intervention (P = .002). Changes in other variables were not significant in this group (P > .05).
After adjusting for covariances including baseline values, physical activity, weight changes, energy intake, disease duration, and parity, a significant decrease in the serum levels of hs-CRP (P = .002), NF-ĸB (P = .045), MCP-1 (P = .040), and MMP-1 (P = .003) were found between 2 groups at the end of the study.
Discussion
Nutraceuticals are gaining more and more importance as a complementary treatment for osteoarthritis, especially, knee OA.34-36 The main pathological characteristics of OA are connected with the excessive production of proinflammatory molecules which lead to the initiation and progression of OA. 37 The current study is the first randomized clinical trial investigating the effects of PPE supplementation on some inflammatory biomarkers and MMP-1 levels in women with knee OA.
Based on the findings, 8-week supplementation with PPE decreased the serum hs-CRP, NF-κB, and MCP-1 levels in women with knee OA. Effects of different components of pomegranate on markers of inflammation have been investigated in other diseases. In the studies by Hosseini et al. and Sohrab et al. consumption of 1000 mg of whole pomegranate extract and 250 ml/day of pomegranate juice by overweight and obese individuals and patients with type 2 diabetes for 30 days and 12 weeks lowered IL-6 and hs-CRP levels, respectively.18,19 Ghoochani et al. reported that after 6 weeks of consuming 200 ml/day of pomegranate juice, serum IL-1ß and TNF-α levels did not have significant alterations in patients with knee OA. 38
An animal study showed that supplementation of PPE over 4 weeks in high-fat diet-induced obese mice, counteracted the expression of inflammatory factors such as IL-1 and IL-6 in the colon and visceral adipose tissue. 25 Several in vitro and in vivo assays also reported that phenolic components of pomegranate such as punicalin, punicalagin, strictinin A, granatin B, and ellagic acid are a very effective treatment for inflammatory disorders.39-41 Rasheed et al. 42 indicated that PPE inhibited the production of pro-inflammatory cytokines by suppressing the gene expression and blocking the mitogen-activated protein kinase and activation of NF-κB in cells. Shukla et al. also demonstrated that PPE inhibited the activation of the NF-κB by endotoxin in mice macrophages. Detecting the low IL-6 levels in the arthritic joints of mice that feed with pomegranate extract compared to the control group was attributed to the inhibitory effect of pomegranate on NF-κB activation. 43 Chao et al. also revealed that some of the pomegranate polyphenols such as caffeic acid and ellagic acid which are abundant in pomegranate peel downregulated MCP-1 and TNF-α mRNA expression in the kidneys of diabetic mice. 23
Inflammatory cytokines lead to irreversible joint damage, which is seen in OA, via up-regulating gene expression of metalloproteinase, stimulating the production of reactive oxygen species, altering the metabolism of the chondrocyte, and possibly increasing osteoclastic bone resorption.7,8,34 Inflammatory cytokines also have a role in connective tissue degradation through stimulating collagenase. 44 Further inflammation and cartilage degradation lead to scarring, thinning, and erosion of the articular cartilage and progression of OA 2 that manifests as joint pain, loss of function, and disability. 44 Of downstream signaling pathways stimulated by the inflammatory factors, the pathway of NF-κB is the central regulator of events that trigger OA. Activation of NF-kB causes various pro-inflammatory cytokines secretion such as TNF-α and IL-6 which trigger the production of CRP by the liver.45,46 Thus, the suppression of NF-ĸB expression consequently reduces various pro-inflammatory such as hs-CRP which is an acute phase protein and indicator of systemic inflammation. 47 Inhibition of the activation of transcription factor NF-κB and other inflammatory cytokines are the major effects of the pomegranate extract. 48 The anti-inflammatory components of PPE such as punicalin, granatin B, punicalagin, and strictinin A significantly reduced the production of prostaglandin E2 and nitric oxide via inhibiting the expression of the pro-inflammatory proteins in the macrophage cells.20,40 This evidence suggested novel pharmacological actions of pomegranate extract for the treatment of OA and other inflammatory and degenerative diseases.42,49
Our results confirmed the impact of PPE on ameliorating inflammation in studied patients. Mechanisms mentioned above might have contributed to lowered serum hs-CRP, NF-κB, and MCP-1 levels in our studied subjects.
MMPs, a family of collagenases degrade various components of extracellular matrix and non-extracellular matrix molecules. 50 The irreversible breakdown of the cartilage matrix through type-II collagen digestion and consequent matrix proteoglycan release from the cartilage is the pivotal event in the OA progress. 51 Our findings indicated that supplementation with PPE diminished the serum levels of MMP1. Such effective impacts were determined in other investigations. Ghoochani et al. showed that taking 200 ml pomegranate juice for 6 weeks led to reducing the breakdown of cartilage enzyme MMP-13 in knee OA patients. 52 Some similar findings suggested that PPE inhibited the production of MMP-1 by dermal fibroblasts which have a very important role in the damage of cartilage and the repairment cycle in OA.22,53 Garbacki et al. 54 also reported that anthocyanins as a component of PPE had a positive regulatory impact on proteoglycan and collagen-II synthesis. Polyphenols are shown to reduce levels of MCP-1 and inhibit the expression of MMPs24,25 thus, are potential candidates for the treatment of many diseases such as OA. 55 A study using human chondrocytes demonstrated that pomegranate fruit extract inhibited IL-1-induced expression of MMP-1, -3, and -13 by inhibiting the activation of the mitogen-activated protein kinase and NF-ĸB 53 Suppressing the MMP expression in OA chondrocytes suggests that pomegranate ingredients inhibit collagen degradation and can prevent joint destruction in subjects with OA.56,57 As explained previously, Nf-kB induces up-regulation of many inflammatory mediators like MCP-1 and metalloproteinases especially MMP-1 and -13. Reduced MMP-1 and MCP-1 levels in our intervened group might have been mediated in part through lowered NF-κB levels which were detected in our study. Furthermore, lowered MCP-1 might also have been involved in reducing MMP-1 in our study. MCP-1 has a vital role in the inflammation process via increasing the infiltration and migration of inflammatory cells like monocytes/macrophages and cytokines at the inflammation site or enhancing the expression of other inflammatory factors and MMP-1. 58
It should be noted that, based on the results, the physical activity levels and diet of the participants were not changed between the groups at the end of the study. Thus, these variables have no confounding impact on the obtained results.
A relatively small sample size and a short study duration of 8 weeks were some limitations of this study. Moreover, our study was only on women and the results may not applicable to males. Other studies are warranted to evaluate the effectiveness of PPE on other indicators of inflammation such as TNF-α, IL-1, IL-1β, IL-6, and MMP-3, -9, and -13 and their related mechanisms among both genders.
Conclusions
Our findings demonstrated that PPE supplementation reduced serum hs-CRP, NF-ĸB, MCP-1, and MMP-1 concentrations in knee OA women. PPE may be of value as a natural complementary medication for OA. Further studies are required to assess the effects of PPE with different doses and duration use on other aspects of inflammation in OA.
Footnotes
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was approved and supported by the vice-chancellor and the Nutrition Research Center of Tabriz University of Medical Sciences, Tabriz, Iran. This article was written based on a data set of PhD thesis, registered in Tabriz University of Medical Sciences, Iran.
Data Availability Statement
All data are available upon request of the corresponding author [