
Abstract
Objective:
The study was aimed at assessing the self-care practices and the associated socio-demographic variables of persons with T2DM in South East, Nigeria.
Methodology:
A cross-sectional study involving 382 persons with T2DM proportionately selected from 4 tertiary health institutions in South Eastern, Nigeria. Data was collected using the Summary of Diabetes Self-Care Activities (SDSCA) and a researcher-developed questionnaire. The questionnaire was administered to persons with T2DM who attended a diabetic outpatient clinic. Data collected was analyzed in frequency percentage. Responses on SDSCA were ranked and rated as poor, moderate, and good self-care behavior. The level of significance was placed at P < .05.
Result:
The majority of the participants were within the age groups of 40 to 59 (46.9%) and 60 and above (46.9%); the majority (74.6%) were married while a good proportion were traders (59.7%). Also, the majority of participants (81.2%) were on oral hypoglycemic agents. Findings further showed that a good proportion (51.3% and 89.8%) of study participants had good self-care behavior in diet and medication domains respectively. Whereas the proportion of participants with poor self-care behavior was very high in foot care (75.1%) and fairly high in both self-blood sugar testing (37.7%) and exercise (37.2%) domains. Only 7.9% practiced 3-monthly laboratory blood glucose testing while 16.5% went for eye checks every 6 months.
Conclusion:
Individuals with diabetes mellitus have poor self-management behavior in most domains of the self-management practice. Age, gender, marital status, educational level, and occupation significantly influenced self-management practices. Hence nurses and health educators should take diabetes self-management education very seriously to help diabetes sufferers improve their self-management behavior.
Introduction
Diabetes mellitus is one of the major global health problems of modern society which affects both developed and developing countries. 1 Diabetes mellitus is not only assuming a pandemic proportion worldwide but is also poised to affect the developing countries of the world much more than their developed counterparts. 2 More than 80% of diabetes-related deaths occur in low and middle-income countries. 3 Nigeria is one of such developing countries that is not exempted from the burden of diabetes as demonstrated by the prevalence of diabetes in Nigeria. 4 Nearly half a billion (425 million) adults were estimated to be living with diabetes globally in 2017 and this will increase to 627 million by 2045 (IDF 5 ). The available record revealed the prevalence of diabetes in Nigeria to be within 8%-10% with close to 4 million cases.
Previous studies have posited that the progressive increase in the prevalence rates of diabetes is associated with lifestyle changes, overweight/obesity, physical inactivity, alcohol consumption, dietary changes, and cigarette smoking which are potentially modifiable factors.1,6 The American Diabetes Association (ADA) classified diabetes into 4 categories namely: Type 1 diabetes previously known as Insulin Dependent or juvenile Diabetes Mellitus (IDDM), Type 2 diabetes previously referred to as Non-Insulin Dependent Diabetes Mellitus (NIDDM), Gestational diabetes and other forms of diabetes mellitus. 7 Of the 4 types of diabetes, type 2 is the commonest affecting more than 85% of the diabetic population. 5 Diabetes is a chronic condition that is associated with a high risk of macro and microvascular complications and these chronic complications are responsible for high morbidity and mortality of the disease and significantly affect the Quality of life of persons with diabetes. Diabetes also exerts a huge financial burden on individuals, families, communities, and the healthcare system as observed in a previous. 8 This also affects the Quality of life of persons with DM.
As a chronic disease with chronic complications, diabetes sufferers are often faced with the challenge of short-term and long-term complications associated with frequent readmissions increasing length of hospital stays, and death. 9 One way to prevent frequent re-admission and early development of complications is to ensure that individuals with diabetes have adequate knowledge and ability for self-management. Self-management refers to a set of skilled behaviors engaged in managing one’s illness. 10 Successful self-management of DM requires that individuals with DM frequently monitor their blood glucose levels and take the required action to keep blood sugar within a physiological level, adhere to a prescribed diet, exercise, take medication, and practice foot care daily. 5 They are also expected to monitor their blood pressure once or more per week, monitor blood glucose in the laboratory (glycated hemoglobin—HbAIC) every 3 months, go for eye checks every 6 months, be able to use standard healthcare services for diabetes management and consult the healthcare provider at least every 3 months in the absence of symptoms. 11 It has been observed that the ability to manage one’s diabetes positively significantly predicts the quality of life and helps to achieve better glycemic control. Hence, the a need to assess the self-management practices of diabetic individuals. 12
Clinical trials and reviews have confirmed the role of self-management in reducing blood glucose and improving quality of life.13,14 However, adherence to self-management is still an issue among diabetic patients worldwide.15,16
Many factors have been reported to affect self-management practices as revealed in literature. Among these factors are: Socio-economic, 17 diabetes knowledge/education,1,18,19 health belief, 20 social support 21 and Self-efficacy.18,22 Socio-demographic variables were also reported to influence self-management and they are gender, 23 and level of education. 24 The current study is aimed at assessing self-care practices and the associated socio-demographic variables of diabetic persons in South East, Nigeria. This was because no such study has been conducted in South East Nigeria, and the current study was intended to fill the gap in this area of knowledge in the South East part of Nigeria.
Methodology
A cross-sectional study involving 382 persons with T2DM was proportionately selected from 4 tertiary health institutions in South East, Nigeria. However, the one tertiary health institution that served as the study site from the 4 participating states in South East Nigeria was chosen using a convenience sampling technique. An instrument for data collection was the Summary of Diabetes Self-Care Activities Scale (SDSCA) and a researcher-developed questionnaire. The SDSCA contains 5 scales with 16 question items that assess self-care activities of persons with diabetes in the following areas: Diet, Exercise, Self-blood glucose monitoring (SBGM), taking of medications (insulin or oral hypoglycemic agent), and foot care. These are areas of daily self-care activities for individuals with diabetes mellitus. The researcher-developed questionnaire contains questions on laboratory blood glucose monitoring (Glycosylated hemoglobin [HbAIC] monitoring), blood pressure monitoring, prevention of hypoglycemia, eye check, and use of healthcare which are not daily self-care activity rather than other aspects of the diabetes self-care behavior was used to collect data. Hence they are not contained in the scale mentioned above. The self-developed questionnaire was tested for content validity by 3 research experts and a content validity index (CVI) score of 100% was assigned after the questionnaires. The purpose of the CVI test was to establish the appropriateness of the questionnaire items as per the subject matter. The SDSCA questionnaire is a standardized instrument with an established validity. The reliability of the instrument was further tested by administering the instrument to 30 T2DM persons from a tertiary health institution with similar characteristics but outside the selected tertiary health institutions used for the study. The Data collected was analyzed using Cronbach alpha (α) statistics. The reliability result of α .895 was obtained
The questionnaire was administered to persons with T2DM who attended diabetic out-patient clinics in the tertiary health institutions in South East, Nigeria after obtaining informed consent (the consent form was in English language), and observing other ethical considerations such as confidentiality, and respondents’ autonomy. However, before the administration of the informed consent document, the details of the study were explained to the participants so that they would be able to decide whether they wanted to participate in the study or not. It took between 5 and 10 minutes to fill out the questionnaires. The data collection was collected only on diabetic clinics and it lasted for 10 weeks. Two research assistants were recruited from each study center and were trained on the purposes and objectives of the study for 3 days to assist in the distribution and collection of the questionnaires. The research assistants were senior nurses who worked in the selected diabetic clinics and were familiar with those participants. Only the English version of the questionnaire was used by the researchers as a linguist who is proficient and fluent in both English and Igbo languages was employed in each of the study sites to translate the questionnaire for the participants who could not understand the English language.
Inclusion criteria
Patients with T2DM of more than 1 month of diagnosis, both male and female diabetics individuals whether married, single, widowed, divorced, or separated. T2DM persons who understand English or Igbo language and T2DM persons who were available met the inclusion criteria and were willing to participate in the study.
Exclusion criteria
T2DM persons who were very ill, mentally unstable, pregnant diabetic women, and those aged 18 years and below were excluded from the study.
Sample size determination
The target population comprised all individuals with T2DM who accessed care from diabetic clinics in the tertiary health institution in South Eastern, Nigeria for 6 months to 1 year and it was estimated at 12 710. Sample size calculation was done using the sample size calculation formula by Fox, Hunn, and Mathers, 2009. A sample size of 373 was obtained. Also, Power Analysis was employed, and the same sample size of 373 was obtained. A 10% attrition was added to give 410. However, the return rate was not 100%, hence data analysis was done based on 382 returned and correctly filled questionnaires.
Zero (0) represents no performance of self-care and it is rated as 0 A mean score of 0.1 to 2.99 was ranked 1—Poor performance A mean score of 3 to 4.99 was ranked 2—Moderate performance A mean score of 5 - 7 was ranked 3—Good self-care performance.
Results
Table 1 shows that most of the participants were within the age groups of 40 to 59 (46.9%) and 60 and above (46.9%); the majority (74.6%) were married, 41.6% had secondary school education, while a good proportion were traders (59.7%). Also, the majority (81.2%) of study participants were on oral hypoglycemic drugs.
Socio-demographic characteristics of study participants. n = 382.

The health status of participants is summarized in Table 2. More than half (53.7) of the study participants had eye problems which resulted mostly from aging (22.3%) and diabetes (19.9%). Also, more than half (60.7%) of participants had high blood pressure and more than half (57.9) were on medication for it.
Showing participants health status.
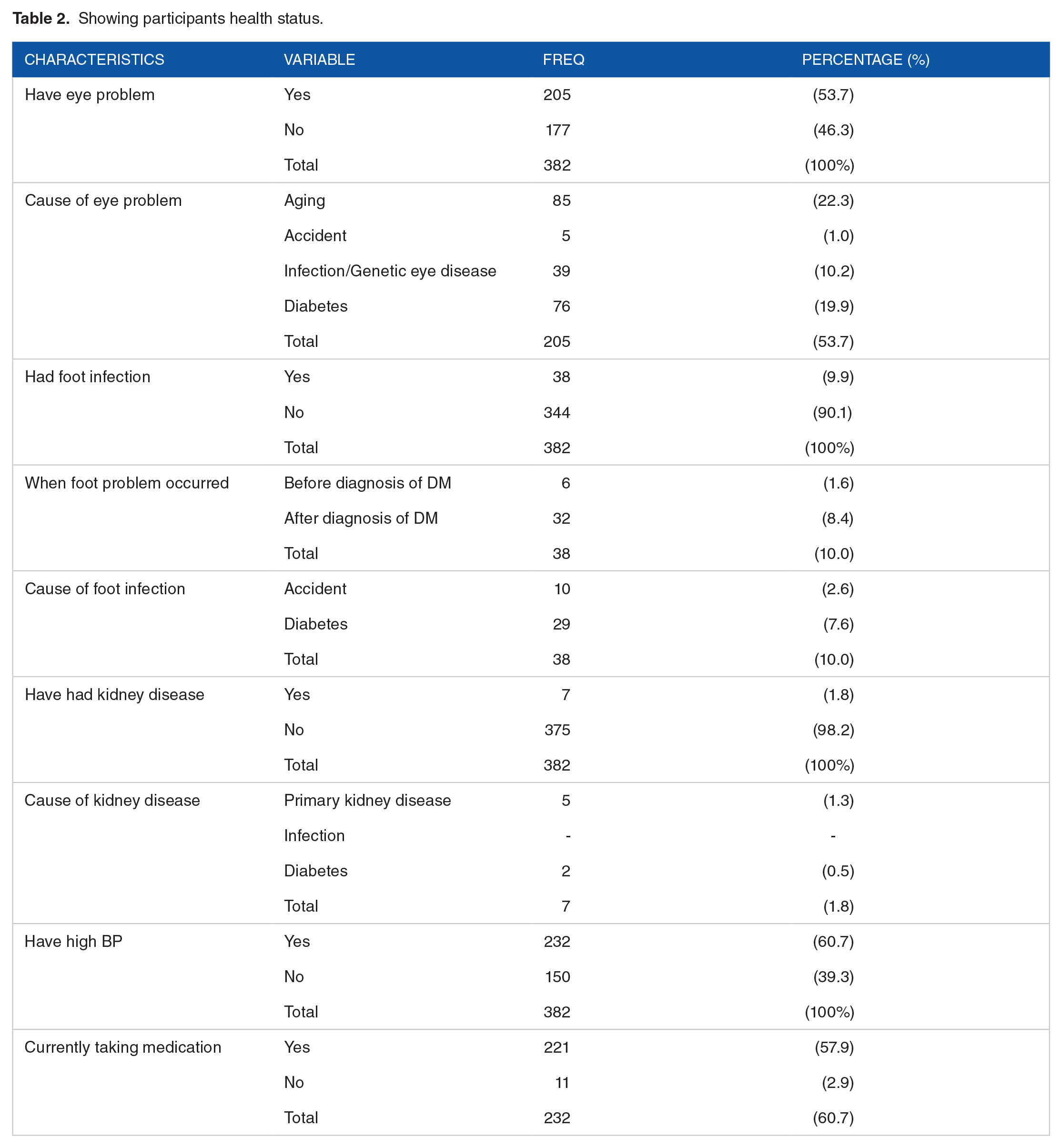
Table 3 shows that the performance of study participants in the self-care activities scale showed a good proportion (51.3% and 89.8%) of study participants had good self-management behavior in diet and medication domains respectively. Whereas the proportion of participants overall with poor self-care behavior was very high in foot care (75.1%) and fairly high in both self-blood sugar monitoring (37.7%) and exercise (37.2%) domains.
Self-management practices of participants.

The level of performance of persons with diabetes in other self-care activities showed that only 7.9%, 57.6%, 48.4%, and 51.8% of all participants monitored their blood glucose in the laboratory once every 3 months; regularly check their BP, the BP check once or more per week and had checked within the previous 1 week before data collection. The proportion of participants who go for eye checkups once in 6 months (16.5%) or go to the hospital for DM consultation once in 3 months (14.1%) was also rather small. Table 4
Self-management practices of participants in some other self-care activities.
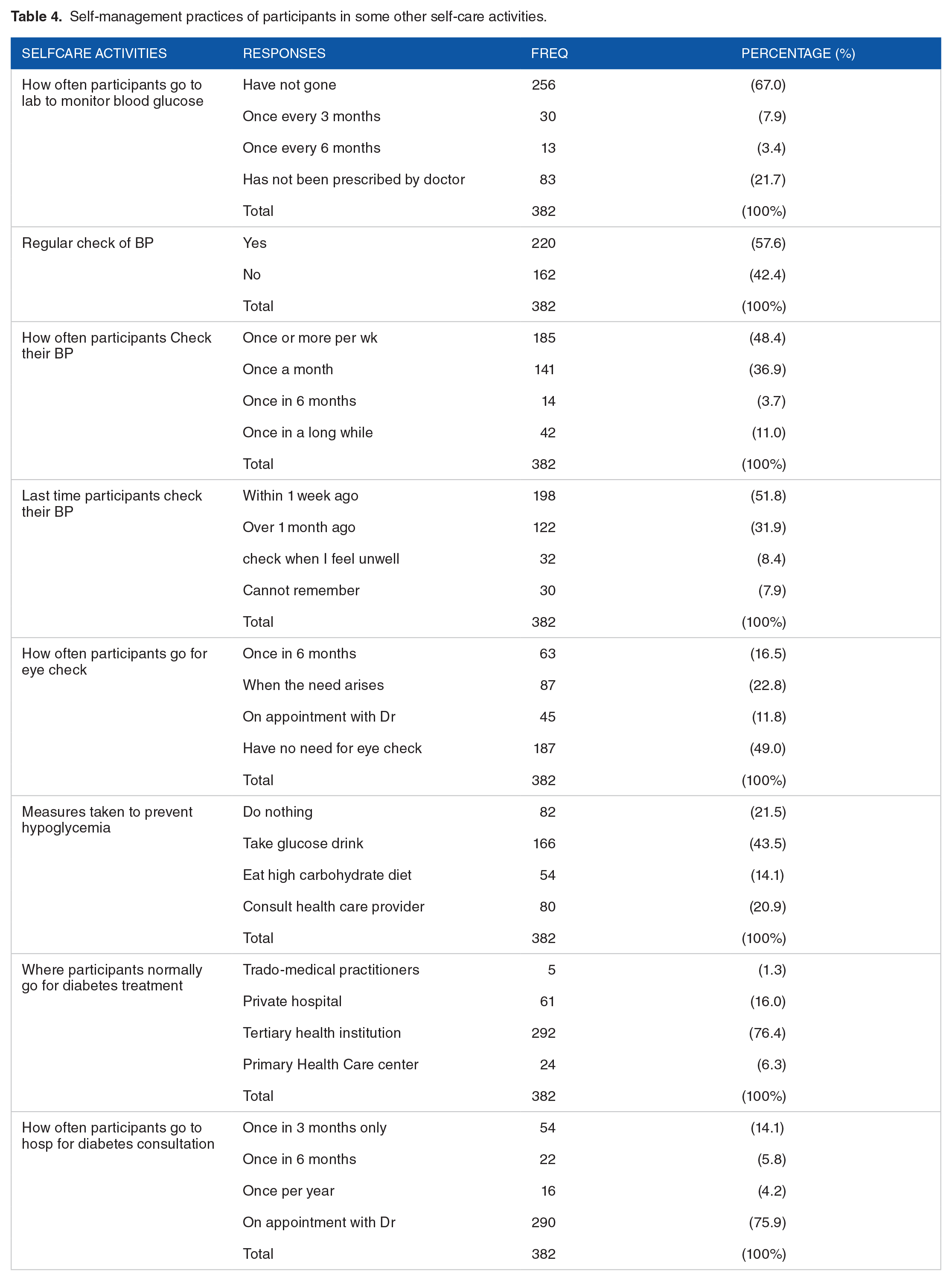
Table 5 shows the correlation between age and the self-management practices of persons with T2DM. Spearman rank order correlation test shows a significant inverse correlation between the age of participants and exercise domains
Spearman rank order test showing correlation between age and the different dimensions of self-management practice of individuals with type 2 DM.

Abbreviations: Cd, correlation of difference.
Table 6 reveals a significant association between gender and blood sugar testing (
Association between gender and the self-management practices of individuals with type 2 DM.

Table 7 reveals a significant association (P < .05) between marital status and the exercise domain of the self-care activity measurement
Association between marital status and the self-management practices of individuals with type 2 DM in South East, Nigeria.

Table 8 shows a significant association (P < .05) between the level of education of participants and the blood sugar testing domain
Association between educational level of individuals with type 2 DM and the different dimensions of the self-management practice.
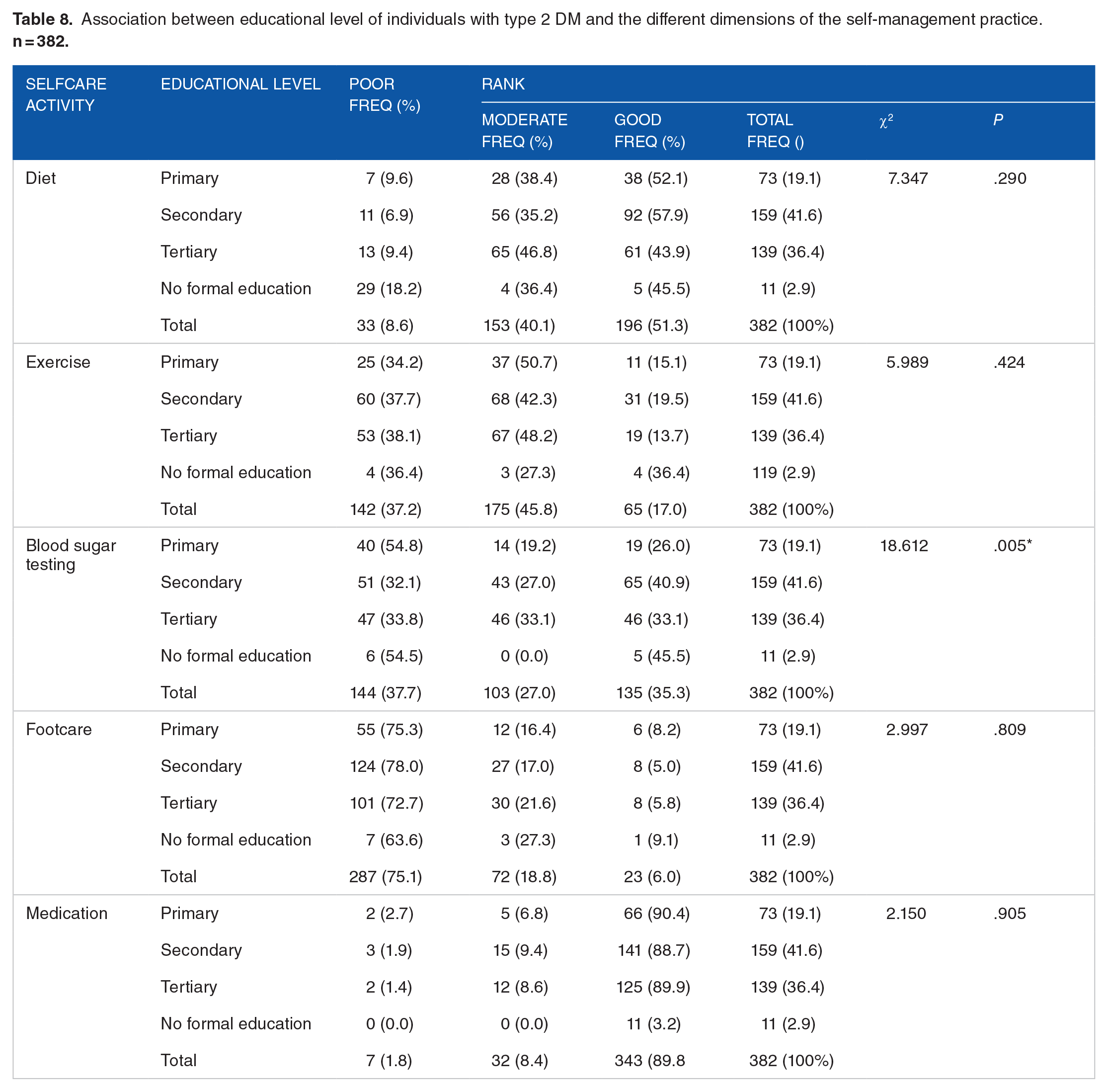
Table 9 shows a significant association (P < .05) between the occupation of participants and the following domains of the self-management practice: Exercise (P = .019), foot care (P = .006), and Medication (P = .005), a good proportion of participants 111(48.7%) who are traders participated moderately in daily exercise, 204 (89.5%) of them (traders) adhered to medication, whereas 173 (75.9%) of same traders had a poor behavior in foot care.
Association between occupation of individuals with type 2 DM and the different dimensions of the self-management practice.

Discussion
The current study was aimed at assessing self-care practices and the influence of associated socio-demographic variables of diabetic persons in South East, Nigeria. Findings on self-management practices revealed that a good number of participants had good self-management behavior in adherence to diet as well as in taking medication. These findings are contrary to the findings of a previous study in which the majority of their participants (75.9%), did not adhere to recommended diet, and only 4.3% of their participants adhered to prescribed medication. 24 This implies that Nigerians in the Southeast living with diabetes have better self-management behavior regarding adherence to diet and medication than their peers in Ethiopia as reported in a previous study. 24 This may be attributed to environmental influences and the level of knowledge available to the participants in the different areas of study.
In this study, more than one-third of all study participants had poor self-management behavior in exercise, while the majority had poor self-management behavior about foot care. The finding on exercise behavior contradicts the findings of a study in Karnataka, India in which close to half (43.4%) of their participants practiced dail7 exercise. 25 This implies that diabetic populations in India practiced daily exercise better than the diabetic population in this present study. However, the findings on poor foot care behavior in this study agree with the findings in other studies on poor foot care behavior in persons with diabetes. While a previous study 26 observed similar findings as only 0.5% of their study participants practiced daily foot care, another study 27 reported markedly low levels of self-management behavior in foot care in their study population. These findings showed that individuals with diabetes hardly care for their feet daily.
Daily self-monitoring of blood sugar levels by participants in this study was observed to be poor. This finding is in line with the finding of a previous study that reported poor self-monitoring of blood sugar levels among their study participants. 24 On the contrary, previous studies26,28 reported higher percentages (76.6% and 70% respectively) of their participants who practiced daily self-blood sugar testing. Poor self-blood sugar testing among participants in the current study may be attributed to the fact that the majority (81.2%) of them were on oral hypoglycemic agents which most often does not require daily monitoring of blood glucose level.
A significant correlation was found between age and the self-management domains of exercise and medication adherence. The inverse correlation between age and exercise implies that as age increases, individuals with diabetes will likely reduce their exercise practice. Also, the significant correlation between age and medication adherence implies that as age increases, individuals with DM are likely to increase their medication adherence.
Gender was found to significantly influence/be associated with self-blood sugar testing. Fewer proportions of females compared to males moderately practiced daily self-blood sugar testing. This finding disagrees with the findings of Mogre et al 23 in which more male participants practiced SBMG more frequently than their female counterparts. 23
Marital status was significantly associated with the exercise domain. This finding concurs with the findings of a study 28 which reported good exercise behavior among married participants in their study, a finding that is supported by the present study. Contrary to the report of another study which found an association between being married and self-blood sugar monitoring, being married however had no significant association with self-blood sugar monitoring in this present study.
Level of education was significantly associated with the self-blood sugar testing domain of the self-care activity measurement. More than half of all participants with primary education do not practice daily blood sugar testing. This finding agrees with the findings of Tan and Magarey 28 and the more recent findings of previous studies.24,29 It has been reported that only 15% of their participants practiced self-monitoring of blood glucose while the majority with low levels of education do not practice daily monitoring of their blood sugar. Also found was that 70% of their participants with primary school education were less likely to monitor their blood sugar. 24
In this study, the participant’s level of education had no significant association with the foot care domain of self-care activity measurement. This finding contradicts that of Huaung et al,29 who reported a positive influence of higher educational levels on foot care among their participants. The occupational status of participants was significantly associated with their self-management behavior in the domains of exercise, medication, and foot care. A good proportion who are traders participated in moderate exercise daily and took their medications daily, and the majority of the same traders did not practice daily foot care.
Findings on other aspects of self-care practice showed that a greater proportion of participants do not monitor their blood glucose level in the laboratory, every 3 months. This finding may be attributed to the fact that many diabetic patients in this study were not aware of such tests while some confuse it with the ordinary blood sugar test that is done anytime they go to the hospital for a checkup. Glycosylated hemoglobin (HbAic) is an expensive laboratory test that is done on diabetic persons once in 3 months to check whether their diabetes has been controlled and most often, it has to be ordered by the physician. However, this finding on laboratory blood glucose monitoring is contrary to the findings of Dinesh et al 26 in which a greater proportion (65%) of their participants monitor their blood glucose in the laboratory every 3 months. 26 This may imply that their diabetic population had better awareness of the 3-monthly laboratory monitoring of blood glucose than the diabetic population used in the present study.
More than half of all participants regularly check their blood pressure. This finding was expected because more than half of the participants had high blood pressure and they are often told during health teachings in the clinics to check their blood pressure regularly. This finding implies increased awareness of regular blood pressure monitoring among participants in this study. Findings revealed a lower proportion (16.7%) of all participants went for eye check-ups every 6 months. This finding is contrary to that of Iswarya et al 8 in which close to half (46.6%) of their participants go for eye checks every year. Almost half of all study participants indicated that they do not need eye checkups. This further shows poor self-management practice concerning observing recommended 6-monthly to yearly eye checkups for persons with DM.
A good proportion of the study participants use tertiary health institutions for diabetes treatment and also keep appointments with their doctors. These findings indicate good self-care behavior among diabetic persons in the South East, Nigeria. Diabetes mellitus is better managed by specialists (Endocrinologists) and they are mostly found in tertiary health institutions such as Teaching Hospitals and Federal Medical Centers (FMC) in Nigeria.
Influence of socio-demographic variables on self-management practices of individuals with type 2 diabetes
The self-management practice of individuals with type 2 diabetes was poor in exercise, foot care, laboratory blood glucose monitoring, and eye checkups. The current study shows a significant correlation between age and the self-management domains of exercise and medication adherence. The inverse correlation between age and exercise connotes that as age increases, individuals with diabetes will likely reduce their exercise practice as there may not be enough motivation for them to continue engaging in exercise activities. Also, the significant correlation between age and medication adherence implies that as age increases, individuals with DM are likely to increase their medication adherence. We could explain these findings by speculating that individuals living with type 2 diabetes are more likely to comply with their medication adherence than they are ready to get involved in exercise because of the fatigue usually associated with the latter. Gender was found to significantly influence/be associated with self-blood sugar testing. The finding that more males adhere to sugar testing than females could be explained by the fact that in the environment of study, women are more involved in domestic chores than men hence it is likely that women would not have time to keep faith with self-blood sugar testing. We also found that marital status was significantly associated with the exercise domain of the self-care activity measurement. Participants’ level of education had a significant association with the blood sugar testing domain of self-care activity measurement. This implies that the level of participants’ performance in self-care management in the domain of foot care is determined by their level of education. The higher the educational level the more knowledgeable they become of the need to carry out sugar testing. However, the occupational status of participants was significantly associated with their self-management behavior in the domains of exercise, medication, and foot care. We noted that a good proportion of participants (48.7%) who were traders participated moderately in daily exercise, 89.5% of them (traders) adhered to medication, whereas 75.9% of same traders had poor behavior in foot care.
Conclusion
Individuals with diabetes mellitus have poor self-management behavior in most domains of the self-management practice. Age, gender, marital status, educational level, and occupation significantly influenced the self-management practices of individuals living with type 2 diabetes.
Recommendation
The researchers recommend that nurses and health educators should take diabetes self-management education very seriously to help diabetes sufferers improve their self-management behavior.
Limitations of the study
The authors had to discard a few copies of the questionnaire because of incomplete details. Also, because the study was a multicenter study the issue of funding was a huge challenge as the study was fully funded by the authors.
Contribution to knowledge
The current study has highlighted the relationships between the practices of management of individuals living with type-2 diabetes and the socio-demographic characteristics of the individuals with type-2 diabetes in Southeastern Nigeria. It was shown that age, gender, marital status, educational level, and occupation influenced the self-care management of individuals living with type-2 diabetes. The differences in the outcome between the current study and the previous studies might stem from the different environments of the study coupled with the variations in the characteristics of the participants. Most of the participants in the current study were traders, this would have influenced the outcome of the study.
Footnotes
Acknowledgements
Not applicable
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Contributions
CNO, UPO, KUA involved in conceptualization— supporting, formal analysis—supporting, investigation— equal, project administration—equal, writing original draft—equal. EOO, MN, JTB, MTIB involved in data curation—equal, formal analysis—lead, supervision— supporting, visualization—lead, writing, review, and editing—lead. VM, MCN, AT involved in conceptualization—lead, formal analysis—lead, investigation—lead, project administration— lead, supervision—lead, writing, review, and editing—lead.
Ethics Approval and Consent to Participate
We want to confirm that all methods used in this study were carried out by the relevant guidelines and regulations as contained in the Helsinki Declaration as amended in 64th WMA General Assembly, Fortaleza, Brazil, October 2013. Ethics approval was sought and obtained from the Institutional Ethics Committee of Health Sciences and Technology, Nnamdi Azikiwe University, Nnewi Campus before the commencement of the study. Written informed consent was obtained from all the participants before they were enrolled in the study. All the authors read and approved the manuscript for publication.
Consent for Publication
Not applicable.
Availability of Data and Materials
The data is with the corresponding author and will be made available at a reasonable request.