
Abstract
Background:
Cancer survival is associated with body mass index (BMI). However, the impact of patients’ baseline characteristics on allogeneic hematopoietic stem cell transplantation (allo-HSCT) outcomes remains unclear. This study aimed to examine the baseline clinical factors associated with 5-year survival rates in patients undergoing allo-HSCT.
Material and Methods:
This was a retrospective exploratory observational study. Patients (n = 113, 52 women; average age: 55 years) who underwent allo-HSCT at the Division of Hematology and Stem Cell Transplantation, Shizuoka Cancer Center, between January 2008 and March 2015, were included in the present study.
Results:
Patients with low BMI (<18.5 kg/m2) had significantly lower 5-year survival rates than those with normal (18.5-24.9 kg/m2) and high (⩾25.0 kg/m2) BMI. The 5-year survival rate was poorer for patients with sarcopenia (41.5%) than that for those without sarcopenia prior to allo-HSCT (P = .05). The 5-year survival rate was poorer for patients with geriatric nutritional risk index (GNRI < 98) (34.5%) than that for those without GNRI prior to allo-HSCT (P < .01).
Conclusions:
Low BMI before allo-HCST pre-treatment was a predictor of 5-year survival rates in this study. Patients undergoing allo-HSCT may require nutritional interventions during pre-treatment to reduce the risk of sarcopenia and GNRI (<98), which affects their survival rates.
Keywords
Background
Standardized body mass index (BMI) values have been associated with cancer survival 1 ; however, the mechanism through which BMI affects cancer risk remains unclear. In Japan, the 5-year survival rates (2009-2011) associated with leukemia, multiple myelomas, and malignant lymphomas are reported as 44.0%, 42.8%, and 67.5%, respectively. 2 Sarcopenia in allogeneic hematopoietic stem cell transplantation (allo-HSCT) has been reported to be associated with long-term survival, 3 but no association with the geriatric nutritional risk index (GNRI) has been shown. 4 Allo-HSCT is used to achieve remission in cases of hematopoietic tumors. This study aimed to examine the impact of patients’ baseline clinical characteristics on allo-HSCT outcomes and determine the role of nutritional interventions in this context.
Materials and Methods
This retrospective, exploratory, observational study, using electronic medical records, included 120 patients (age: 16-70 years) who underwent allo-HSCT (transplantation day: day 0) and for whom nutritional intervention was recommended at the Shizuoka Cancer Center (SCC) Division of Hematology and Stem Cell Transplantation between January 2008 and March 2015. Patients were excluded from this study if data on their clinical characteristics were lacking. Allo-HSCT pre-treatments included myeloablative conditioning (MAC), reduced-intensity conditioning (RIC), and human leukocyte antigen (HLA)-matching. Transplantation types included unrelated donor bone marrow transplantation (UR-BMT), cord blood transplantation (CBT), and allogeneic peripheral blood stem cell transplantation (allo-PBSCT). 5
Patients were evaluated before undergoing pre-treatment (T1) and 5 years after receiving their transplant (T2). Remission status at T1 was not evaluated for patients with myelodysplastic syndromes as it could not be determined. Data were collected on the following variables: 5-year survival rates (using day 0 as the starting point); pre-treatment type (MAC, RIC); and associated survival outcomes, that is, baseline age, BMI, and hematopoietic cell transplantation-specific comorbidity index (HCT-CI). 6 BMI values were divided into the following 3 categories: underweight (<18.5 kg/m2), normal weight (18.5-24.9 kg/m2), and overweight (⩾25.0 kg/m2), 7 and 5-year survival rates were compared among these categories. Skeletal muscle mass index (SMI, assessed using a bioelectrical impedance analyzer8,9 [BIA: In Body S20® Seoul, South Korea] was used to diagnose sarcopenia at T1 (women: <5.7 kg/m2, men: <7.0 kg/m2), 10 and survival rates were compared between patients with and without sarcopenia. The association (5-year survival rates) between GNRI 4 was calculated as follows: (14.89 × serum albumin level) + (41.7 × [body weight/ideal body weight]). The association between GNRI at T1 and survival was evaluated, after which the cut-off value associated with survival outcomes was estimated. Survival rates were compared between groups and were defined based on a cut-off value of <98 points at T1. The observation period for all censored patients was more than 5 years.
Measurements were taken using the InBody S20® device 2 hours after breakfast (from 10:00 a.m. to 12:00 noon). We set the reference extracellular fluid-to-total body fluid ratio as 0.35 and the extracellular water-to-total body water ratio as 0.40. We defined the upper limits of the extracellular fluid-to-total body fluid ratio and extracellular water-to-body water ratio (indicating mild edema) as 0.35 to 0.38 and 0.40 to 0.43, respectively. If edema was noted, the measurements were obtained again to control for the impact of edema. All variables were measured using a high-precision body composition analyzer (InBody S20®) to determine the frequencies, which were calculated for each part of the body using 6 different frequencies (1, 5, 50, 250, 500, and 1000 kHz). 9 Data on performance status, HCT-CI, graft-versus-host disease (GVHD), and HLA-matching were extracted from the Transplant Registry Unified Management Program. 11
Statistical Analyses
The normality of distribution was verified using the Shapiro–Wilk test. All variables are expressed as medians (minimum–maximum). Multivariate logistic regression analysis was performed to assess the relationships between the patients’ clinical characteristics at T1 and 5-year survival. The associations of age with SMI and BMI, and SMI, as well as performance status, were assessed using the Pearson’s product-moment correlation. The associations between BMI and pre-treatment methods and transplantation types were assessed using analysis of variance (ANOVA). Differences in the pre-treatment method, HLA, and transplantation types between surviving and non-surviving patients were examined using the chi-square and Steel–Dwass tests. A survival curve was created using the Kaplan–Meier method, and associations between survival rates and BMI (3 categories), SMI (sarcopenia), and GNRI values were assessed using the log-rank test. All statistical analyses were performed using JMP (version 12.0®; SAS Institute, USA) and R (version 3.6.3; R Core Team [2020], www.r-project.org) software. Two-sided P-values of <.05 were considered statistically significant.
Ethical Considerations
This clinical study was performed in accordance with the principles of the Declaration of Helsinki and was approved by the relevant institutional review board (approval number: J2021-49). Verbal consent was obtained from the patients in accordance with the board’s recommendations.
Results
A total of 113 patients were included in the analysis. Seven patients were excluded due to missing baseline data. The patients’ median age was 55 years (range, 17-70 years; P < .01 according to the Shapiro–Wilk test). The mean age values for women and men were 53 (17-69) and 57 (17-70) years, respectively (P = .40: women 51, men 62). The patients’ characteristics are presented in Table 1.
Patients’ background characteristics.

Abbreviations: AML, acute myelogenous leukemia; ML, malignant lymphoma; MDS, myelodysplastic syndromes; ALL, acute lymphoid leukemia; MM, multiple myeloma; CLL, chronic lymphatic leukemia; ATL, adult T-cell leukemia lymphoma; AA, aplastic anemia; MAC, myeloablative conditioning; BU, busulfan; TBI, total-body irradiation; MEL, melphalan; RIC, reduced-intensity conditioning; UR-BMT, unrelated bone marrow transplantation; CBT, cord blood stem cell transplantation; Allo-PBSCT, allogeneic peripheral blood stem cell transplant; HLA, human leukocyte antigen; GVHD, graft-versus-host disease; HCT-CI, hematopoietic cell transplant-comorbidity; PS, performance status.
The overall 5-year mortality rate was 35% (n = 40, including 17 women and 23 men). The non-surviving group included 16 patients with acute myelogenous leukemia (AML; 8 women, 8 men), 7 patients with malignant lymphoma (ML; 3 women, 4 men), 7 patients with myelodysplastic syndromes (MDS; 2 women, 5 men), 6 patients with acute lymphoid leukemia (ALL; 3 women, 3 men), 4 patients with multiple myeloma (MM; one woman, three men), and one patient with chronic myelogenous leukemia (CML; a man). The mean age of the non-surviving group was 59 (range, 18-70) years. At T1, the mean ages of women and men were 54 (30-64) years and 61 (18-70) years, respectively. Furthermore, the mean overall survival period was 322 days (range, 46-1756 days; women: 439 days [102–1496 days], men: 273 days [46–1756 days]). The overall 5-year survival rate was 65% (Table 1).
A total of 54 and 19 surviving patients underwent MAC and RIC, respectively, at a rate comparable to that observed among non-surviving cases (31 and 9, respectively; P = .68). Surviving and non-surviving groups had comparable rates of complete and partial HLA matches (37 and 19, and 36 and 21, in the surviving and non-surviving groups, respectively; P = .85). Overall, 66, 33, and 14 patients received UR-BMT, CBT, and allo-PBSCT; the rates of these procedures differed significantly between the surviving and non-surviving groups (UR-BMT: 66 vs CBT: 33, P = .28; CBT: 26 vs allo-PBSCT: 15, P = .19; UR-BMT: 66 vs allo-PBSCT: 14, P = .53).
There was no association between age and BMI (r = .04, P = .69) or between age and SMI (r = .03, P = .76) at T1. There was no association between SMI and performance status (r = .23, P < .05) at T1. At T1, BMI values were 21.1 kg/m2 in MAC cases (14.1-31.0 kg/m2; P = .55 according to the Shapiro–Wilk test) and 21.9 kg/m2 in 28 RIC cases (17.8-29.5 kg/m2, P = .07), without any significant between-group differences (ANOVA: P = .06). Furthermore, at T1, BMI values were 21.5 kg/m2 (14.1-29.3, P = .99), 22.1 kg/m2 (15.0-31.0, P = .58), and 20.6 kg/m2 (16.5-27.5, P = .91) among patients who underwent UR-BMT (n = 66), CBT (n = 26), and allo-PBSCT (n = 21), respectively (P = .18).
The clinical characteristics associated with the onset of GVHD (grade ⩾1) and performance status are presented in Table 2. Age and BMI were associated with the 5-year survival rates (Figure 1).
Clinical indicators assessed during the nutritional evaluation.

Abbreviations: IBW, ideal body weight; BMI, body mass index; GNRI, geriatric nutritional risk index; UR-BMT, unrelated bone marrow transplantation; CBT, cord blood stem cell transplantation; Allo-PBSCT, allogeneic peripheral blood stem cell transplant; BIA, bioelectrical impedance analysis; SMI, skeletal muscle mass index; SMM, skeletal muscle mass; FM, fat mass; ECF, extracellular fluid; TBF, total body fluid; ECW, extracellular water; TBW, total body water; Pa, phase angle.
*p: Shapiro-Wilk.

Odds ratios and confidence intervals associated with baseline clinical characteristics in surviving and non-surviving patients.
Furthermore, 14, 80, and 19 patients were underweight (<18.5 kg/m2), of normal weight (18.5-24.9 kg/m2), and overweight (⩾25.0 kg/m2), respectively. Significant differences were observed in the 5-year survival rates between the underweight, normal weight, and overweight groups (Figure 2).

Receiver operating characteristics curve for survival by baseline body mass index.
The BMI cut-off value associated with the 5-year survival rate was 20.5 kg/m2 (Figure 3).

Five-year survival rates stratified by the body mass index category (underweight, normal weight, and overweight).
The T1 SMI was indicative of sarcopenia in 47 of 113 (41.5%) patients. The survival rates differed between patients with and without sarcopenia (Figure 4).

Five-year survival rates stratified by the sarcopenia status (sarcopenia is defined based on skeletal muscle mass index cut-offs of <5.7 and <7.0 kg/m2 for women and men, respectively).
The T1 GNRI indicated nutritional risk in 39 of 113 (34.5%) patients. There was a significant difference in the 5-year survival rates between patients with and without an increased nutritional risk (Figure 5).
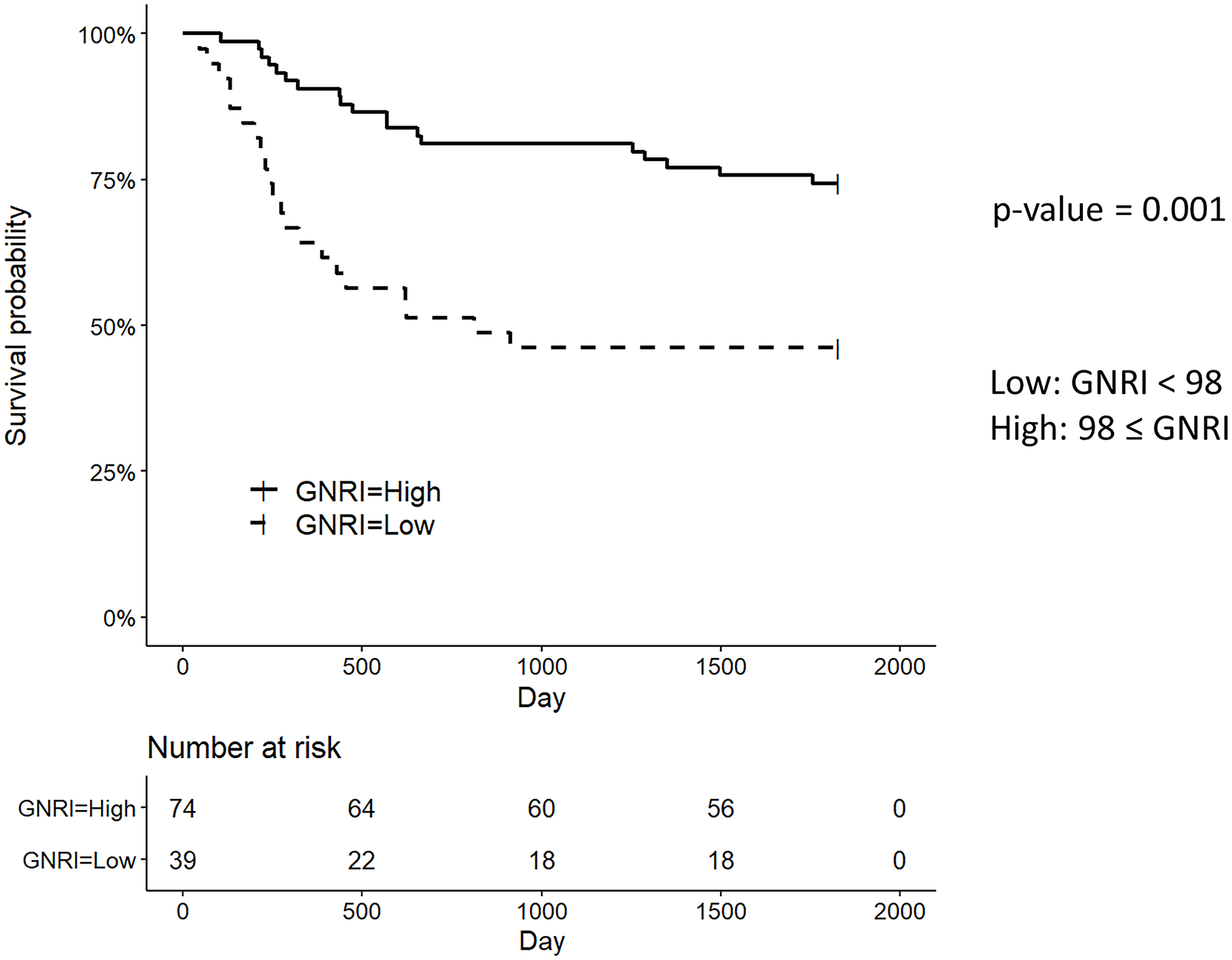
Five-year survival rates stratified by the geriatric nutritional risk index categories (low nutrition: <98 points).
Discussion
This study examined the association between the baseline clinical characteristics and 5-year survival rates of patients undergoing allo-HSCT. The overall 5-year survival rate was 65% (mean survival period: 322 [46-1756] days). Survival rates in patients with AML, ALL, CML, and ATL were 36%, 18%, 3%, and 3%, respectively, and 25%, 67%, 61%, and 100% in those with MM, ML, MDS, and AA, respectively. Survival rates for AML, ALL, CML, and ATL are very low, which may be due to the effects of non-remission, 12 Ph-positive chromosomes, 13 low performance status score, 14 the European Group for Blood and Marrow Transplantation (EBMT) risk score, 15 and acute lymphoma types 16 ; however, in the present study, these factors remain unclear. The overall cancer-related and ML-related, leukemia-related, and MM-related survival rates were comparable to, higher than, and lower than the corresponding rates previously reported in Japan. 2 Pre-treatment types and HLA-matching did not affect these survival rates. In addition, survival rates were highest in patients undergoing UR-BMT, followed by those in patients undergoing allo-PBSCT and CBT. This finding is consistent with that of a previous study 17 and suggests that declining birth rates in Japan may affect donor matching at the SCC. 18
In the present study, BMI affected survival rates at a cut-off value of 20.5 kg/m2, of which 20.5 kg/m2 may be a useful reference for nutritional interventions during remission induction or consolidation therapy before allo-HSCT.
A significant difference in 5-year survival rates was observed among patients with BMI values at baseline. Those with the highest BMI had the best prognosis, but the BMI did not exceed 35 kg/m2 in the present study. However, high BMI (35 kg/m2) may be associated with the risk of overnutrition, and nutritional interventions should be considered accordingly. 19 These results are consistent with those of a meta-analysis of studies on the impact of BMI on allo-HSCT outcomes. 20
In the present study, GNRI was associated with survival outcomes. The GNRI is an indicator of long-term nutritional status, which may account for the observed association; however, this indicator does not account for differential blood counts, such as lymphocyte levels, which are often affected by hematopoietic tumors. Nevertheless, this finding is consistent with that of a previous study on the impact of BMI on survival. 21 Meanwhile, HCT-CI values and GVHD rates were not associated with survival rates in the present study, suggesting that other pre-treatment and transplant-related factors may be relevant.
Although T1 performance status was low in most cases, sarcopenia was confirmed in 41.5% of the patients at T1. There was no association between SMI and performance status (r = .23, P < .05) at T1. Remission induction therapy and consolidation therapy are used as pre-treatments to reduce tumor size to increase the likelihood of successful allo-HSCT. 5 In this context, the present results may reflect the limited activities of daily living that patients undergoing pre-treatment may engage in, which may increase the risk of sarcopenia that warrants a nutritional intervention.
Furthermore, in the present study, baseline BMI and GNRI values (both of which depend on body weight) affected survival outcomes of patients undergoing allo-HSCT. The impact of sarcopenia on transplantation outcomes suggests a need for nutritional assessments and interventions before allo-HSCT.
This study had some limitations, including the lack of stratification by diagnosis and treatment type and a lack of baseline BIA data (which may have biased the present findings). In addition, the follow-up period was relatively short in this study. Future studies should involve longer follow-up periods and larger sample sizes to obtain data on baseline BMI before the start of transplant-associated treatments, which may affect body weight.
Conclusions
The baseline BMI affected survival outcomes after allo-HSCT, independently of the other clinical characteristics. The presence of sarcopenia and GNRI values also affected survival outcomes after allo-HSCT. The presence of sarcopenia and nutritional riskin patients referred for allo-HSCT suggests a need for nutritional intervention as part of the pre-treatment protocols.
Research Data
sj-xlsx-1-nmi-10.1177_11786388221128362 – Research Data for Impact of Body Mass Index on 5-Year Survival Rates in Patients Undergoing Allogeneic Hematopoietic Stem Cell Transplantation
Research Data, sj-xlsx-1-nmi-10.1177_11786388221128362 for Impact of Body Mass Index on 5-Year Survival Rates in Patients Undergoing Allogeneic Hematopoietic Stem Cell Transplantation by Takashi Aoyama, Akifumi Notsu, Koki Ichimaru, Kinuko Hayashi, Masanori Tsuji, Kanako Yoshitsugu, Masafumi Fukaya, Terukazu Enami and Takashi Ikeda in Nutrition and Metabolic Insights
Footnotes
Acknowledgements
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by JSPS KAKENHI [Grant number: 22K18237].
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
TA performed the experiments, data analysis, and interpretation and drafted the manuscript. All authors read and approved the final manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.