
Abstract
Introduction:
Currently, nutritional rickets has become a concern of many nutrition experts in many countries. Sunlight is the best and most reliable Source of vitamin D. Since, there is scarce information regarding infant sunlight exposure practice and the determinant factors. Hence, this study aimed to assess mothers’ infant sunlight exposure, practice level, and associated factors.
Methods:
A community-based cross-sectional study was conducted on 884 mothers from March 20 to April 4, 2017. Through the multi-stage simple random sampling method, the study areas had selected. The data were collected using a structured and pre-tested questionnaire and were entered into Epidata version 3.1 and exported to SPSS version 20 for analysis. The strength of association was measured using binary logistic regression at a 95% CI odds ratio. Finally, P < .05% was declared statistically significant.
Results:
From 884 infant coupled mothers, 866 were recruited in the study with a response rate of 97.9%. Only 44% of mothers had good practice of infant sunlight exposure. In multivariate analyses; Knowledge status (AOR = 1.4, 95% CI: 1.0-1.9), Attitude status (AOR = 1.4, 95% CI: 1.1-1.9), mothers age group (AOR = 8.6, 95% CI: 5.1-14.4), mothers educational status (AOR = 5.2, 95% CI: 1.6-16.9), delivery at health facility (AOR = 1.5, 95% CI: 1.0-2.1), and friend influence (AOR = 1.6, 95% CI: 1.2-2.1) were significantly associated with maternal exposure status of their infants to sunlight.
Conclusion:
This finding showed that the majority of the mothers did not expose their infants to sunlight appropriately. The mother’s knowledge, attitude, educational status, institutional delivery, and friend influence were the significant factors and needs to work on these.
Introduction
For centuries back to ancient Rome and Greece civilization, Sunlight exposure had used for therapeutic purposes (heliotherapy).1,2 During the second half of the 19th Century, the sunlight had realized as a bactericidal and therapy purpose for rickets.1 -4 The level 25(OH)D also determines the body’s calcium homeostasis, bone health, cellular health, and immunity function. At least a level of 20 and 30 ng/ml of 25(OH)D are required to maintain calcium homeostasis and maximal bone health and cellular health orderly.5 -8 It is crucial for the Immune system, maintaining cardiovascular function, healthy heart and circulation, respiratory system, healthy lungs and airways for Brain development, Muscle function, and anti-cancer effects. 9
Exposure of the body in a bathing suit to one minimal erythemal dose (MED) is equivalent to taking 10 000 to 25 000 IU vitamin D orally. Therefore exposure of the body parts like arms, face, legs, and hands to sunlight for one MED 2 to 3 times a week is sufficient to get adequate body vitamin D requirement and even for the storage of vitamin D3 in the body fat. 8
Sunlight exposure is the cheapest source of vitamin D. When the skin expos to the sun, vitamin D will produce. Sunscreen blocks ultraviolet light from damaging the skin, But, it does affect vitamin D production from the skin. Although most people believe using sunscreen lowers vitamin D production from our skin, no proven evidence supports their belief.10,11
Some literature said that reduced exposure to the sun and choose sunglasses with medium to dark lenses for UV-A and UV-B protection during peak hours between 11 am and 4 pm when a person’s shadow appears shorter than they are.10,12
Vitamin D can produce by our skin upon exposure to ultraviolet B (UVB) irradiation (280-320 nm) from sunlight. 13 More than 90% of the circulating vitamin D in the body originates from cutaneous production. 13 Sunlight converts 7-dehydrocholesterol in the skin to vitamin D3, which will be transported to the liver and hydroxylated to 25-hydroxyvitamin D (25(OH)D). It will then be conveyed to the kidney and hydroxylated to 1,25-dihydroxyvitamin D (1,25(OH)D). 13 1,25(OH)D is the metabolically active prohormone. The level has uses as a determinant factor of vitamin D status. Vitamin D deficiency will result in osteomalacia and rickets.
Recent studies have shown that vitamin D insufficiency is common in tropical countries even if there is sunshine throughout the year in this region due to malpractice and inadequate knowledge toward the exposure of infants to sunlight. 14
Ethiopia adopts health education as a strategy to change maternal behavior on infants’ sunlight exposure to prevent rickets in the country during the 1960s. 15 Implementation of this strategy remains low, inconsistent, and health messages had no focus that positively influences maternal practice, infants not to get adequate sunlight. Lack of sufficient information on the determinant of this risky behavior and the attitude of Ethiopian mothers. 15
Vitamin D deficiency is prevalent among urban and rural Ethiopian school children for 61.8% and 21.2%, respectively. 16 The study had conducted on pregnant women and women of reproductive age showed that vitamin D deficiency is prevalent in Ethiopia.15 -17 Some initial and recent studies suggested that daily practice to sunshine remains the cheapest, safest, and most effective method of preventing rickets.15,17
There is scarce information regarding the mother’s practice of infant sunlight exposure and its determinant factors. Hence, this study aimed to assess mothers’ infant sunlight exposure, practice level, and associated factors.
Methods and Materials
Study design, setting, and period
A community-based cross-sectional study was done at Dejen woreda from March 20 to April 4, 2017. The woreda had latitude and longitude of 10°10′N38°8′E and an elevation between 2421 and 2490 m above sea level. It is one of the woredas in the Amhara Region of Ethiopia.
Based on the 2007 national census conducted by the Central Statistical Agency of Ethiopia (CSA), the woreda has 23 kebeles and 102 359 total population. Seven Kebeles had selected for the study.
Study participants and sampling procedures
All mothers who had an infant during the data collection period in the selected kebeles were the study populations. While mothers who fulfilled the inclusion criteria were the study participants. Multi-stage sampling technique and computer generated random sampling methods were used to recruit 884 infant coupled mothers from 7 kebeles (Figure 1) A single population proportion formula was used to determine sample size using the Epi Info Version 3.5.1 StatCalc software considering a proportion of 50%, confidence interval (CI) of 95%, and margin of error 5. In addition, the Epi Info StatCalc was also used to calculate sample size using the risk factors for sunlight exposure status: using proportion of good and poor practice of infants’ exposure status to sunlight, exposed to unexposed group ratio of 1:1, a power of 80%, odds ratios, and 95% CI as shown in Table 1. After that, a sample size of 384 was calculated, however, with a 15% non-response rate and a design effect of 2, the final sample size was estimated to be 884.


Schematic presentation of sampling procedure of knowledge, attitude, practice, and associated factors of mothers toward infant sunlight exposure in Dejen 2017.
Sample size determination of the study participants using EPI Info version 3.5.1.

Where n = sample size
P = proportion take as 50% (no previous study)
d = margin of error
α = 5%
Zα/2 with 95% confidence level = 1.96.
And hence 1.962 0.5(1 − 0.5)/0.052 = 384 samples were required.
And hence considering none response rate of 15%, and the sample size of this study was calculated as; 384 × 15% = 58 then 58 + 384 = 442 sample.
Multiplying 442 by the design effect 2 gives 884. For the associated factors, a double population proportion formula using EPI Info version 3.5.1 StatCalc had used to calculate the sample size.
But the value was lower than the above sample size. Then the final sample size was 884 infants.
Data collection methods and instruments
The data had collected through 5 diploma Nurses and 1 BSc nurse supervisor. The Data were collected through the home-to-home visits using a structured adapted interviewer-administered questionnaire. The questionnaires had 5 parts, socio-demographic characteristics, Knowledge, Attitude, Practice related, and associated factors of mothers toward their infant sunlight exposure. The questionnaires were prepared initially in the English version and translated to Amharic version and Amharic version questionnaire was used for data collection.
Variables of the study
The dependent variable was maternal practice level regarding infant sunlight exposure. Socio-demographic variables (Age of infant, Age of mothers, Mother Educational status, Husband educational status, Mothers Religion, Family size, Mothers Occupation, Father’s occupation), social factor (media influence, health professional influence, infant grandmother influence), and health-seeking behavior of mothers (ANC follow up, place of delivery), Knowledge status, and Attitude status were the independent variables.
Operational definition
Infant: a child whose age is less than 12 months old.
Good practice: those mothers who responded to the practice-related questions and scored above the median. 18
Poor practice: those mothers who failed to respond to the practice-related questions and scored less than or equal to the median values. 18
Good-knowledge: those mothers who responded to the knowledge-related questions and scored above the median. 19
Poor knowledge: those mothers who respond knowledge related questions and scored less than or equal to the median values. 19
Favorable attitude: those mothers who responded to attitude-related questions and scored above the median value.20 -22
Unfavorable attitude: those mothers who responded to attitude-related questions and less than or equal to the median values.20 -22
Data quality control
Two days of training had given for both the data collectors and supervisor. The adapted questionnaires were prepared initially in the English version and translated to the Amharic version and then back to the English version for consistency. The pre-test had done on 5% of the sample in the other woreda. The completeness of data, missing, and inappropriate data filling was checked daily by supervisor and principal investigator.
Data processing and analysis
The data was checked visually, coded and entered into EPI data version 3.1 and exported to IBM-SPSS version 20 for statistical analysis. The association between each independent variable with the outcome variable had assessed using bivariate logistic regression. Model fitness was checked using Hosmer and Lemeshow goodness of fit. P < .2 in bivariate analysis covariate retained for multivariate analysis. Logistic regression analysis had performed to identify factors associated with the outcome variable. Finally, a P < .05 declare as statistical significance. The data had presented using tables, charts, and texts.
Result
Socio-demographic characteristics
Of 884 sampled mothers, 866 of them were recruited in the study with a response rate of 97.96%. Among 866 study participants, 534 (61.7%) mothers had less than or equal 6 months of age infant. More than half, 460 (53.1%) mothers had age less than or equal to 30 years old (Figure 2). The mean age of study mothers and infants were 31.1 (95% CI, 30.5-32.0 with standard deviation of ±6.371) years and 5.71 (95% CI, 6.2-6.6 with standard deviation of ±3.1) months respectively. The majority of mothers 847 (97.8%), were orthodox by religion, 863 (99.7%) were Amhara by ethnicity. Almost 827 (95.5%) were married (Table 2).
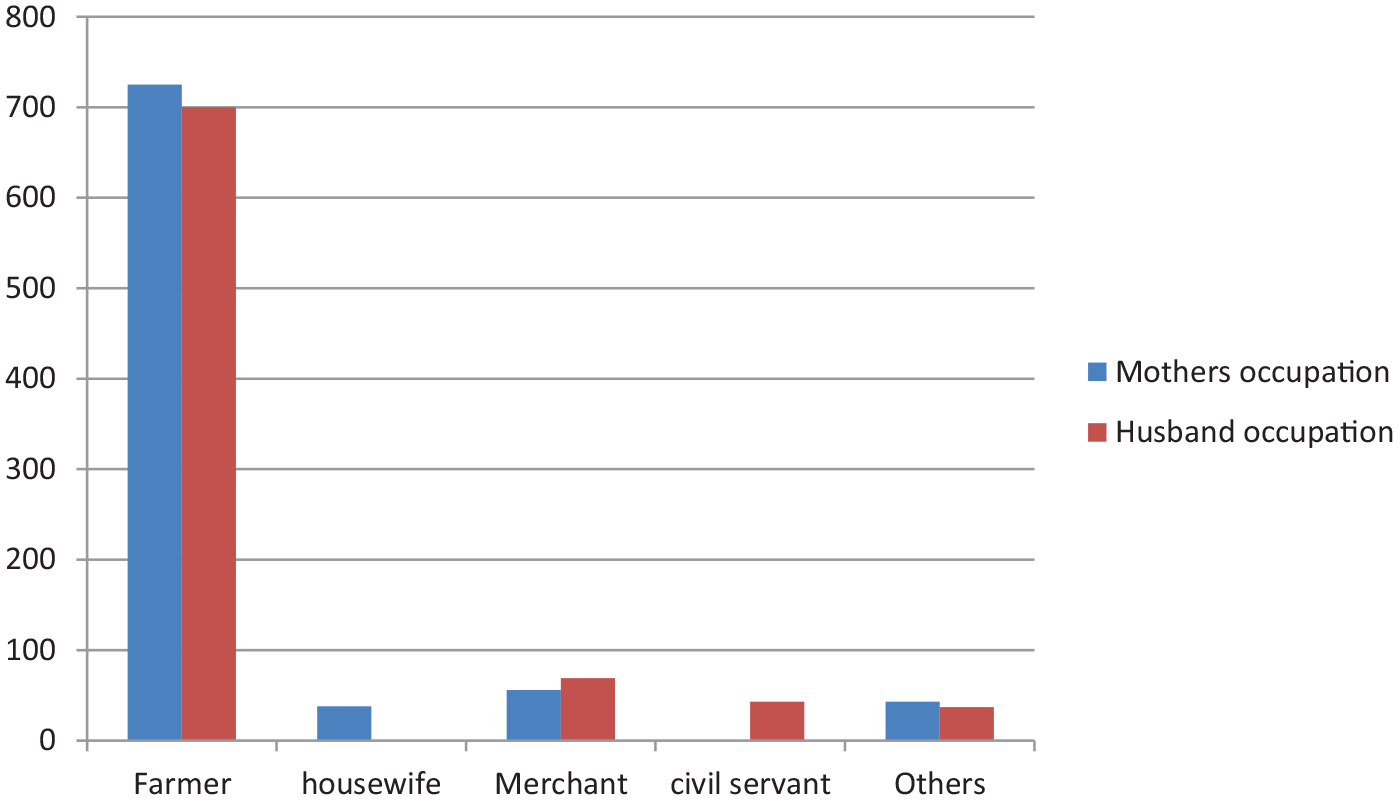
Occupational status of the husband and mothers of the study participants Dejen woreda, Ethiopia 2017.
Distribution of socio-demographic characteristics of study participants in Dejen woreda, East Gojam Zone, Amhara Region, Ethiopia, 2017 (n = 866).

Majority of study mothers, 769 (88.8%) were farmers by occupation as shown in Figure 2.
Knowledge of mothers toward infant sunlight exposure
The median value of knowledge of study participants was 7.5. Out of 866 study participants, 433 (50%) had poor-knowledge status regarding infant sunlight exposure. The majority of mothers (852, 98.4%), knows infant sunlight exposure were essential to the infant, and 373 (43.1%) had answered infant sunlight exposure are for the development, growth, and strength of bone, and 779 (90%) of mothers know relatively the safest period of infant sunlight exposure. Regarding knowledge of the harmful effect of sunlight exposure (246, 28.4%), (38, 4.4%), (454, 52.4%), and (107, 12.4%) of mothers mentioned that it causes skin cancer, gigantism, dark skin pigmentation, and fever were respectively.
Attitude level of study mothers toward infant sunlight exposure
Almost 473 (54.6%) of mothers had an unfavorable attitude. From these, 239 (27.6%) and 211 (24.4%) mothers strongly disagreed that sunlight exposure did not have an evil eye effect.
Practice level of study mothers on infant sunlight exposure in April 2017
Five hundred six (56%) of mothers scored less than the mean value practice-related questionnaire. Even though 829 (95.7%) of mothers intentionally expose their infants to sunlight. The majority of mothers 439 (50.7%) and 571 (65.9%), expose infants after applying butter on the infant’s body and cover with a cloth (Table 3).
Practice level of study mothers regarding their infant sunlight exposure in April 2017.

Determinant factors of mothers’ infant sunlight exposure practice
A significant association was observed between mothers’ knowledge status; attitude status, age groups; educational level with the mother’s practice level regarding infant sunlight, exposure. Mothers who had good knowledge regarding infant sunlight exposure were 1.4 times more likely to have a good practice of infant sunlight exposure than those mothers who had poor knowledge (Table 4).
Multivariate analysis of characteristics’ associated with the practice status of study mothers regarding their infant sunlight exposure.

Abbreviations: AOR, adjusted odds ratio; COR, crude odds ratio; URAW, unable to read and write.
Discussion
More than 829 (95.7%) of mothers intentionally expose their infants to sunlight. It is almost similar to the study done at Debre Markos, 96.6%. 18 But higher than the study done at Yirgalem General Hospital which was 84.7%. 23 The variations could be attributed to differences in educational status and cultural practices in different geographical locations within the same country. More than 77% of mothers expose their infants to sunlight outdoor. These were lower than the study done at Debre Markos and Sakarya which were 89.4% 13 and 87.5% 18 respectively. Ninety (90.5%) of mothers expose their infant in the relatively safest (morning before 10 am and after 5 pm) period that was lower than the study report from Debre Markos. 18 The variation may be due to differences in awareness level of mothers concerning the importance of infants’ sunlight exposure. Half of the mothers in the present study exposed their infant after applying butter to the infant’s body before exposing infants to sunlight. However, the finding was higher than the study report from Debre Markos, 43.7%. 18 This might be due to knowledge gap regarding the disadvantage of malpractice (application) between the studies and it might have an impact in the synthesis of Vitamin-D properly. About 53% of the study mothers expose their infant after covering with a cloth which is higher than the study done at Yirgalem General Hospital that was 27.8%. 23 Such big discrepancies might be resulted either from cultural influences or poor awareness. More than 56% of mothers had poor practice of infant sunlight exposure which is higher than the study done at Yirgalem General Hospital that was 45%, 23 study done at St. Paul’s Hospital that was 40%, 24 and a study done in Farta district which was 45.7%. 25 The possible reason may be the study period, study area, and cultural difference. However, it is lower than the study done at Aleta Wondo Health Center which was 67.4%. 26 The reason behind this may be cultural and educational status difference.
In this study, more than half mothers (52%) had started exposing their infant at the age of 15 to 45 days which is lower than the study done at Yirgalem Hospital that was 66.4%. 23 The reason may be the study period difference.
A mothers’ educational status had a significant association with the practice of infant sunlight exposure. This was supported by the study report from Debre Markos. 18 knowledge status, Attitude status, mother’s educational status, mother age group, delivery at a health facility, and mothers’ friend influence had a significant association with the mothers’ practice status.
Conclusion
More than half of the mothers did not practice appropriate infant sunlight exposure. Mothers; educational statuses, knowledge status, attitude status, education status, age group, friend influence, and health facility delivery had significantly associated with the practice level of infant sunlight exposure. The present study finding indicates a need of awareness creation for the community concerning the importance of infants’ exposure to sunlight with the proper practice.
Footnotes
Acknowledgements
First, we would like to thank Debre Markos University Department of Public Health for giving us this chance to conduct research. Second, we want to extend our thanks to the East Gojam Zonal Health Department, Dejen woreda health office staff, and health extension workers of the study area for giving relevant information for this study. Finally, we would like to give our gratitude to Debre Markos University library staff post-graduation, documentation, and record staff for their cooperation.
Authors’ Contributions
AB conceptualization. AB, AM, YH, BA, and HT formal analysis. AB, AM, YH, BA, and HT development or design of methodology. AB, AM, YH, BA, and HT entering data into software. AB, AM, YH, BA, and HT supervision. AB, YH, BA, and HT writing original draft. AB, AM, YH, BA, and HT writing review and editing. AB and ABYHBAHT prepares all figures. AB, ABYH, and BAHT prepare all tables. AB, ABYH, and BAHT wrote the main manuscript text, all authors read and approved the final manuscript.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
The proposal was submitted and approved by the Debre Markos university ethical review committee as ሣኮ/ምር/ማህ/አገ/ድህ/ም/አስ/339/15/09 in 2017. A letter of permission had obtained from the Dejen woreda health office. A briefing had given for every study participant before taking oral consent. Confidentiality was maintained by excluding their name and personal identifiers.
Data Availability Statement
The data sets used and analyzed in this study are available from the corresponding author. Data will not be shared to preserve the participant anonymity.