
Abstract
Introduction:
Iron deficiency anaemia is an international public health concern and pregnant women are at an increased risk. We investigated the consumption of iron rich foods and associated factors among pregnant women in a rural district from Ghana.
Methods:
Following a cross-sectional design, dietary intake of iron rich foods was obtained from 252 pregnant women using a 24-hour recall food check list. Nutrition knowledge, attitudes and socio-demographic characteristics were also assessed.
Findings:
Participants had a mean (SD) knowledge score of 54.66 (22.74)%. About 73% of the participants had heard about iron-deficiency anaemia. Only 16.3% of the participants knew foods that help the body to absorb and use iron while 9.1% knew beverages that decrease iron absorption. About 71% of the participants ate fish and/or seafood while 67.1% of them ate green leafy vegetables. Only 4.4% of the participants ate organ meat, and 29% took flesh meat. Only 22.4% of the study participants usually drank coffee or tea while 78.2% ate vitamin C-rich foods. With regards to attitudes, 88.5% of the participants perceived anaemia to be a serious disease. Nutrition knowledge was significantly associated with the consumption of iron rich foods (β = .02; 95% CI = 0.01-0.02).
Conclusion:
Nutrition knowledge may be an important determinant of the consumption of iron rich foods among pregnant women making it necessary for healthcare providers to continue to provide nutrition education to pregnant women during routine antenatal care.
Introduction
Anaemia is an international public health problem affecting maternal and child mortality, physical performance and visits to health care facilities. 1 It is associated with high morbidity and mortality in women and children,2-4 poor birth outcomes,5,6 decreased work productivity in adults and poor brain and behavioural development in children. 7 Populations at increased risk of anaemia are children and women of reproductive age. 2 According to the World Health Organization (WHO), a third of the world’s population are anaemic in which 40% are pregnant women. 8 Global evidence show that 56% of pregnant women in developing countries are anaemic. 3 A systematic review of evidence from 4 Sub-Sharan African countries reported that the prevalence of anaemia in pregnant women ranged from 32% to 62%. 9 The 2014 Ghana Demographic Health Survey estimates that 45% of pregnant women are anaemic. 10 Half of the cases of anaemia in the world is due to iron deficiency, the most common nutritional deficiency in the world. 11 Iron deficiency negatively affects productivity and cognition and contribute to about 20% of all maternal and perinatal mortality and low birth weight.12,13
Iron deficiency anaemia could be due to a number of factors including poor dietary intake of iron rich foods, unavailability of foods rich in iron, household food and nutrition insecurity, poor nutrition knowledge and attitudes, high demand for iron during pregnancy and worm infestations and infections such as malaria.14,15 In addition, most pregnant women from developing countries enter pregnancy with an already low level of iron in the blood which is exacerbated by the increased demand for iron by the developing foetus.3,16
One of the frequently reported measures of diet quality is diet diversity and it assesses the number of foods consumed across and within food groups during the last 24 hours.17-19 It is assumed that increasing the variety of foods and food groups in the diet could help one achieve an adequate intake of essential nutrients. Evidently, diet diversity has been shown to be associated with nutrient adequacy and has become a key element of high-quality diets. 17
Nutrition education interventions are some of the strategies that could be used to improve the nutrition knowledge and attitudes of pregnant women towards iron deficiency anaemia and the consumption of iron rich foods. However, such nutrition education interventions can only be effective if there is data that reports on dietary practices and associated factors among pregnant women regarding the consumption of iron rich foods. Although a number of studies from Ghana20-24 and elsewhere in sub-Saharan Africa9,25-28 have reported on the phenomenon the majority focussed on the prevalence of anaemia as well as knowledge and attitudes of pregnant women towards anaemia in general but not iron deficiency anaemia.20-23,26 Also, only a few of the studies have investigated the dietary practices of pregnant women regarding the consumption of iron rich foods.9,21,24 Furthermore, most of the studies from Ghana except one 24 were conducted in the Southern parts of Ghana which is socio-economically different from the Upper West Region that is more rural and poorer. Thus, evidence on the dietary practices of pregnant women and its determinants is limited especially from a poor rural setting such as the Nandom District in the Upper West Region of Ghana. We investigated the consumption of iron rich foods (using diet diversity as a proxy) and associated factors among pregnant women in a rural district in Ghana.
Methods
Study design, setting and participants
Following a cross-sectional design, this study was conducted among pregnant women attending monthly outpatient antennal clinic at the St. Theresa’s Hospital located in Nandom, the capital of the Nandom Municipal. The district lies in the north western corner of the Upper West Region of Ghana between Longitude 2°25 W and 2°45 W and Latitude 10°20 N and 11°00 S. It is bounded to the East and South by the Lambussie and Lawra Districts respectively and to the North and West by the Republic of Burkina Faso. It is the most densely populated District in the region. It has an estimated 2020 population of 50, 698 projected from the 2010 population census. About 78% of the employed population engage in agricultural, forestry and fishery work. The St. Theresa’s Hospital which is the Municipal Hospital of Nandom is an agency hospital established by the Catholic Church. The hospital has a total bed capacity of 218.
Study population, participant recruitment and data collection procedures
Permission was obtained from the Municipal Health Administration of the Nandom Municipal to have access to the hospital and the Antenatal clinic (ANC). The hospital provides daily antenatal care through its ANC to pregnant women scheduled to attend. All pregnant women who attended the ANC were eligible for inclusion into the study. Pregnant women were excluded if they were unwilling to participate in the study. On days scheduled for data collection 2 members of the research team (N.Y.A.B and V.A.A) visited the ANC. After the pregnant women had received their antennal care, N.Y.A.B and V.A.A approached them to introduce the study to them and to also seek for their consent to participate in the study. Potential participants who agreed to participate were taken through the informed consent processes and a questionnaire administered to those who consented. The questionnaire was self-administered to those who could read in English but translated into a local dialect for those who could neither read nor write in English. Written informed consent was obtained and participation in the study was voluntary. Participants were at liberty to withdraw from the study at any time if they felt uncomfortable. Confidentiality of the data was assured. All data was collected in a secluded room at the hospital premises. Ethical approval was granted by the University for Development Studies Institutional Review Board through the Department of Community Health and Family Medicine (UDSIRB/2020).
Data collection methods
Data was collected using a questionnaire, items of which were adapted from the guidelines for assessing nutrition-related knowledge, attitudes and practices manual of the Food and Agriculture Organization of the United Nations. 18 The questionnaire was adapted to fit the local context of the study in which locally available sources of iron were included in the questionnaire. The knowledge scale had 9 items and consisted of multiple-choice questions. The knowledge areas that were assessed included awareness regarding iron deficiency anaemia, health risks of iron deficiency, the causes of iron deficiency anaemia, food sources of iron and how to prevent anaemia. Each question was scored a point for a correct answer. Total scores were generated for each participant and computed out of 100%. Frequency of participants who correctly answered a question was also computed.
Components of attitude towards iron-deficiency anaemia during pregnancy that were evaluated were: perception of the likelihood of getting iron-deficiency anaemia; seriousness of iron deficiency anaemia to the health of the mother and the foetus; perception of the effectiveness of iron supplements to prevent anaemia; and confidence and difficulty in preparing meals with iron-rich foods. The attitude scale had 13 items that were answered on a 3-point-Likert scale. Two forms of the 3-point Likert scale were used depending on whether the item was assessing perceived barriers or perceived benefits. For perceived barriers the responses were: 1-not difficult, 2-so-so and 3-difficult. For perceived benefits: 1-not good, 2-not sure and 3-good. In order to ensure higher scores denoted positive attitude, items for the perceived barriers were reversed score (ie, 1 = 3, 2 = 2, 3 = 1). Total scores were generated for each participant and computed out of 100%.
Dietary intake was assessed using a food-intake check list. A food-intake checklist is a simplification of the 24-hour dietary recall approach which ask whether a particular food or list of foods was consumed in the past 24 hours. 18 Given that the micronutrient of interest was iron, 7 food groups that are shown to be rich sources of iron were included. These were organ meat, flesh meat, insects, fish and seafood, legumes, green leafy vegetables and iron-fortified foods. To contextualize the questionnaire, iron rich foods that were peculiar to the study area were added to the list of foods per group whereas foreign food items were removed or replaced with equivalent local ones. Thus, from a list of locally available iron rich foods, participants were asked to indicate whether they ate any of the foods in the last 24 hours. Responses of the pregnant women to these questions were used to generate a dietary diversity score for iron (DDSI). The DDSI was obtained by summing the number of the food groups consumed in the last 24 hours, 17 with the aim to be reflective of nutrient adequacy.17,29 For instance, if a participant reported eating at least one of the foods listed in a particular group, the participant was scored 1 for that food group. Given dietary diversity scores are usually used as a proxy of nutrient adequacy,17,30 DDSI was used in this study as a proxy of adequacy of the consumption of iron rich foods. The questionnaire also assessed participants’ consumption of foods that enhances or may inhibit the absorption of iron. To evaluate the consumption of foods that enhances the absorption of iron, participants were asked to indicate Yes or No to the question ‘Do you usually eat vitamin C rich fruits, such as (orange, lemons, mango, baobab fruit, “ɔraa”, etc.) or drink juice made from them?’ To assess the consumption of foods that may affect the absorption of iron, participants were asked to indicate Yes or No to the question ‘Do you usually drink coffee or tea?’ The frequency and timing of the consumption of these foods were also asked.
General and socio-demographic characteristics of the participants were also evaluated using the questionnaire. These were age, marital status, educational status, ethnicity, employment status, husband’s employment status and whether husband earns enough.
To ensure comprehensibility, the questionnaire was pretested among 20 participants selected from a non-participating community within the area having similar demographic characteristics. This allowed for further clarification and modification of some of the items of the question. In addition, the questionnaire was evaluated for content validity by a team of nutritionists, behavioural sciences and public health specialists.
Statistical analysis
The data was entered into, and analysed using the Statistical Package for Social Sciences (SPSS) version 21.0 software. Descriptive statistics such as mean, standard deviation and frequency tables were used to describe the data. Pearson correlation was used to determine associations among continuous variables (ie, knowledge, attitude, DDSI and age). Student t-test and one-way anova were used to determine associations among continuous variables (ie, DDSI) with categorical variables such as marital status, educational status, ethnicity, employment status, husband earning enough and husband’s employment status. To assess the determinants of the consumption of iron rich foods (DDSI), multiple linear regression was adopted. A P-value less than .05 was considered significant in all analysis.
Results
General and socio-demographic characteristics of the participants
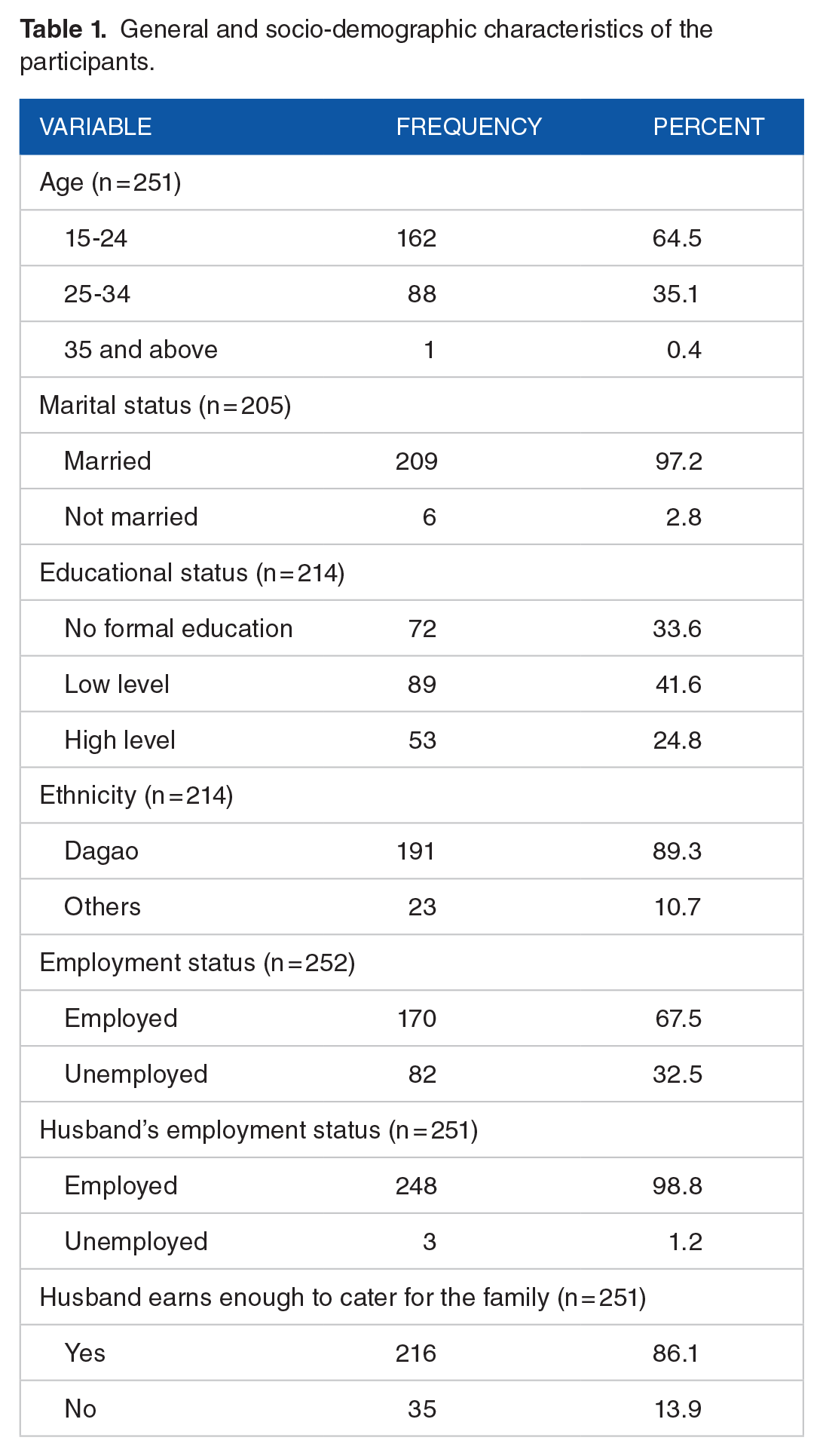
Table 1 presents the general and socio-demographic characteristics of the participants. With a mean (SD) age of 28.11 (6.37) years, 64.5% of the pregnant women were within the 15 to 24 age category. Also, 97.2% of them were married; 24.8% had higher level education (tertiary or senior high level) and 33.6% had no formal education. Other ethnic groups (Moosi, Dagomba, Akan, etc.) make up 10.7% of the participants with the rest being Dagaos. Only 20.9% were in their first pregnancy.
General and socio-demographic characteristics of the participants.
Nutrition knowledge of the participants
Table 2 presents the knowledge of participants with regards to anaemia and the consumption of iron rich foods. About 73% had heard about iron deficiency anaemia; 55% could recognize the symptoms and signs of anaemia and 72.1% knew the causes of anaemia. Only 16.3% knew the foods that help the body absorb and use iron. Mean (SD) knowledge score was 54.66 (22.74)%.
Knowledge of anaemia and iron-rich foods.

Attitudes towards iron-deficiency anaemia
Forty four percent (n = 59) of the participants perceived that there were likely to be iron-deficient. Almost 90% (n = 223) perceived anaemia to be a serious disease and 76.6% believed iron supplements alone could prevent one from getting anaemia and 14.3% (n = 36) did not think so. Most of the people who said taking iron tablets only was not effective in preventing anaemia illustrated the need to consume iron rich foods to complement the iron supplements. Eighteen percent (n = 44) thought it was difficult to prepare iron-rich meals and the rest thought it was not difficult. However, 98.4% (n = 248) were confident in preparing meals with iron-rich foods. Among those who reportedly said it was difficult to prepare iron-rich foods, identified unaffordability and inaccessible of those foods as reasons why they found it difficult to prepare iron rich foods. Participants described their likeness for the taste of beef in which 77.6% (n = 194) said they liked it; 18.8% (n = 47) disliked it and 3.6% (n = 9) were unsure. Participants had a mean (SD) attitude score of 89.44 (8.91).
Consumption of iron-rich foods
Table 3 shows a 24-hour recall of the consumption of iron-rich foods and foods that enhances or inhibits the absorption of iron. Only 4.4% of the participants ate organ meat and 29.0% took flesh meat. However, 70.6% ate fish and/or seafood, and 67.1% ate green leafy vegetables. The pregnant women had a mean dietary diversity score for iron of 2.74 (1.09) with scores ranging between 0 and 7.
Practices in relation to consumption of iron-rich foods.

Determinants of consumption of iron rich foods using DDSI
Following a correlation analysis, there was a positive correlation between DDSI with knowledge (r = .307, P < .001) and attitude scores (r = .149; P = .018) (shown in Table 4). Using one-way ANOVA, DDSI were stratified by the socio-demographic variables in which participants who had high level of education (3.03) had significantly (P = .012) higher mean DDSI than their counterparts with low level of education (2.60). There was no significant association between DDSI with participants’ marital status (2.72 vs 2.33; P = .405); ethnicity (2.71 vs 2.73; P = .896); employment status (2.69 vs 2.82; P = .359); first pregnancy (2.86 vs 2.67; P = .290) husband’s employment status (2.73 vs 3.00; P = .677); and husband’s income earning status (2.71 vs 2.86; P = .454).
Pearson correlation between knowledge, attitude and iron-rich diet diversity scores.

Correlation is significant at the .05 level (2-tailed).
Correlation is significant at the .01 level (2-tailed).
Adjusting for possible confounders, multiple linear regression analysis was done to identify the determinants of iron-rich dietary diversity scores and presented in Table 5. Knowledge scores was significantly associated with iron-rich diet diversity scores of the participants (β = .02; 95% CI = 0.01-0.02).
Multiple linear regression of determinants of iron-rich diet diversity scores.

Adjusted R2 = .12.
Discussion
In this study we evaluated the consumption of iron rich foods and its determinants among pregnant women from a rural district in Northern Ghana. The commonly eaten iron-rich foods reported by the pregnant women were fish or other sea foods and green-leafy vegetables. Animal sources of iron were sparingly eaten by the pregnant women. The significant determinant of the intake of iron rich foods by the pregnant women was nutrition-related knowledge.
An important finding of this study was that fish or other seafoods (70.6%) was the most commonly consumed iron-rich food among the pregnant women. Of those, most of the pregnant women reportedly ate meals prepared with dried anchovies (known as ‘amani’ or ‘keta school boys’ in Ghana) and herrings. These 2 kinds of fish are commonly sold in Ghanaian markets and are generally affordable and can be stored for several days given that they are usually smoked and dried. It can thus be assumed that their affordability and the fact that they can be stored for long in their dry state made them a go-to source of iron. There is thus the need for health workers to continue to encourage pregnant women during routine antenatal care to eat more of these kinds of fish that are commonly available in the communities. For the other animal sources of iron, <5% and <30% of the pregnant women ate organ and flesh meats respectively. It is concerning that the consumption of iron-rich foods from animal sources was very low given that it may increase the risk of iron-deficiency anaemia among the pregnant women because haeme-iron which is the type of iron found in meat is more bioavailable than non-haeme iron which is found in plant sources.31,32 Furthermore, the absorption of haeme-iron is not as much affected by other food components of a meal as compared to non-haeme iron.33,34 The low consumption of these food sources of iron could be due to unaffordability of such foods as most of the pregnant women who reportedly said it was difficult to prepare iron rich foods cited unaffordability as a barrier. In poor rural communities such as the current study setting, farm animals are kept but not for consumption but for economic purposes. Community-level education and awareness programmes should thus be implemented to enable community members understand the causes and effects of iron-deficiency anaemia on the mother and child and how it can be prevented.
Regarding the plant sources, the commonly reported consumed iron-rich food was green leafy vegetables. Legumes was however consumed by only 27% of the participants. Green leafy vegetables are generally easy to come by in the study area given that they are staples. The pregnant women were reportedly familiar with diets from the green leafy vegetables and frequently described such diets as ‘green-green’. The 67% of the pregnant women who consumed green leafy vegetables is lower than the 33.7% reported among pregnant women attending antenatal care in Addis Ababa, Ethiopia 35 and the 44.5% among pregnant women receiving antenatal care at a tertiary referral hospital in Northern Ghana 24 but lower than 76.7% reported by Tibambuya et al 36 among pregnant women attending antenatal clinic in West Gonja, Ghana. The differences could be due to availability, affordability and seasonality of the green leafy vegetables.
The World Health Organization recommends the intake of a variety of foods during pregnancy including fruits.37 Vitamin C-rich fruits in particular are advised during pregnancy because vitamin C helps in the absorption and the bioavailability of iron by providing the appropriate pH.38,39 It is thus commendable that majority of the participants ate vitamin C-rich foods usually along with their meals or right after their meals. In addition, a large majority of the pregnant women also avoided coffee or tea that may impede the absorption of iron in the body.33,38,39 These findings are lower than the 66.9% of antenatal attendees in a general hospital in Lagos, Nigeria that drank tea in a study reported by Yesufu et al 40 ; the 75.3% of participants who took tea or coffee in a study reported by Wemakor 24 among pregnant women from Northern Ghana and the 46.9% who reportedly took coffee or tea immediately after their meals in a study reported by Oumer and Hussein. 41 The variations could be due to socio-economic, cultural and contextual differences. It is however an interesting conundrum that majority of the pregnant women in the current study did not know the foods that can improve or impede the absorption of iron in the body, although they consumed more vitamin C rich foods but limited the intake of tea and coffee. This probably suggests that these pregnant women ate vitamin C rich foods probably not to make iron more bioavailable in their bodies but for other reasons.
In the present study, we found that knowledge was significantly associated with the consumption of iron rich foods. This finding is consistent with those of Nana and Zema 42 who reported a significant association between dietary knowledge and health dietary practices among pregnant women from North Western Ethiopia and those of Mirsanjari et al 43 that reported a significant weak association between nutrition knowledge and dietary practices among pregnant women from Singapore. It is important to note that knowledge alone may not be enough to result in improved dietary practice but it is a necessary first step. The findings can be explained that having nutrition knowledge presupposes pregnant women’s’ understanding of the negative effects of iron deficiency anaemia to themselves and their unborn child as well as being able to identify rich sources of iron. There is thus the need for healthcare providers to continue to provide nutrition education and counselling to pregnant women during routine antenatal care.
This study is not without limitations. Its cross-sectional nature makes it difficult to establish causality. The use of a single study setting may affect the generalizability of the findings to other settings. Social desirability and recall bias may be present due to the use of a self-report instrument that required participants to recall. We also note our limitation of combining tea and coffee as food items that may inhibit the absorption of iron given that the evidence showing the inhibitory effects of coffee is variable although those regarding tea is well established. Notwithstanding this the study has important strengths. The study increases our understanding of the dietary practices of pregnant women regarding the consumption of iron rich foods and the factors that may be contributing to those dietary practices. The findings provide avenues that will inform the design of interventions to improve the dietary practices of pregnant women in the study setting and other developing countries that may have similar settings.
Conclusion
The consumption of iron rich foods from sea foods and plant sources was common but those from organ and flesh meats was less frequent. Nutrition knowledge may be an important determinant of dietary practices regarding the consumption of iron rich foods among pregnant women. Interventions that improve the nutrition knowledge of pregnant women may be a laudable strategy to improve the consumption of iron rich foods and subsequently the iron status of pregnant women.
Footnotes
Acknowledgements
Authors wish to thank the Nandom District Director of Health Services and the Medical director of the Nandom Hospital for granting them permission to have access to the premises and the study participants.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
NYA, VAA and VM formulated the research question(s), and designed the study, NYA and VAA undertook data collection, VM analysed the data and VM, SZ, MAA and AA wrote the article. All authors agreed for the manuscripts to be published in its current form.