
Abstract
Background:
Although orphans are at increased risk of undernutrition, studies assessing prevalence of undernutrition are limited to orphans residing with their relatives or on street. This study was conducted to assess magnitude of undernutrition and its associated factors among institutionalized school-age orphans in Harari Regional State, eastern Ethiopia.
Methods:
An institution based cross-sectional study was conducted among all school-age (6-12 years) orphans living in all orphan centers in Harari Regional State, eastern Ethiopia. Data were collected by using a structured pretested questionnaire supplemented with anthropometric measurements. Data were entered using EpiData 3.1 and analyzed using SPSS 22. Logistic regression models were fitted to identify factors associated with undernutrition. Statistical significance was declared at P-value <.05.
Results:
A total of 265 orphans residing in all orphan centers in the region were included. The prevalence of stunting, wasting, and underweight were 15.8% (95% CI: 11.9, 20.7), 10.9% (95% CI: 7.7, 15.3), and 8.7% (95% CI: 4.3, 10.5), respectively. Staying in orphan center for 6 to 10 years (AOR = 6.2; 95% CI: 2.6, 15.10), having recent illness (AOR = 3.9; 95% CI: 1.4, 10.4), and being aged 10 to 12 years (AOR = 11.2; 95% CI: 3.5, 35.4) were significantly associated with stunting whereas having recent illness (AOR = 4.3; 95% CI: 1.4, 7.3) and being aged 6 to 7 years (AOR: 10.4; 95% CI: 3.2, 33.6) were significantly associated with wasting. Underweight was more likely (AOR: 8.9; 95% CI: 2.7, 29.5
Conclusions:
Almost 1 in 6, 1 in 9, and 1 in 11 institutionalized school-age orphans in Harari Regional State were stunted, wasted, and underweight respectively. Younger children and those with recent illness were more likely to be undernourished. Underlying reasons for undernutrition among orphans being cared in orphan centers should be further explored.
Introduction
Globally, according to current estimates in 2019, 144 million children under 5 years of age were stunted, 47 million wasted and 38.3 million were overweight. 1 In Ethiopia, the recent 2019 Mini Ethiopian Demographic and Health Survey (EDHS) indicated that 37%, 7%, and 21% under 5 years age children were stunted, wasted, and underweight respectively. 2 In low-income settings, malnutrition contributes to more than half of all child deaths. 3 Undernutrition puts children at a greater risk of dying from common infections and increases the frequency and severity of infections. In addition, children with malnutrition experience developmental delays, weight loss, and recurrent illness. As such, the interaction between under nutrition and infection creates a potentially lethal cycle of worsening illness and deteriorating nutritional status among children. 4
Children who lost one or both of their parent(s)—orphans—are at increased risk of undernutrition because of lack of food, safe water, parental care, supervision, and protection. There were nearly 140 million orphans globally in 2015, of which 61 million were in Asia followed by 52 million in Africa.5-8 Majority of orphans were never breast fed at all or exclusively breastfed and are prone to infections. 9 The vicious cycle of infection and undernutrition among children is well established.10,11 Because of little or no external assistance, loss of parental care and poor hygiene, and inadequate amount and diversity of foods, orphan children are vulnerable to malnutrition.5-7,10
In addition, orphaned and institutionalized children may experience micro nutrient deficiencies resulting in weak immunity and thereby infections. Given orphan children are at highest risk of undernutrition risking their health and development, understanding the level and risk factors of malnutrition among this segment of population is an initial step for averting the problem.12,13 Although several studies on nutritional status of under-5 children in Ethiopia exists,14-22 little is known about orphan children in Ethiopia in general and eastern Ethiopia in particular. Therefore, this study was conducted to assess the prevalence of undernutrition and its associated factors among institutionalized school-age orphans in Harari Regional State, eastern Ethiopia.
Methods
Study setting
The study was conducted in 5 licensed private orphan centers—Save Our Souls (SOS) Children Village, Darulhijra Orphanage, Hotamisrak Orphanage, Harar Yahagerlij Charity, and Genet Orphan Center—in Harari Regional State, eastern Ethiopia. These centers are devoted for the care and rearing orphan children, including their schooling and health care services. The study was conducted from June to July, 2020.
Study design and population
An institution based cross-sectional study was conducted. All school-age (6-12 years) orphans residing Harari Regional State constituted the source population. The study population included all school-age orphans living in these centers during the study period.
The sample size was calculated by using single population proportion formula with the following assumptions: prevalence of stunting (19.7%) among institutionalized orphans and vulnerable children from previous study in Addis Ababa, 23 5% margin of error, 95% confidence interval. The final sample size for this study was 267 including 10% for non-response rate. We included all school-age orphans found in the centers during data collection. Accordingly 75, 80, 38, 60, and 12 orphans from Save Our Souls (SOS) Children Village, Darulhijra Orphanage, Hotamisrak Orphanage, Harar Yahagerlij Charity, and Genet Orphan Center participated in the study respectively.
Data collection
Data were collected by face to face interview using a pre-tested structured questionnaire adapted from previous studies.6,23-25 The questionnaire was administered using local languages—either Afaan Oromoo or Amharic. Data on sociodemographic characteristics, diet, and related information were collected from their care givers and the orphan center directors. In addition, height and weight were measured. Height was measured by using vertical wooden height board and recorded to the nearest 0.1 cm. The heels, buttocks, scapulae, and head were positioned in contact with the vertical backboard. Weight was measured with the child wearing light clothes and with no shoes. The weight scale was calibrated immediately before and during each measurement session and weight was recorded to the nearest 0.1 kg. Data were collected by trained 4 diploma nurses under the supervision of 2 BSc health professionals.
To minimize intra and inter-observer’s variability of the data collectors, relative technical error of measurement (TEM) was calculated during training among 10 school-age children to minimize random anthropometric measurement error. The accepted relative technical measurement errors for intra-observer and inter-observer were less than 1.5% and less than 2% respectively.
Data processing and analysis
Data on sociodemographic characteristics, hygiene, health related and dietary conditions were entered using EpiData 3.1 and exported to SPSS 22 for analysis. The data were sorted, summarized, cleaned and checked for missing values using frequencies and cross tabulations.
Height for age Z score (HAZ), weight for age Z score (WAZ), and body mass index for age Z score (BAZ) was generated using the World Health Organization (WHO) 2007 Anthroplus software. Children who fall below negative 2 (<−2SD) and negative 3 (−3SD) standard deviations from the median of the reference population were regarded as moderately and severely malnourished, respectively. 26 Stunting, wasting, and underweight were dichotomized as “yes = 1” and “no = 0.” Binary and multiple logistic regressions were used to check the association of independent variables with nutritional status. Statistically significant association was set at P-value <.05.
Ethical considerations
Ethical clearance was obtained from the Institutional Health Research Ethics Review Committee (IHRERC) of the College of Health and Medical Sciences, Haramaya University (Ref. No. IHRERC/122/2020). A formal letter of support from Haramaya University was submitted to the management of the orphan centers. Information about purpose and procedures of the study, potential risk and benefits was given to the care givers and center directors. Informed voluntary written consent was obtained from the center directors and then assent was sought from the children and the care takers after being informed about the study.
Results
Sociodemographic characteristics
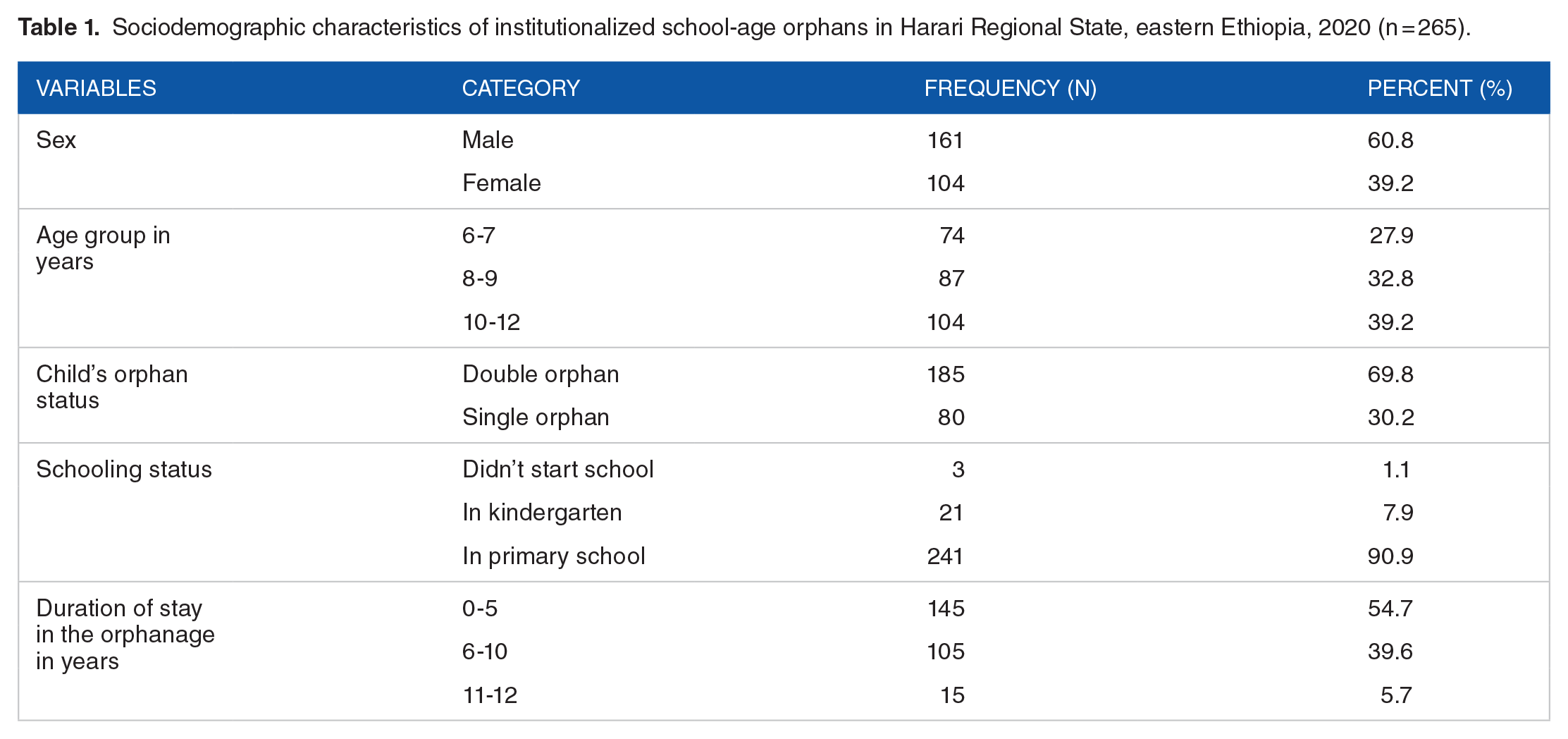
Of a total 267 orphans approached, 265 (99.3%) were included in the study. The mean (±SD) age of children was 107.8 (±23.3) months, ranging from 6 to 12 years. Majority of the children were in primary school (90.8%), males (60.8%) and stayed in the orphan centers <6 years (54.7%). Almost 7 out of 10 children were double orphans (who lost both parents). Details of sociodemographic conditions are summarized in Table 1.
Sociodemographic characteristics of institutionalized school-age orphans in Harari Regional State, eastern Ethiopia, 2020 (n = 265).
Hygiene and health related behavior
Care givers reported that 240 (90.6%) and 93.6% children had frequent hand washing after visiting toilet and frequent hand washing before meal respectively. However, only 136 (51.3%) reported using soaps during hand washing. Care givers reported that 40 (15.1%) of the children had recent illness.
Dietary characteristics
Regular 3 meals per day was reported by 238 (89.8%) care givers and few reported missing meals 24 hour prior to the study (Table 2).
Dietary characteristics of institutionalized school-age orphans in Harari Regional State, eastern Ethiopia, 2020 (n = 265).

Prevalence of undernutrition and its associated factors
The prevalence of stunting, wasting, and underweight was 15.8% (95% CI: 11.9%, 20.7%), 10.9% (95% CI: 7.7%, 15.3%), and 8.7% (95% CI: 4.3%, 10.5%) respectively. Stunting was highest among older children (10-12 years) while underweight and wasting were highest among young children (6-7 years) (Figure 1).

Prevalence of undernutrition among institutionalized school-age orphans in Harari Regional State, eastern Ethiopia, 2020 (n = 265).
Stunting
In the binary logistic regression age, duration of stay in the orphan center, history of recent illness, and not being satisfied with one’s meal were factors significantly associated with stunting. In the multiple logistic regression, however, only age, history of recent illness, and duration of stay in the orphan center remained independently associated with stunting. The odds of stunting among orphans with recent illness was 3.9 times (AOR = 3.9; 95% CI: 1.4, 10.4) higher compared to their counterparts. Stunting was 6.2 times (AOR 6.2; 95% CI: 2.6, 15.1) more likely among orphans who stayed in the center for 6 to 10 years compared to those less than 6 years. Orphans aged 10 to 12 years were 11.2 times (AOR = 11.2; 95% CI: 3.5, 35.4) more likely to be stunted as compared to orphans in ages of 6 to 7 years (Table 3).
Factors associated with stunting among institutionalized school-age orphans in Harari Regional State, eastern Ethiopia, 2020 (n = 265).

Wasting
In both binary and multiple logistic regression analyses, recent illness and age of orphans were significantly associated with wasting. Orphan children in the age group of 6 to 7 years were 10.4 times (AOR = 10.4; 95% CI: 3.2, 33.6) more likely to be wasted than those in age group of 10 to 12 years. On the other hand, the odds of wasting among orphans who had recent illness were 3.3 times (AOR = 3.3; 95% CI: 1.4, 7.3) higher than their counter parts (Table 4).
Factors associated with wasting among institutionalized school-age orphans in Harari Regional State, eastern Ethiopia, 2020 (n = 265).

Significant at P
Underweight
Presence of recent illness and duration of stay in orphan centers were associated with underweight in the binary logistic regression. In the multiple logistic regression, only presence of recent illness was significantly associated with underweight. School-age orphans who had recent illness were 8.9 times (AOR: 8.9; 95% CI: 2.7, 29.5
Factors associated with underweight among institutionalized school-age orphans in Harari Regional State, eastern Ethiopia, 2020 (n = 265).

Discussion
In this study, we assessed the prevalence of undernutrition and its associated factors among institutionalized school-age orphans in eastern Ethiopia. We found that 15.8%, 10.9%, and 8.7% of the orphans had stunting, wasting, and underweight, respectively. To the best of our knowledge, this is the first study to report nutritional status of school-age orphan children in Ethiopia. Orphans who stayed in orphan centers for 6 to 10 years and older (10-12 years) were more likely to be stunted while younger children (6-7 years) were more likely to be wasted and underweight. Orphans who reported recent illness were more likely to be wasted and underweight.
The prevalence of stunting in our study is consistent with findings reported in Cameroon, 27 Bangladesh, 28 and India. 7 It is, however, lower than Ethiopian national level data, 2 reports from Uganda, 29 Ghana, 30 and Bangladesh. 31 This variation might be due to differences in sample size, study designs, and variation in the age group. The Ethiopian national data was done among children under the age of 5 years, larger sample size was used in Ugandan study while the study participants in Ghanan study ranged 2 to 18 years which could contributed to the higher stunting. On the other hand, stunting reported here is higher than the findings from other studies.6,32-35 The possible explanation might be differences in the method of screening—as some used subclinical malnutrition which may increase undernutrition, differences in feeding habits, sample size variation, and socioeconomic characteristics.
In terms of prevalence, wasting in this study was similar with Ethiopian national level data, 2 findings from Kenya and Bangladesh.36,37 It is, however, higher than reports of studies from Hawassa, Ethiopia, 24 Cameroon, 27 Bangladesh, 31 and Ghana, 38 and lower than findings of other studies.33,34,39 This variation might emanate from differences in study design, sample size, and socioeconomic factors.
The prevalence of underweight from the current study was in agreement with findings from Ghana and Kenya.36,38 However, it is lower than Ethiopian national level data, 2 study reports from Nigeria, 34 Sri Lanka, 39 Kenya, 6 and Bangladesh. 40 This might be justified by the difference in the method of screening undernutrition, the use of different cut off point for classifications, and variation in sample size.
We found that the odd of stunting was higher among orphans who lived 6 to 10 years in the orphanages than their counterparts. This is in line with reports of other studies.6,41 However, it contrasts the finding of study from Bangladesh 31 and Addis Ababa, Ethiopia. 25 This disagreement could be due to difference in quality of diet served in the centers studied, and the overall poor care provided in the centers.6,7
Furthermore, orphans aged 10 to 12 years were more likely to be stunted. Similar findings were reported from other studies.6,25,27,41 This could be because stunting is irreversible and children will live with it throughout their life. This study revealed that recent illness has increased the odds wasting and underweight among the orphans. This was similar with previous studies.5,24,42 This is could be due to the inter-relation between infection and malnutrition.4,11
This study has shed light on undernutrition among school-age orphans in orphan centers. But, daily meal menus of the orphan centers which could influence undernutrition of orphans across the centers were not assessed. Recent illness was assessed only by history and could result in under reporting.
Conclusion
Almost 1 in 6, 1 in 9, and 1 in 11 institutionalized school-age orphans in Harari Regional State were stunted, wasted, and underweight respectively. Younger children and those with recent illness were more likely to be undernourished. Underlying reasons for undernutrition among orphans being cared in orphan centers should be further explored.
Footnotes
Acknowledgements
We would like to thank the study participants, individuals, and organization that supported us in conducting this study.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Authors’ Contributions
FM, IM, SGF, AKT, and FW designed the study, participated in data collection, analysis, interpretation, and critically reviewed the draft manuscript. SGF drafted the manuscript with continuous input from AKT and FW. All authors read and approved the final manuscript for submission.
Data Sharing Statement
All data used for this study could be obtained from the authors upon reasonable request.