
Abstract
Background and aims:
A worldwide increase in childhood overweight (OW) and obesity (OB) has been reported. OB is an inflammatory state which affects iron metabolism and the sensibility of the tests to detect iron deficiency (ID). Our aim was to evaluate the adequacy of current ferritin cut-offs to define ID in children with OW/OB.
Methods:
This cross-sectional study included 152 children (54% girls) aged (median [Q1-Q3]) 11 (8-13) years with OW/OB. Complete blood count and iron metabolism were evaluated. Low ferritin, transferrin saturation (TSat), and anemia were defined by age- and sex-specific cut-offs recommended by National Guidelines. Iron intake was assessed in a subgroup (n = 80) by a 24-hour dietary recall. Analyses were made according to pubertal development and ferritin tertiles.
Results:
The overall prevalence of low ferritin, TSat, and anemia was 2.6%, 23.8%, and 5.2%, respectively. Among pre-pubertal children (n = 87), the frequency of low TSat rose across ferritin tertiles (P < .05), whereas it decreased among pubertal children (n = 65; P < .005). Cases of anemia among pre-pubertal children were found in the highest ferritin tertile, whereas 4/6 anemia cases in pubertal children were found in the lowest ferritin tertile (<39 µg/L). Pubertal children within the lowest ferritin tertile + low TSat (n = 11) showed lower hemoglobin (–9%; P < .005) and hematocrit (–8%, P < .01) than those in the same tertile + normal TSat (n = 16). The overall prevalence of children with ferritin < 39 µg/L + low TSat was 9.2%.
Conclusions:
Higher ferritin cut-off values are required to define ID in children with OW/OB. Such cut-off remains to be validated in larger, multi-ethnic cohorts of children with OW/OB.
Introduction
Iron deficiency (ID) is one of the most common micronutrient deficiencies worldwide and is considered to be responsible for around 25% to 50% of all the cases of anemia.1,2 Other health implications associated with ID, besides those related with anemia, include cognitive impairment during development, tiredness, dizziness, irritability, and sexual dysfunction in adults.3,4 ID is a developing pathological state which may progress from pre-latent and latent states to ID anemia, which is characterized by ID erythropoiesis and finally low hemoglobin (Hb) concentration. 5 One of the most important biomarkers used to define pre-latent and latent ID is low serum ferritin concentration. Other markers that can be altered in latent ID are transferrin saturation (TSat), mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH), and red blood cell distribution width (RDW). Although ferritin is the most sensitive parameter to detect ID, its major limitation is that under inflammatory conditions ferritin behaves as a positive acute phase reactant and its plasma concentration rises. 5
On the other hand, childhood overweight (OW) and obesity (OB) is another major health concern and its prevalence has been rapidly increasing in the last few years. 6 OB is now recognized as a low-grade proinflammatory state established by an altered secretion of adipocytokines. Among the proinflammatory mediators secreted by adipocytes in OB, low adiponectin and high interleukin (IL)-6 and tumor necrosis factor (TNF)-α are remarkable. Such mediators induce the secretion by hepatocytes of other acute phase reactants such as alpha-1 acid glycoprotein, C-reactive protein (CRP), and the major regulator of iron homeostasis, hepcidin, among others. Thus, inflammation in OB subjects promotes the expression of hepcidin which in turn reduces iron absorption and serum iron.7,8 Indeed, higher hepcidin levels and lower iron bioavailability and absorption were reported in children with OB in comparison with their normal-weight counterparts.8–10 In particular, Zimmermann et al 10 analyzed data from 4 controlled efficacy trials of iron fortification in children and observed that higher baseline body mass index (BMI) z-scores impacted negatively the total body iron outcomes by the end of the trial (as assessed by the change in the soluble transferrin receptor/ferritin ratio). Then, some studies found that children with OB are at an increased risk of ID in comparison with normal-weight children.11–14 However, in most of these studies, the definition of ID was rather heterogeneous using different combinations of serum iron, ferritin, and/or TSat. 13
Under the inflammatory conditions of OB, the use of ferritin to define ID in OB subjects is a matter of debate. 13 To sort this inconvenience, some authors proposed a correction to serum ferritin levels to accurately define ID in the context of OB epidemics 15 as in the presence of subclinical inflammation. 16 Such an approach has already been suggested in regions where infections are common and the World Health Organization (WHO) recommended a higher ferritin cut-off (<30 ng/mL) to define ID. 17 The suitability of such approach in children with OB has not been explored yet. Our aim was to evaluate the adequacy of the current ferritin cut-off to define ID in a cohort of children with OW/OB.
Materials and Methods
Study design and population
This study was a cross-sectional analysis of an ongoing prospective study which consecutively included every child between 5 and 17 years with OW or OB who consulted the Pediatric Diabetes and Nutrition Service of the Complejo Médico Churruca Visca, Buenos Aires, Argentina, from April 2017 to April 2018. Patients were excluded if any of the following was present: diabetes, hypothyroidism or treatment with levothyroxine, concomitant autoimmune or liver pathologies, and evidences of any acute infection as assessed by high sensitivity C-reactive protein (hsCRP) > 10 mg/L. 18 From 161 studied children, 9 were excluded (1 with current overt hypothyroidism, 3 with celiac disease, 3 with hsCRP > 10 mg/L, and 2 who refused to participate in the study) and 152 were included in this analysis.
Interview and clinical assessment
All the eligible patients were interviewed in a joint session by a pediatrician and a nutritionist to explain the study protocol and their aims. After the parent and their child signed the informed consent and assent forms, respectively, the patients were referred for the initial evaluation. Height and weight were measured with the patient without shoes and wearing light clothes and in a subsample (n = 80) a single 24-h dietary recall was performed. Portion sizes were estimated with the use of a visual guide of food portions and weights (International Life Science Institute, Argentina). The intake of each macronutrient and micronutrient was calculated using the food chemical composition from the Sistema Argentino de Registro Alimentario (SARA; Ministerio de Salud de la Nación). Low iron intake was defined according to the Estimated Average Requirement (EAR) published by the Institute of Medicine, National Academies. 19 To correct for dietary underreporters, iron intakes were adjusted for energy intakes and expressed as iron μg/kcal. BMI was calculated and z-scores determined according to the growth tables of the WHO. 20 OW was defined as z-BMI between +1 and +2, OB as z-BMI between +2 and +3, and severe OB as z-BMI > +3, as established by the WHO. Pubertal development was assessed by Tanner 21 criteria. For this study, puberty was defined by a Tanner stage > I in children aged >10 years or less if signs of pubertal development were present. The study protocol was conducted following National (Disp. 1480/11 from the Ministerio de Salud de la Nación) and International (Helsinki Declaration) Guidelines and was approved by the Ethics Review Board of the Complejo Médico Churruca Visca.
Biochemical assessment
Blood samples were drawn after a 12-hour overnight fast. The complete blood count (CBC) was performed in a multi-parameter automated hematology analyzer (CELL-DYN Ruby; Abbott, USA). Plasma glucose, lipids, iron, and transferrin levels were determined in a UniCelDxC 800 chemistry autoanalyzer (Beckman Coulter, USA). TSat was calculated from serum iron and transferrin concentrations, and ferritin levels were assessed in an automatic immunoassay analyzer (Architect i1000sr; Abbot). HsCRP concentration was measured by nephelometry (Immage, Beckman Coulter, USA) The cut-off values of Hb, MCV, TSat, and ferritin levels were taken from the guidelines of the Argentine Society of Pediatrics 22 and are shown in Table 1. Low MCH was defined as <25 pg and elevated RDW as >15%.
Cut-off values from the Argentine Society of Pediatrics.

Hb, hemoglobin; MCV, mean corpuscular volume; TSat, transferrin saturation.
For these parameters, age groups are defined in guidelines as 5-10 years, 11-14 years, and 15-18 years.
Sample size
For sample size calculation, we used the national estimates of ID in school-aged children which are around 10%. 23 Then, we calculated the sample size needed to estimate 10% of ID cases with an error (α) of 0.05 and a 95% confidence interval. The resulting minimum number of subjects to be included in the study was 139. The OpenEpi software (Emory University, USA) was used for sample size calculation.
Statistical analysis
Statistical analyses were mostly performed dividing between pre-pubertal and pubertal children. Also the whole study population was divided according to ferritin tertiles. Continuous variables were tested for normality using the Shapiro-Wilk test. Trends across ferritin tertiles were evaluated using linear contrasts in analysis of variance (ANOVA) tests after log-transformation of skewed variables. Correlations were tested by Pearson or Spearman test according to data distribution. Differences in proportions between 2 groups were assessed by Fisher exact test. Trends of categorical variables across ferritin tertiles were evaluated by chi-square test. Receiver operating characteristic (ROC) curve analysis was performed to evaluate ferritin cut-off points with the best sensitivity and specificity to detect a TSat < 15%. SPSS 17.0 (IBM, USA) was used for statistical analyses.
Results
The studied population involved 152 children aged (median [Q1-Q3]) 11 (8-13) years, of which 54% were girls. The prevalence of OW, OB, and severe OB was 16%, 52%, and 32%, respectively. The frequency of anemia, low MCV, MCH, TSat, ferritin, and high RDW in the study sample is shown in Figure 1.

Prevalence of hematological and iron metabolism alterations in children with OW/OB (n = 152).
The most prevalent alteration of the CBC was low MCV followed by low MCH. The overall prevalence of anemia was rather low despite the fact that almost 25% of the sample featured low TSat. Low ferritin concentration according to the Argentine Society of Pediatrics definition was rare and only observed in 2.6% of the total population (these cases were female children). As expected, ferritin concentration correlated with z-BMI (r = 0.18, P = .025) and with inflammatory markers: hsCRP (r = 0.35, P < .001) and white blood cell count (WBC; r = 0.22, P = .005). No significant correlation was observed between ferritin and Hb or any other hematimetric index (P > .05). On the other hand, TSat was correlated with hematological markers: Hb (r = 0.31, P < .001), MCV (r = 0.28, P < .001), MCH (r = 0.28, P < .001), and RDW (r = –0.23, P = .004), as well as with z-BMI (r = –0.19, P = .020) and WBC (r = –0.33, P < .001).
Differences between pre-pubertal (n = 87) and pubertal children in hematological and iron metabolism markers (n = 65) were assessed. Low MCV was more frequently found in pre-pubertal children (27% vs 10%, P = .007), whereas low ferritin (0% vs 6%, P = .032) was more frequent in the pubertal group. To further evaluate the association between ferritin and hematological and iron metabolism markers, we divided the study population according to ferritin tertiles among pre-pubertal and pubertal children (Table 2). Among pre-pubertal children, only a positive trend for WBC was observed. On the other hand, significant trends in pubertal children regarding Hb, TSat (both positive), and transferrin (negative) concentration were noticed. No significant trends regarding iron intake values in the pre-pubertal and pubertal groups (P > .05) were observed. A positive trend was observed across ferritin tertiles for hsCRP concentration only in pubertal children (Table 2).
General characteristics of the study population divided according to pubertal development.
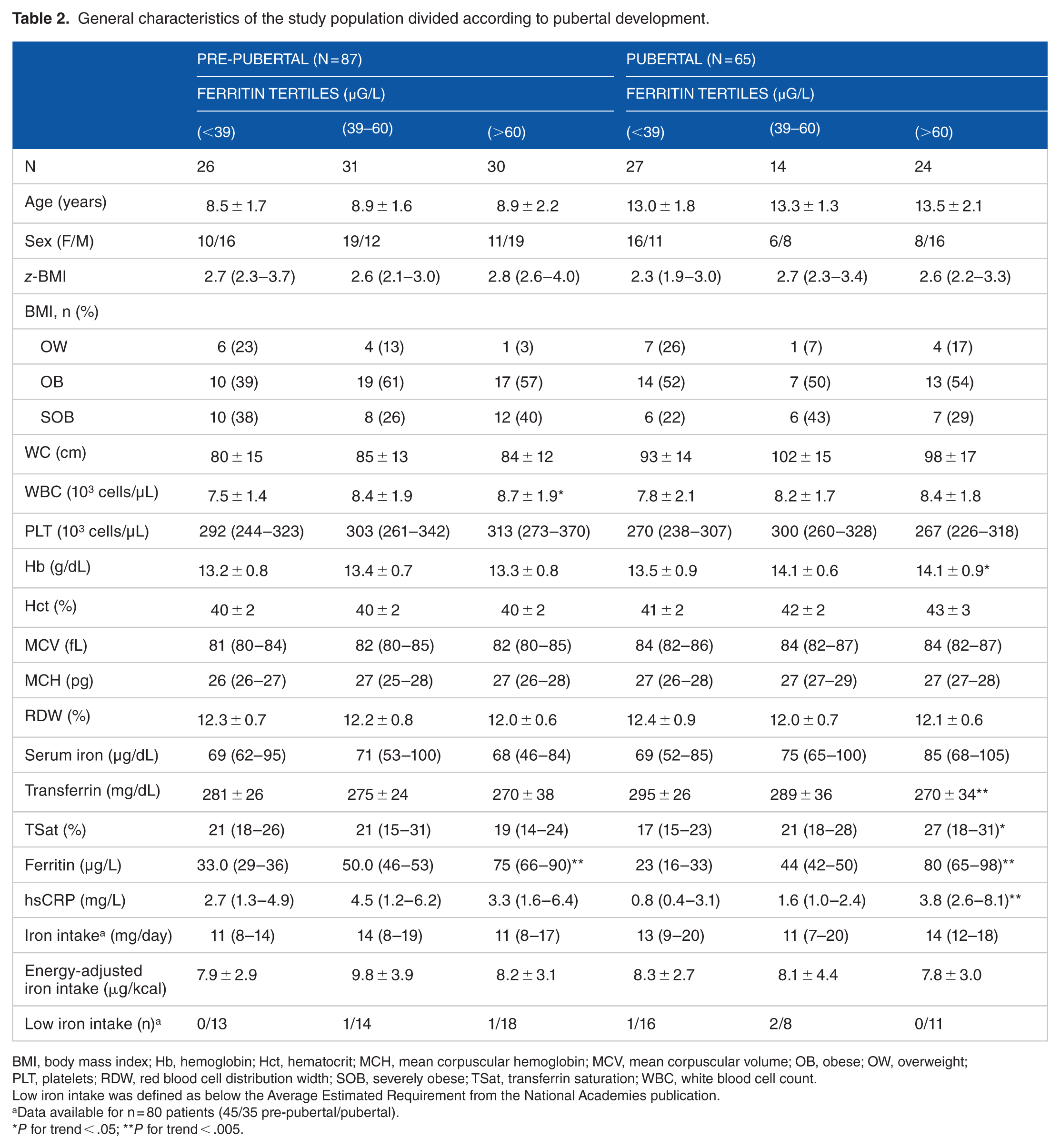
BMI, body mass index; Hb, hemoglobin; Hct, hematocrit; MCH, mean corpuscular hemoglobin; MCV, mean corpuscular volume; OB, obese; OW, overweight; PLT, platelets; RDW, red blood cell distribution width; SOB, severely obese; TSat, transferrin saturation; WBC, white blood cell count.
Low iron intake was defined as below the Average Estimated Requirement from the National Academies publication.
Data available for n = 80 patients (45/35 pre-pubertal/pubertal).
P for trend < .05; **P for trend < .005.
When evaluating the sex- and age-specific cut-off values of hematological and iron metabolism markers across ferritin tertiles, opposite trends in low TSat between pre-pubertal and pubertal children were observed (Figure 2). No other significant trends across ferritin tertiles were noticed in the prevalence of anemia, low MCV, MCH, and high RDW; all P > .05). ROC curve analysis to identify a relevant ferritin cut-off associated with low TSat showed significant results only in pubertal children. In this group of children, a ferritin < 39 μg/L identified cases of low TSat with a sensibility of 0.69 and a specificity of 0.79 (area under the curve [AUC] [95% confidence interval]: 0.76 [0.62-0.91], P < .01). This value was concordant with the definition of the lowest tertile of ferritin.

Prevalence of low transferrin saturation across ferritin tertiles in the pre-pubertal (n = 87) and pubertal (65) children with overweight/obesity.
Out of the 8 cases of anemia, 2 were found among the pre-pubertal children and belonged to the highest tertile of ferritin. The other 6 cases were found among pubertal children and were distributed 4/1/1 across the ferritin first, second, and third tertiles, respectively.
Finally, among pubertal children with ferritin < 39 µg/L, those with (n = 11) and without low TSat (n = 16) were compared. Sex distribution was not different between the groups (P > .05). Pubertal children with low TSat + ferritin < 39 µg/L showed lower Hb (12.8 ± 1.1 vs 13.9 ± 0.6 g/dL, P = .004), hematocrit (39% ± 2% vs 42% ± 2%, P = .015) and higher RDW (12.9 ± 1.1 vs 12.1 ± 0.6, P = .009) than the other group. Accordingly, all the cases of anemia within this ferritin tertile were found in this group of children with low TSat + ferritin < 39 µg/L.
The overall prevalence of low TSat + ferritin < 39 µg/L was 9.2% (14/152), which was 3.5-fold higher than that of low ferritin.
Discussion
This study shows that the ferritin values suggested in guidelines to define ID displayed scarce utility in children with OW/OB. Among pre-pubertal children with OW/OB, low TSat values were more frequent in those within the highest ferritin tertile, attesting for hypoferremia due to an inflammatory state rather than ID. Conversely, low TSat was more frequent in pubertal children within the lowest ferritin tertile, situation compatible with ID. In addition, half of the cases of anemia in this entire cohort belonged to the group of pubertal children with low TSat + ferritin < 39 µg/L.
Our results are in line with the study of Nead et al 11 that suggested modifying the guidelines for screening for ID to include children with elevated BMI. In their study, which was based in NHANES III, the overall prevalence of ID was 5.4% among children with OW/OB, lower than the overall prevalence of low TSat (23%) and of the combination of low TSat + ferritin < 39 µg/L (9%) in our study. However, low TSat alone is not a rare finding in children with OW/OB and other studies showed variable prevalence ranging from 20% to 40%.12,24,25 The challenge in children with OB is to distinguish between the two situations that goes by with low TSat: ID, and hypoferremia due to inflammation.5,13 Soluble transferrin receptor is one of the possible biomarkers which can be used in this regard; however, high costs and low standardization do not support its evaluation in most of the clinical laboratories. 26 In a cross-sectional analysis including 876 European adolescents from the HELENA cohort study, Ferrari et al 27 using a transferrin receptor definition showed 8.2% of ID prevalence among the group of 181 adolescents with OW/OB. Such estimate is close to the 9.2% value observed in this analysis. Then, the use of a higher ferritin cut-off to back low TSat values still remains a plausible strategy to detect ID cases among children with OW/OB.
The clinical implications of this study arise from the fact that using the currently suggested ferritin cut-off the prevalence of ID was only 2.6%, whereas when using both low TSat + ferritin < 39 µg/L the value almost tripled such frequency. It can be argued against the rather low ferritin cut-off from the Argentine Association of Pediatrics; however, when the ferritin cut-off suggested by the WHO was used instead, low ferritin ( < 15 μg/L) was observed in 4.6%, still half of the combination of low TSat + ferritin < 39 µg/L. Then, in the context of OB epidemics, the detection of ID could pass unnoticed in many children. The pubertal children presenting with ferritin < 39 µg/L without low TSat could resemble the state of pre-latent ID, in which hematological markers display only minor alterations.
Our findings were limited to the pubertal group as only 3 pre-pubertal children showed low TSat and ferritin < 39 µg/L, and no further comparisons were made. In this group of pre-pubertal children ID was rare. This fact could be explained through lower iron requirements compared with pubertal children, as iron intake was not different between pre-pubertal and pubertal children. Another possible explanation for the lack of ID cases among pre-pubertal children in comparison with other studies could rely on the dietary habits of Argentinean population, which includes elevated intakes of red meat. Even though ID was rare among this group of children, low TSat was prevalent and TSat values were significantly correlated with hematological indices. Then, hypoferremia and anemia of inflammation could be a relevant physiopathological event in pre-pubertal children with OW/OB, as also noticed by others.9,28 In agreement, a recent study showed that obese pre-pubertal children presented higher hepcidin and lower ferroportin concentrations in comparison with normal-weight children. 29
Analysis of iron intakes suggests low iron absorption as an important contributor to ID in this cohort of children with OW/OB. Accordingly, Cepeda-Lopez et al 14 found that CRP levels instead of iron intake were a major contributor to low serum iron and high total iron binding capacity in a Mexican Nutrition Survey which included 1174 children. More importantly, the results of Zimmermann et al 10 highlight the detrimental effects of OW/OB on iron absorption in controlled iron fortification trials.
Some of the limitations of this study rely on the fact that female and male children were analyzed altogether. Also, although pubertal development was considered for the analyses, we did not consider differences between Tanner stages II to V among pubertal children. These decisions were based on the lack of statistical differences between sex and age across ferritin tertiles and on the low number of patients in each group that could result if all the categories were to be considered. Furthermore, dietary assessment through a single 24-hour dietary recall has its inherent limitations (ie, dietary underreport) and significant correlations between iron metabolism markers and micronutrient intakes could have been gone unnoticed. Nonetheless, the dietary assessment was mainly conducted to check iron adequacy of the diets, which was the case for a large proportion of the sample. Neither crude iron intake nor energy-adjusted iron intakes were correlated to hematological, iron, or inflammation markers. Another limitation was the lack of data on hemoglobinopathies in studied patients. Structural or quantitative alterations in Hb chains could have affected the prevalence of altered hematimetric indices in this sample. However, the impact of these conditions over TSat and ferritin, the main variables of our analysis, is minor and do not affect our main conclusions. Finally, the lack of measurement of soluble transferrin receptor and/or hepcidin levels limited the validation of our proposed definition of ID. Then, our conclusions are limited to the fact that a different ferritin cut-off (higher than the ones currently proposed) should be used to screen ID in children with OW/OB. The final confirmation of ID diagnosis would require a soluble transferrin receptor or hepcidin measurement.
The major strength of this study relies on the studied cohort which only included children with OW/OB. As the lifestyle habits of OW/OB children are particular in sedentary behavior and fruits and vegetable intakes,30,31 the exclusion of all the individuals with normal weight was crucial to explore a clinically relevant ferritin cut-off for this population. Also, iron intake was not different between pre-pubertal and pubertal children and no correlations were observed between iron intake and hematological or iron metabolism markers; thus, highlighting the role of elevated BMI. A particular ferritin cut-off must be validated in larger studies and in cohorts with different genetic and cultural backgrounds.
In conclusion, higher ferritin cut-off values are required to define ID in children with OW/OB. Current ferritin cut-off values could miss at least half of the ID cases in this population. In OB children, ferritin (with an adequate cut-off) plus TSat should be used to screen ID in this clinical context. An exact ferritin cut-off remains to be validated in larger, multi-ethnic cohorts of children with OW/OB.
Footnotes
Acknowledgements
The authors would like to thank all the nurses and staff of the Pediatric Diabetes and Nutrition Service and of the Central Laboratory of the Complejo Médico Churruca Visca, Buenos Aires, Argentina. They would also like to thank the collaboration of the heads of the Central Laboratory Dr Pascual Ladelfa and Dr Laura Judcovski and the Fundación “Alberto J Roemmers” for financial support.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The present study was partially supported by a grant from the Fundación “Alberto J Roemmers”.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
MLM, ELC and FF performed the biochemical assessments. MLM, FF, ELC, MPS and TM done the statistical analyses and wrote the first draft of the manuscript. LK, IL, EA, JF, SP, LB and MPS performed the general clinical evaluation and recruited the patients. IL, JF, SP and LB carried out the 24-h dietary recall. LK and MPS reviewed the recruitment of patients and ethical aspects of the study. LK, EA, MPS and TM conceived the study, and participated in its design and presentation to the Ethical Review Board of the Complejo Médico Churruca Visca. MLM, FF, SP and TM revised the manuscript until its final version. All authors read and approved the final manuscript.