
Abstract
The measurement of resting energy expenditure (REE) is important to both human physiology and nutrition. There are several pre-conditions for the proper measurement of REE, but a key criterion is that it takes place in the thermoneutral zone (TNZ). Deciding whether a person is in his or her TNZ is not an easy task, and a suggested way forward is the monitoring of forearm to fingertip skin temperature gradients (FFG). In this commentary, we highlight our recent findings that FFG varies between individuals even when measured at a temperature within TNZ. Interestingly, FFG showed a consistent direct relationship with adjusted REE, in both cross-sectional and longitudinal study designs. In addition, we provide new findings that FFG is sensitive to small ambient temperature variations within the TNZ, in comparison to visual analogue scale (VAS)-derived subjective measures of thermal comfort. While further research is needed in this area, our view is measurements of FFG should be included in REE protocols. This would inform investigators on how their participants are responding to the ambient room temperature and also allow appropriate statistical adjustments in REE for between-group comparisons.
Keywords
Resting energy expenditure (REE) or resting metabolic rate (RMR) is the least amount of energy expended to maintain bodily functions in the awake state, with 50% or more of this energy directed towards the maintenance of core body temperature.1,2 Conceptually, REE/RMR is similar to basal metabolic rate (BMR) with the same pre-requisites for its measurement, except one. In research laboratories, BMR is measured soon after waking and so necessitates an overnight residence at the laboratory. When participants arrive at the clinic/laboratory early morning and undergo a mandatory 30-minute rest, the resulting measurement is termed REE and is ~5% higher than BMR as classical measured. Clearly, in a hospital/clinic-based setting where patients cannot undergo an overnight 12-hour fast or cannot meet other specific pre-requisites due to their disease condition, the term REE is used. In all these situations, a key requirement for the measurement of BMR/REE based on the principle of indirect calorimetry, is that it is conducted in the TNZ. 3
The TNZ is a range of ambient temperature, where the body temperature can be maintained without recourse to increased thermogenesis or sensible heat loss. For a lightly clothed person, the TNZ is accepted to range from 23-27°C, 4 but it is modulated by age, gender, clothing, and body composition. 5 Much of the vasomotor control within the TNZ is brought about through changes in skin blood flow. The opening of arteriovenous anastomoses in the glabrous skin of palms directs blood flow to the skin’s superficial capillaries and assists in heat loss. In a normally clothed person, this and other areas (ventral surface of fingers, forehead etc.) are exposed to the ambient temperature and hence contribute immensely to heat regulation in the TNZ. Overall, it would be expected that within the TNZ, peripheral skin blood flow would vary but neither vasodilation nor vasoconstriction would dominate. 5 It is difficult to objectively determine the TNZ in every individual, but monitoring of FFGs has been recommended as a way forward6,7 and correlates very well with fingertip blood flow in responses to ambient temperature changes. 8
In a recent study, 7 we noted a wide range of FFG during REE measurements made at a controlled temperature of 25°C. These ranged from a value that would suggest net vasodilation (–4.25°C) to net vasoconstriction (+7.8°C) across the individuals studied, which in turn would account for a wide range in fingertip flow at rest. 8 To control for many between-subject factors in that study, we included factors known to influence REE 3 in a backward linear regression analysis. These factors were age, gender, fat mass (FM), fat-free mass (FFM), waist circumference, season, physical activity, vitamin D status (25OHD), an index of insulin sensitivity, and metabolic syndrome status. We found that each °C increase in FFG was associated with an increase in REE by 63 kJ/day, 95% confidence interval (CI): 14.4-112.1; P < .012, where the final adjusted model included age, FM, FFM, and insulin sensitivity. 7 Interestingly, in a smaller subset of 29 participants who were re-measured after a period of 6 months, we observed that the change in FFG also made a direct contribution to adjusted change in REE. Overall, both cross-sectional and longitudinal designs offered the same direct relationship between these two variables. 7
In that study, we had also tested whether more complex models provided a better understanding of the relationship between FFG and REE (Figure 1). Essentially, the cubic relationship implied that there could be a range of FFG for which no discernable change in adjusted REE would be seen. However, above the upper end of this range, REE would increase, whereas below the lower end of the range, the REE would decrease.

Relationship of adjusted RMR to FFG: cross sectional data.
The question arose whether several individuals were potentially not in their TNZ even though they were all measured at 25°C. One explanation could be that TNZ may have shifted upwards in some; therefore, 25°C was sensed as ‘cool/cold’ which necessitated some vasoconstriction (more positive FFG) and thermogenesis. At the other extreme of the relationship, 25°C was sensed as ‘warm/hot’, so a fair number responded with a vasodilatory response and a lowering of REE (Figure 1). A mathematical solution of that cubic equation indicated that the range was 0.40°C-2.48°C for these data. This is not readily appreciated on visual inspection of Figure 1, where the limits appear wider. Clearly, there is the need for larger sample sizes to confirm and extend these findings and for investigators to study different ambient temperatures within TNZ.
The thermal comfort zone (TCZ) is considered to be similar to TNZ, since it responds to similar inputs and is aimed at defending core temperature. However, it differs from the TNZ in being more dependent on behavioural regulation than autonomic regulation. Kingma et al. 5 have argued that the TCZ is much narrower than TNZ and may act well before TNZ is reached. While this is operative in free-living situations in defence of core body temperature, in most laboratory-based trials, the full extent of this behavioural response is possibly curtailed due to the need for compliance to the study protocol imposed. Therefore, from a practical viewpoint, it was pertinent to gauge how indicators of thermal comfort compared against the FFG during a standardized REE protocol.
We had transitioned a group of men and women through three temperatures: 20°C, 25°C, and 27°C in a random order on different days for a 1.5-hour exposure at each temperature. 9 We had asked each participant to rate their thermal comfort at each ambient temperature based on three recommended questions. 10 The data in Table 1 showed that there was a distinct within-subject response. Participants preferred both 25°C and 27°C relative to 20°C in their ratings of ‘agreeable’, ‘discomfort,’ and ‘irritable’, with no discernable difference between the two warmer temperatures. In contrast, FFG measured at these temperatures showed a clear and significant separation of effects between 25°C and 27°C (Table 1). Therefore, while it was possible for a larger change (here 5°) to be reflected in all elements of the visual analogue scale (VAS) questionnaire, measures of FFG were able to capture much smaller temperature perturbations.
Subjective measures of thermal comfort and forearm to fingertip skin temperature gradients following a 1.5 hours exposure to three ambient temperatures.
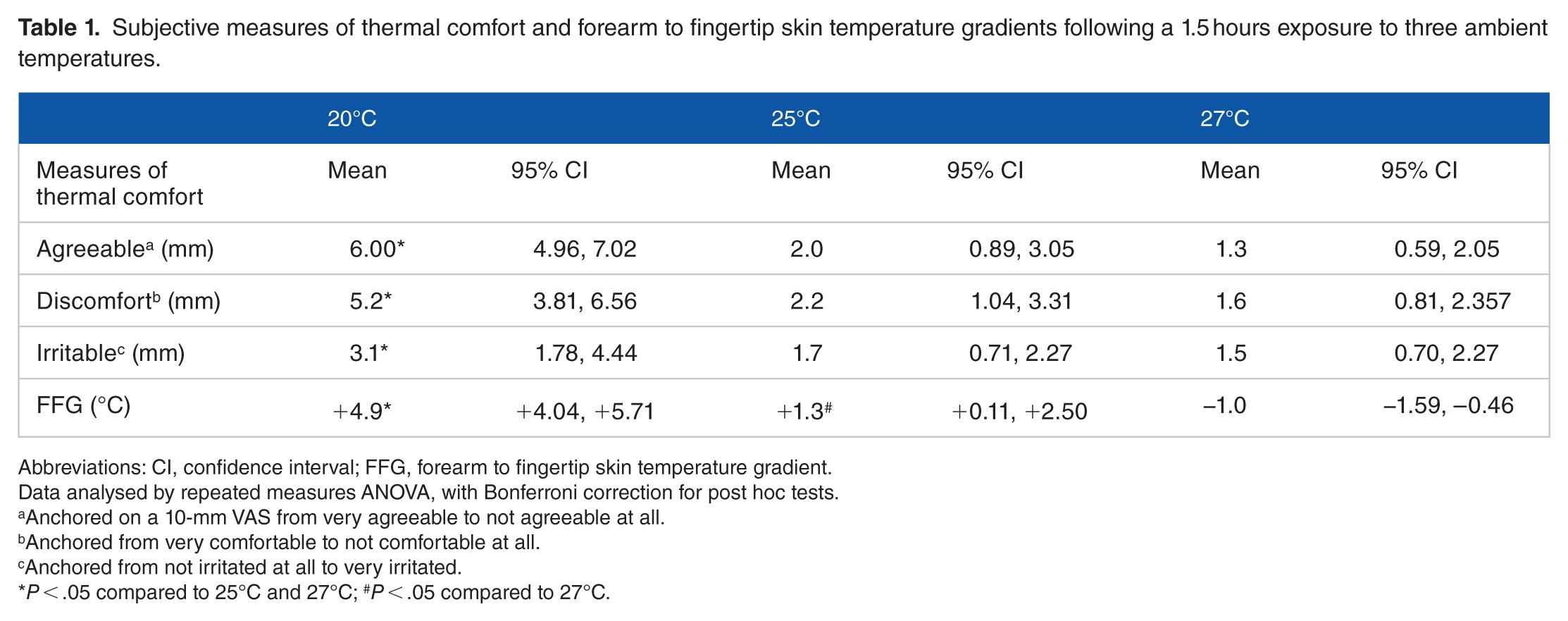
Abbreviations: CI, confidence interval; FFG, forearm to fingertip skin temperature gradient.
Data analysed by repeated measures ANOVA, with Bonferroni correction for post hoc tests.
Anchored on a 10-mm VAS from very agreeable to not agreeable at all.
Anchored from very comfortable to not comfortable at all.
Anchored from not irritated at all to very irritated.
P < .05 compared to 25°C and 27°C; #P < .05 compared to 27°C.
In summary, a basic but critical requirement for a valid measurement of REE is a judgement on whether the person is being measured in his or her TNZ. Our view is that FFG is a useful physiological measure that is sensitive to minor changes in ambient temperature and would inform the investigator of how each participant was interacting with the set temperature in the laboratory or clinic. We have previously used such information on FFG to adjust for potential differences in REE between groups. 11 There is clearly a need for more research in defining whether there is an optimal range of FFG across which REE may remain steady. That knowledge would inform the investigator whether their participant was actually in their TNZ. Future work is suggested across diverse ethnic groups, body fatness, winter/summer, and over a wider range of temperatures within conventional TNZ.
Footnotes
Acknowledgements
The authors thank Dr Yun Zhao for useful discussions.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
MJS and KP planned and co-wrote the manuscript.