
Abstract
Objective:
We assessed what predicts nutritional adequacy at day 14 following implantation of left ventricular assist device (LVAD).
Method:
We retrospectively reviewed the cases of 97 adult patients who underwent LVAD implantation at our institution from June 2011 to June 2016. We divided the patients into two groups based on the administered enteral nutrition (EN) calories on post-operative day (POD) 14: the EN calories of group SEN (sufficient enteral nutrition) were >80% of their total target calories, or the EN calories of group IEN (insufficient enteral nutrition) were <80% of their total target calories. We compared the two groups in terms of the perioperative factors within 1 week after surgery.
Results:
Groups SEN and IEN consisted of 53 and 44 patients, respectively. The mean doses of adrenaline and noradrenaline, mean central venous pressure (CVP), duration of nitric oxide administration, and mean residual gastric volume during 1 week after surgery in group SEN were significantly lower than those in group IEN (P < .05). In multivariate analysis, higher CVP during 1 week after surgery was identified as an independent risk factor for delayed EN on POD14 (odds ratio, 1.40; 95% confidence interval, 1.11-1.66; P = .0037). Total bilirubin, occurrence of acute kidney injury, and mixed venous blood saturation during 1 week after surgery were not significant predictors for EN on POD14.
Conclusions:
Increased CVP within 1 week after LVAD implantation was an independent factor for reduced EN feeding.
Keywords
Background
Left ventricular assist device (LVAD) is an advanced treatment for patients with severe heart failure refractory to medical treatment. LVAD technology has been widely used with aims of being a bridge to transplantation, a destination therapy, and a bridge to recovery. Despite benefits from this progressive therapy, many complications have occurred because of its increased use. 1
One of clinical issues after LVAD implantation is intolerance of enteral nutrition (EN) feeding. Underfeeding is an important problem encountered in cardiac surgery, including LVAD implantation. Postoperative nutritional management may represent an important factor for clinical outcomes in patients undergoing cardiac surgery. Many studies, including meta-analyses, showed that early EN can reduce mortality or infectious complications in critically ill patients.2,3 EN has been shown to have beneficial effects on immune function, wound healing, and intestinal mucosa integrity, which can prevent increased mucosal permeability and bacterial translocation. 4 Guidelines, such as the American Society for Parenteral and Enteral Nutrition (ASPEN) and the European Society for Clinical Nutrition and Metabolism (ESPEN), recommend the initiation of early EN for critically ill patients.5,6
Although there is no randomized controlled trial, ASPEN recommends that patients in hemodynamic compromise (eg, requiring high-dose catecholamines, large volume fluid, or blood products) should not be started with EN until they become stable because of the risk of gut ischemia. 5 ESPEN does not comment on EN for patients who are hemodynamically unstable. In 2017, the European Society of Intensive Care Medicine (ESICM) has published a guideline on the initiation of early EN for critically ill patients. The guideline generally recommends the initiation of early EN in patients in shock; however, these patients should be carefully monitored, and EN should be delayed in patients with uncontrolled shock. 7 Evidence for appropriate EN progression for hemodynamically unstable patients is still lacking, and further studies are required.
Hemodynamic instability in patients after LVAD implantation can easily occur because of right ventricular (RV) dysfunction. Circulatory compromise including RV dysfunction can lead to gastrointestinal disturbance, 8 which causes ventilator-associated pneumonia (VAP) and intestinal ischemia. However, EN after LVAD implantation has never been well studied. In this study, we examined retrospectively the influence of medical outcomes on EN progression after LVAD implantation.
Methods
This study was approved by the institutional review board of Osaka University Hospital (Ethical number: 17361) and was registered in 2017. We retrospectively reviewed 97 adults (age, ≧18 years) who underwent any type of LVAD implantation at our institution from June 2011 to June 2016. We extracted all the clinical information from their medical records.
In our management protocol of the nutrition after LVAD implantation, the target calorie intake is set at 25 kcal/predicted body weight/day as non-protein calorie (NPC), to be achieved within 1 week through parental nutrition (PN) and EN. One half of the target amount of calorie is planned to be received through EN. The patients can start taking meals after they are extubated without laryngeal paralysis. Our primary goal was the achievement of EN at POD14 after LVAD implantation. Individual nutrition plan was determined by the attending intensive care unit (ICU) physicians based on the protocol.
We calculated the calories for PN and EN on POD14 after LVAD implantation and divided the patients into two groups (group SEN (sufficient enteral nutrition) and group IEN (sufficient enteral nutrition)) based on EN calories: the EN calories for group SEN were >80% of their target calories or the EN calories of group IEN were <80% of their target calories. The EN calorie of a patient who was fed through a gastric tube was calculated from the administered calories. With regard to EN calories of patients taking meals, we applied the following approximation: Patients eating >80% of their meals were defined as group SEN. Their EN calorie intake was estimated as 80% of their target calories. Patients who ate <80% of their meals were defined as group IEN. Their EN calorie intake was estimated as 50% of their target calories.
We collected the following clinical information as baseline characteristics: age, weight, height, body mass index (BMI), underlying cardiomyopathy, and type of LVAD. Data within 7 days after surgery were also collected: 7-day mean doses of adrenaline, noradrenaline, and dobutamine; 7-day mean values of central venous pressure (CVP) and oxygen saturation of mixed venous blood (SvO2); number of days nitric oxide was administered; 7-day mean serum total bilirubin (T-Bil) level; occurrence of acute kidney injury (AKI) and re-operation; number of days opioids were administered; and the mean daily gastric residual volume. We collected data of the doses of adrenaline, noradrenaline, and dobutamine, and the values of CVP and SvO2 at 12 a.m. each day. If the pulmonary catheter was removed before 1 week, SvO2 data were obtained until the removal. AKI was defined based on the Kidney Disease: Improving Global Outcomes (KDIGO) (2012) criteria: increase in serum creatinine by >0.3 mg/dL within 48 h, increase in serum creatinine to >1.5 times baseline, or urine volume <0.5 mL/kg/h for 6 h. Ventilator-free days within 28 days after surgery and length of ICU stay were also compared.
Statistical analysis
Categorical and continuous variables were expressed as frequencies and percentages, and medians with interquartile range (IQR), respectively. In our univariate analysis, Fisher exact test was used to identify the associations between categorical variables, and Mann-Whitney U test was used for comparison between medians. In our multivariable analysis, logistic regression analysis was used. The mean values of CVP, SvO2, T-Bil, and occurrence of AKI within 7 days after surgery were included. We considered CVP and SvO2 as the indices of right and left heart functions, respectively. In addition, T-Bil and AKI were included for liver and kidney functions, respectively. We analyzed these four factors that were presumed to be associated with the initiation of EN at POD14 after LVAD implantation. Pearson correlation was used to measure the relationship between mean CVP during 1 week after LVAD implantation and percentages of EN feeding calories reaching the target calories on POD14.
A P value of <.05 was considered statistically significant. All statistical analyses were performed with statistical software EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan), which is a graphical user interface for R (The R Foundation for Statistical Computing, version 3.2.2). More precisely, it is a modified version of R commander (version 2.2-3), which is designed to add statistical functions frequently used in biostatistics.
Results
Overall, 97 patients were included in the analysis. The median age was 44 (36, 55) years, and the median BMI was 20.2 (18.1, 23.1) kg/m2 (Table 1). The most common indication for LVAD implantation was dilated cardiomyopathy (60 cases; 62%), followed by hypertrophic cardiomyopathy (15 cases; 16%). The most frequently implanted type of LVAD was HeartMate II (36 cases; 37%), followed by Duraheart (18 case; 19%) and EVAHEART (17 cases; 18%).
Baseline characteristics.

Quantitative data are expressed as median and interquartile range. Categorical data expressed as number and percentage.
Abbreviations: BW, body weight; BMI, body mass index; CM, cardiomyopathy; IEN, insufficient enteral nutrition; LVAD, left ventricular assisted device; SEN, sufficient enteral nutrition.
Of the 97 patients, 53 (54.6%) and 44 patients (45.4%) were classified into groups SEN and IEN, respectively (Table 2). The median total calorie intake on POD14 in groups SEN and IEN were 1313 (1141, 1510) kcal and 979 (737, 1199) kcal, respectively. The median accomplished percentages of the total calorie intake on POD14 in groups SEN and IEN were 80 (80, 92.7) % and 60.3 (49.0, 79.9) % of the target calories, respectively. The median EN feeding calories in groups SEN and IEN were 1229 (1103, 1411) kcal and 261 (0, 755) kcal, respectively. The median accomplished percentages of the EN calories on POD14 in groups SEN and IEN were considerably different [18.7 (0, 50) % in group IEN].
Comparison of EN and total calorie intake on POD14 between groups SEN and IEN.

Quantitative data are expressed as median and interquartile range. Categorical data are expressed as number and percentage.
Abbreviations: EN, enteral nutrition; IEN, insufficient enteral nutrition; SEN, sufficient enteral nutrition.
The 7-day mean dose of noradrenaline, 7-day mean value of CVP, number of days nitric oxide was administered, and mean daily residual gastric volume in group SEN were significantly lower than those in group IEN (P < .001) (Table 3). The 7-day mean dose of adrenaline in group SEN was also significantly lower than that in group IEN (P = .008). The 7-day mean SvO2, 7-day mean dose of dobutamine, 7-day mean serum T-Bil, occurrence of AKI, re-operation, and number of days opioid were administered were not significantly different. Ventilator-free days within 28 days after the surgery and length of ICU stay in group SEN were significantly shorter than those in group IEN.
Comparison of perioperative data during 1 week after LVAD implantation and outcomes between two groups.

Quantitative data are expressed as median and interquartile range. Categorical data are expressed as number and percentage.
Abbreviations: AKI, acute kidney injury; CVP, central venous pressure; ICU, intensive care unit; IEN, insufficient enteral nutrition; LVAD, left ventricular assist device; NO, nitric oxide; SEN, sufficient enteral nutrition; SvO2, oxygen saturation of mixed venous blood; T-Bil, total bilirubin.
In our multivariate analysis, increased CVP during 1 week after LVAD implantation was identified as an independent risk factor for delayed EN on POD14 (odds ratio [OR], 1.40; 95% confidence interval [CI], 1.11-1.66; P = .0032) (Table 4). T-Bil, AKI, and SvO2 were not significant predictors for administration of EN on POD14. The correlation coefficient between mean CVP and percentages of EN feeding calories reaching the target calories on POD14 was −0.247 (P = .0146) (Figure 1).
Multivariate analysis of the perioperative risk factors during 1 week after LVAD implantation related to delayed EN on POD14.

Abbreviations: AKI, acute kidney injury; CVP, central venous pressure; EN, enteral nutrition; LVAD, left ventricular assist device; SvO2, oxygen saturation of mixed venous blood; T-Bil, total bilirubin.
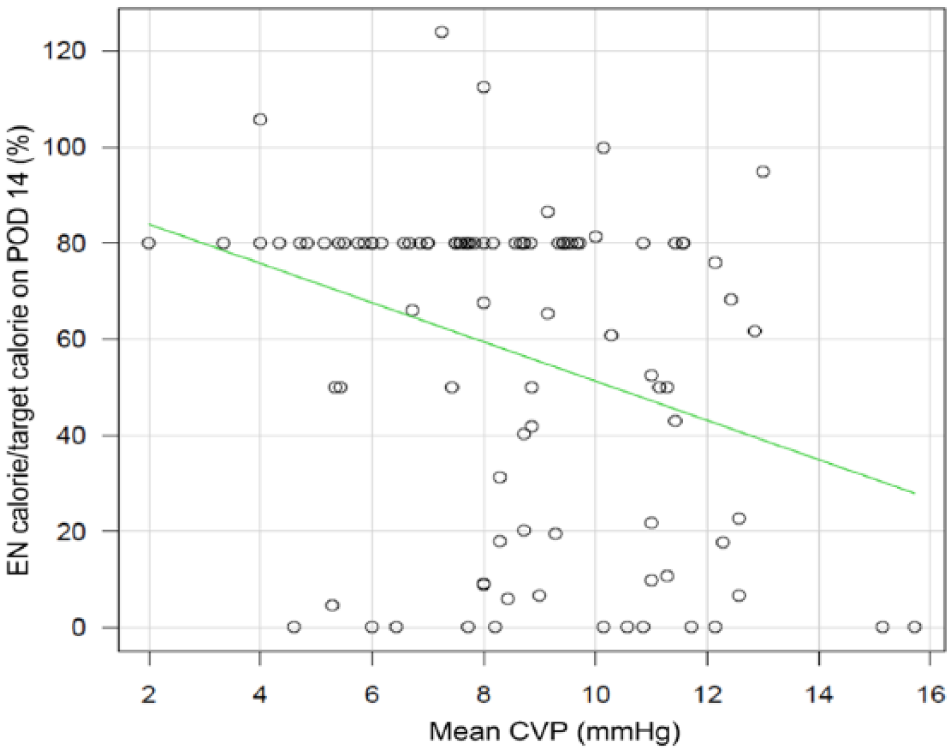
Relationship between mean CVP during 1 week after LVAD implantation and percentages of EN feeding calories achieved for the target calories on POD14. EN indicates enteral nutrition; CVP, central venous pressure; POD, post-operative day.
Discussion
In the present study, we demonstrated that high CVP during 1 week after LVAD implantation was an independent risk factor related to decreased EN calorie intake on POD14. In contrast, T-Bil, AKI, and SvO2 were not associated with the accomplishment of EN feeding. High CVP after LVAD implantation could be a sign for gastrointestinal intolerance. Identifying patients with gastrointestinal intolerance may help reduce complications of EN.
The initiation of EN is reported to be possible in patients with severe hemodynamic failure.9,10 In a large-scale, multi-center, observational study by Khalid et al, 11 mechanically ventilated, vasopressor-dependent patients have been shown to have a significant survival advantage when EN feeding was started within 48 h after ICU admission compared with those starting EN feeding later than 48 h. The initiation of EN feeding after LVAD implantation has not been studied. To the best of our knowledge, our study is the first report showing the impact of high CVP on EN feeding in patients undergoing LVAD implantation.
Increased intestinal work through EN leads to increased splanchnic blood flow. 12 The initiation of EN in patients with cardiac shock is controversial because low blood flow in the splanchnic area can cause intestinal ischemia. 13 Although the occurrence of intestinal ischemia is rare, 14 knowing whether hemodynamic response to EN is adequate in patients who are hemodynamically unstable is difficult. In this study, because SvO2 levels were not low in all patients, their cardiac output was speculated to be adequate without symptoms of left ventricular failure. In patients with LVAD implantation, because cardiac output is speculated to be preserved, remarkable intestinal ischemia basically does not usually occur.
However, most of the patients required inotropes and NO inhalation to prevent RV failure. High CVP is usually caused by RV dysfunction or fluid overload after LVAD implantation. During a prospective study on patients with chronic heart failure whose left ventricular ejection fraction ≦40%, Miroslava Valentova et al 8 found that congestive RV dysfunction may trigger cardiac cachexia. The results of our study showed that high CVP might reflect gastrointestinal edema, inducing gastrointestinal intolerance even when cardiac output is preserved after LVAD implantation. Careful observation and monitoring are necessary to evaluate gastrointestinal intolerance in patients with LVAD implantation.
The measurement of gastric residual volume is thought to be one of methods for detecting gastrointestinal intolerance. ESICM suggests delaying EN if the gastric residual volume is >500 mL/6 h, 7 but Montejo et al 15 reported that the limit of 500 mL for gastric residual volume is not associated with gastrointestinal complications from the analysis of 329 intubated patients. Deciding the clear threshold for gastric residual volume provided for EN in critically ill patients is difficult. In addition, because the stomach of patient with LVAD is displaced by the LVAD apparatus, the type and position of LVAD may affect the stomach size. Therefore, implanted LVAD may make the decision for the threshold of gastric residual volume more difficult.
RV dysfunction in patients with end-stage heart failure leads to liver dysfunction. 16 Tsiouris et al 17 showed that preoperative hepatic and RV dysfunction seem to be predictors of post-LVAD survival, which should certainly be taken into account in the patient selection process. Because early EN in acute liver failure is recommended based on the reports showing the improvement of outcomes, except for fulminant hepatic failure, EN may prevent hepatic damage caused by RV dysfunction.7,18,19 Therefore, we hypothesized that the high value of serum T-Bil within 7 days after surgery, which was presumed to be related to liver damage due to RV dysfunction, might be related to gastrointestinal intolerance. However, high serum T-Bil level within 7 days after LVAD implantation was not an independent risk factor for the delay of EN on POD14. High serum T-Bil level after LVAD implantation could not be induced only by liver damage due to RV dysfunction. Hemolysis, absence of food, drug-induced, or other causes of liver injury could increase serum T-Bil levels. Hemolysis is particularly the usual complication of cardiac surgery and LVAD support.20,21
LVAD implantation can frequently lead to AKI due to various causes, such as the following: neurohormonal activation; hemodynamic factors, such as low renal perfusion and venous congestion; hemolysis; drugs, including antibiotics; inflammation; and oxidative stress.22,23 No clinical trial has studied the relationship between AKI and gastrointestinal intolerance. AKI might induce gastrointestinal edema and electrolyte abnormality. We hypothesized that AKI would likely affect gastrointestinal intolerance, but it was not significantly related in the present study.
Gastrointestinal intolerance can lead to VAP. 24 Our analysis showed high CVP after LVAD implantation could be a sign for gastrointestinal intolerance. CVP may be a favorable marker regarding the administration of standard or decreased EN feeding. In case EN is used for such patients, we suggest that EN should be started very slowly or delayed until CVP decreases. With regard to how EN is used for patients with LVADs, more studies are required.
Our study has several limitations. First, this is a retrospective and observational small study in a single-center. Second, we set the target intake calories, but the attending physicians determined the actual amount of EN. Various factors, including vital signs, doses of catecholamine, and gastric residual volume, could affect their decision. We assessed the predictors within a week interrupting EN progression even on POD14; nevertheless, the attending physicians attempted to achieve the target calorie intake. Third, emergent surgery for various complications after LVAD implantation, including bleeding, cardiac tamponade, and cerebral hemorrhage could suddenly reduce the amount of EN despite receiving adequate EN before the surgery. Further high-quality investigation will be required to clarify the association between CVP and EN feeding in patients undergoing LVAD implantation.
Conclusions
EN might possibly improve the post-operative outcome after LVAD implantation, but this analysis showed that high CVP was an independent factor for reduced EN. Even when cardiac output is maintained, high CVP was a signal of gastrointestinal disorder. In case EN is used for patients with high CVP after LVAD implantation, we suggest that EN should be started slowly or delayed until CVP decreases.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Concept/design: Ryuichiro Abe, Akinori Uchiyama
Data collection: Ryuichiro Abe, Atsuhiro Matsumoto, Ryota Sakaguchi
Data analysis/interpretation: Ryuichiro Abe, Atsuhiro Matsumoto, Akinori Uchiyama
Drafting article: Ryuichiro Abe, Atsuhiro Matsumoto, Akinori Uchiyama, Yuji Fujino
Critical revision of article: Ryuichiro Abe, Atsuhiro Matsumoto, Ryota Sakaguchi, Akinori Uchiyama, Yuji Fujino
Approval of article: Ryuichiro Abe, Atsuhiro Matsumoto, Ryota Sakaguchi, Koichi Toda, Yoshiki Sawa, Akinori Uchiyama, Yuji Fujino.