
Abstract
Background:
Palliative care has been recognized as an essential component of a humanitarian response; however, it remains unavailable in most humanitarian crisis settings. Globally, healthcare workforce capacity represents a major barrier to implementing children’s palliative care, and there is limited evidence to guide educators on the learning needs and preferences of healthcare professionals working in humanitarian settings.
Objective:
The primary objective of this study was to explore the extent of training, experience, and confidence in children’s palliative care among healthcare professionals working in humanitarian settings. Secondary objectives were to identify perceived educational needs, including priority learning topics and preferred methods of palliative care education.
Methods:
We conducted a cross-sectional survey of healthcare professionals with experience working in humanitarian settings. The survey assessed participants’ self-reported knowledge, confidence, attitudes, prior training experiences, and learning preferences related to children’s palliative care.
Results:
One hundred thirty four healthcare professionals participated, including nurses (37%), physicians (17%), and clinical officers (15%). Most participants provided clinical care (n = 82, 64%) and were locally recruited staff (83%). More than 70% of respondents reported having some palliative care training, either during their professional training (n = 52) or through continuing medical education (n = 41). Despite this, many participants reported discomfort with key palliative care situations, including forming a therapeutic relationship with families of dying children (61%) and discussing impending death with parents (61%). Nearly all respondents (98%) expressed interest in further training, with preferred learning modalities including online teaching sessions and web-based certificate courses.
Conclusions:
There is strong interest and awareness for children’s palliative care training amongst humanitarian healthcare professionals. Despite prior exposure to palliative care education, many participants report limited confidence and skill in providing children’s palliative care, particularly in communication and psychosocial domains. Health educators should consider developing online training programs on children’s palliative care to meet the educational needs of healthcare professionals in humanitarian settings.
Keywords
Introduction
There is a growing recognition of the need for palliative care to prevent and relieve serious health-related suffering for children. Every year, an estimated 21 million children worldwide require access to palliative care, yet access remains extremely limited. 1 The 2020 Global Atlas of Palliative Care estimated that 97% of the children living with serious or life-threatening illnesses reside in low- and middle-income countries, where palliative care services are often scarce or inaccessible.2,3
In 2018, the World Health Organization published its first guidance on integrating palliative care into humanitarian responses, emphasizing an ethical responsibility to relieve physical, psychosocial, emotional, and spiritual suffering among individuals with serious and life-threatening illness. 4 Despite this, children’s palliative care needs during humanitarian crises remain particularly neglected. When palliative care activities are present, they are often focused on adults, particularly those with cancer. Globally, neonatal conditions, congenital anomalies, and neurological disorders account for the majority of pediatric palliative care need, while cancer represents less than 10%. 2 While children represent approximately 7% of the global need for palliative care, they may comprise a much larger proportion of those requiring palliative care in humanitarian settings, where populations are younger and child health services are often prioritized.2,4,5
Historically, global child health efforts have focused on communicable diseases, with limited attention to children with serious, chronic, or life-limiting conditions. Where palliative care services exist in low- and middle-income countries, they are often confined to urban tertiary facilities and poorly integrated into the country’s healthcare system. 6 In 2018, a Lancet Commission report on pain relief and palliative care recognized palliative care as “an essential component of any response to humanitarian emergencies and crises.” 7 Nevertheless, palliative care has remained largely overlooked in practice, with few published studies addressing palliative care delivery or training in humanitarian settings.7-11
Healthcare professionals working in humanitarian settings include physicians, nurses, clinical officers, and community health workers who often practice with expanded scopes of responsibility, limited access to specialist support, and significant resource constraints.12,13 Care is typically delivered at a local level and is primarily clinical in nature, frequently within rural or otherwise resource-limited healthcare facilities. 14 These professionals work across diverse humanitarian contexts, including camps for displaced populations (internally displaced persons or refugees), settings where populations lack access to routine healthcare services, and acute emergency responses related to armed conflict, natural disasters, or epidemics. Most humanitarian healthcare workers are locally recruited staff, with a smaller proportion of internationally mobile professionals supporting emergency responses.12-14
Building and training a skilled healthcare workforce capable of delivering palliative care is a key component of health system strengthening. Globally, limited palliative care knowledge and skills among healthcare professionals remain significant barriers to improving palliative care service availability.15,16 Training in pain and symptom management, psychosocial support, and end-of-life communication is often absent from undergraduate professional education, leaving clinicians underprepared to meet the needs of patients with serious illness. A recent survey of physicians providing cancer care in Bangladesh found that most physicians were unaware of the potential therapeutic benefits of morphine for pain management and did not feel adequately trained to prescribe morphine for this indication. 17 Emerging qualitative research from humanitarian contexts similarly identifies unmet education needs in pediatric palliative care, particularly related to communication, pain and symptom management, and addressing common misconceptions. 18 Beyond these studies, there remains little evidence to guide palliative care education for healthcare professionals working in humanitarian settings.
Understanding healthcare professionals’ knowledge, attitudes, and confidence regarding children’s palliative care is therefore essential to inform effective educational interventions. The educational needs of professionals in humanitarian settings may be distinct from those in other contexts, given differences in disease burden, resource availability, and healthcare delivery models. Constraints related to medications, equipment, staffing, and clinical infrastructure are likely to influence how palliative care interventions are delivered, underscoring the importance of context-specific training approaches.12,13
The aim of this study is to explore the educational needs of healthcare professionals in humanitarian settings, specifically exploring their knowledge, confidence, and attitudes toward children’s palliative care. A secondary aim is to explore the learning preferences of these health care professionals for training in children’s palliative care. These findings will support health system planners and educators in developing effective children’s palliative care training programs to effectively support capacity building amongst humanitarian healthcare professionals.
Methods
Sampling and Recruitment
A convenience sampling strategy was used to recruit participants. Potential participants were invited to participate via email and social media messaging. Participants were recruited through humanitarian health organizations and humanitarian health provider education networks, leveraging existing collaborations and contacts of study team members (MD, KR, RY) who had worked and provided palliative care training in humanitarian settings. Study recruitment used a snowballing technique. Additional recruitment was conducted via social media announcements with relevant professional societies, chat groups, and via word of mouth. No a priori sample size calculation or power analysis was conducted; the sample size was based on the number of participants who responded during the recruitment period.
Healthcare professionals were eligible to participate if they had a minimum of 2 months experience working in a humanitarian setting. The minimum 2 month threshold of humanitarian experience was selected to ensure that participants had sufficient exposure to the clinical and organizational realities of humanitarian healthcare delivery. A humanitarian setting was defined as an event (eg, armed conflict, natural disaster, epidemic, famine) or series of events that results in a critical threat to the health, safety, security, and well-being of a community or other large group of people. 19 Individuals were excluded if they had less than 2 months of experience working in humanitarian health settings. Participants were recruited between January and November 2023.
Study Design
This study was designed as a cross-sectional survey. Potential participants were invited to complete a one-time survey exploring their knowledge, confidence, attitudes, and educational needs and preferences related to children’s palliative care. Participants were asked to provide demographic information about their professional role, work experience, work location, and opioid availability. Participants’ self-reported knowledge, attitudes, and confidence providing palliative care were assessed using a seven-point Likert Scale from [1] “strongly disagree” to [7] “strongly agree.” Participants were asked about perceived palliative care needs among their patients, any prior palliative care training, and their learning needs and preferences.
Survey Development
There were no specific scales identified which had been published or adapted to humanitarian settings for palliative care knowledge, skills, or attitudes assessment. The study team developed a novel survey based on existing tools from well-resourced settings including the End-of-Life Professional Caregiver Survey, Palliative Care Quiz for Nursing, Neonatal Palliative Attitudes Scale, and Frommelt Attitude toward Care and Dying.20-23 These scales were designed for high income settings. The tool was reviewed and refined by palliative care clinicians with experience working in humanitarian settings, which led to modification of survey items to reflect the clinical practice in these settings. A humanitarian setting was defined for participants prior to survey completion. The study tool was pilot-tested with 4 humanitarian healthcare professionals (4/138, 3%) and modifications were made to the language to improve clarity and readability of questions and response items. A copy of the survey is included in Data Supplement 1.
Data Analysis
Demographic information was summarized using descriptive statistics. Results of Likert-scale data were summarized using frequencies. Responses of “strongly agree,” “agree,” and “somewhat agree” were considered positive, while responses of “strongly disagree,” “disagree,” and “somewhat disagree” were considered negative. Mean scores and standard deviations were calculated for each Likert statement. Preferred palliative care training modalities were ranked 1 to 3 by respondents and analyzed using a weighted-rank score. The most preferred training modality (selected first) would receive a score of 3, while the third most preferred training modality (selected third) would receive a score of 1. The total scores were added together and summarized utilizing a bar graph.
Ethics and Reporting
This research was conducted in accordance with the World Medical Association Declaration of Helsinki. Ethical approval for the study was obtained from the Research Ethics Board of the Children’s Hospital of Eastern Ontario (Approval Number: 22/90X; Date: July 26, 2022). All participants provided informed consent prior to participation, and all participant data were fully de-identified prior to analysis. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 24 The completed STROBE checklist is included in Data Supplement 2.
Results
Participant Demographics
134 healthcare professionals participated in the study, including nurses (37%), clinical officers (21%), and physicians (13%). The average age of study participants was 36 and most were men (63%). Participants had an average of 7.2 years of experience working in humanitarian settings and an average of 10 years of professional experience. Most participants’ work was primarily clinical care (64%), while a minority focused on health administration (13%). Most participants were working in a hospital (62%) or primary health centers (22%). Most participants were locally recruited staff (83%). Table 1 shows additional demographic data about participants.
Participant Demographics.

Multiple response options permitted.
Palliative Care Training and Experience
Most respondents (71%) had previous palliative care training, including formal teaching (39%) or clinical exposure (25%) during health professional training. Other types of training included online palliative care training (35%) and other types of continuing professional education (31%).
Strong opioids were reported as available by most participants (62%), although many reported that access was intermittent (46%). The most common strong opioid reported to be available was morphine (n = 85, 64%) followed by fentanyl (n = 20, 15%). Reported barriers to opioid availability included policy, legal, and financial barriers (28%) or opioids being out of stock (23%). Table 2 summarizes healthcare professionals’ previous palliative care experiences.
Participants’ Prior Training and Experience with Palliative Care.
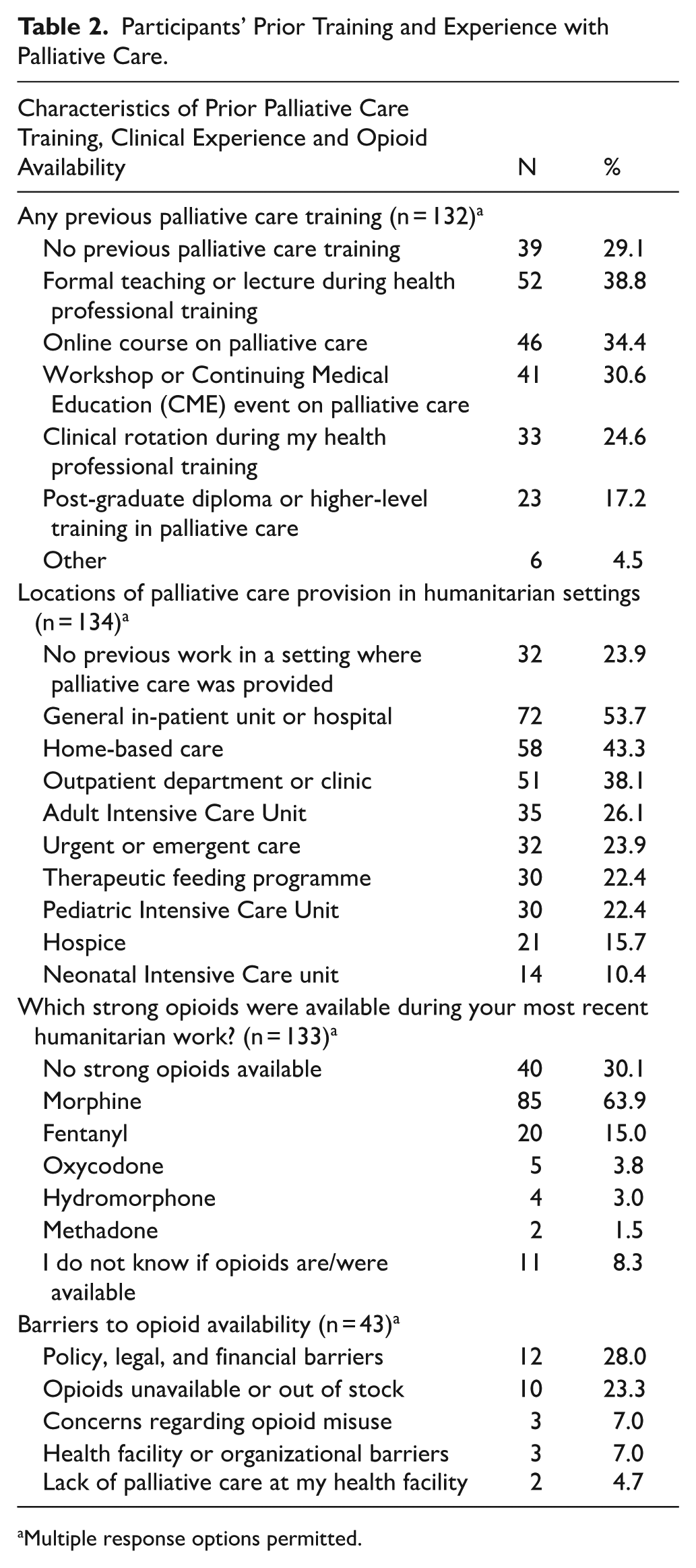
Multiple response options permitted.
Palliative Care Attitudes and Self-Efficacy
Table 3 summarizes healthcare professionals’ knowledge, attitudes, and self-efficacy related to children’s palliative care. Overall, respondents demonstrated strong knowledge and positive attitudes toward core palliative care principles. Most participants correctly endorsed early integration of palliative care at diagnosis (99%), the importance of palliative care in humanitarian contexts (97%), family-centered decision-making (94%), and the safe and effective use of morphine for pain control when prescribed by trained providers (91%).
Healthcare Professionals’ Knowledge, Attitudes, and Self-Efficacy Toward Children’s Palliative Care (n = 132-134, for Each Individual Question).

Participants’ responses were assessed using a seven-point Likert Scale (1 = strongly disagree; 7 = strongly agree). Responses of “strongly agree,” “agree,” and “somewhat agree” were categorized as agree, while responses of “strongly disagree,” “disagree,” and “somewhat disagree” were categorized as disagree. Mean scores and standard deviations (SD) were calculated for each statement.
While most respondents reported frequent exposure to death in humanitarian settings (78%), fewer indicated consistent access to mental health or counseling support (77%), sufficient time to spend with families following a child’s death (74%), or the availability of local policies and guidelines to support palliative care practice (72%). Many participants described caring for dying children as traumatic (64.7%) and reported feelings of personal failure when a child died (67%), highlighting the psychological burden of pediatric end-of-life care in humanitarian contexts.
Despite strong endorsement of honest communication as a principle (93%), communication-related challenges were common. Most respondents (70%) reported that they would change the subject to something cheerful when a child asked, “Am I dying,” and a majority reported discomfort discussing impending death with parents (61%) and difficulty forming therapeutic relationships with families of dying children (61%). Participants reported high self-efficacy for several clinical tasks, including identifying children who may benefit from palliative care (98%), assessing holistic needs (97%), and managing pain (93%).
Palliative Care Priorities
Nearly all (98%) participants were interested in further pediatric palliative care training. Preferred training topics included pain and symptom management (89%), communicating bad news (79%), and providing psychological and spiritual support (72%). Participants identified the need for additional supports and resources to be able to provide palliative care, including clinical training (68%), clinical guidelines and protocols (65%), and case studies (63%). Table 4 summarizes palliative care priorities and training preferences.
Palliative Care Priorities and Training Preferences.

Multiple response options permitted.
Preferred palliative care training modalities included online teaching sessions, web-based certificate courses, and in-person workshops. Learning modalities perceived as less effective included watching recorded videos, bedside teaching, and simulation. Figure 1 summarizes respondents’ preferred training modalities using a weighted-rank score.

Preferred palliative care training modalities. Values represent a weighted-rank score of healthcare professionals’ preferences, with higher values representing training modalities that are more preferred. Respondents were asked to select their top 3 preferred training modalities to help develop and improve their pediatric palliative care knowledge. For example, the most preferred training modality (selected first) would receive a score of 3, while the third most preferred training modality (selected third) would receive a score of 1. The total scores are shown in the Figure.
Discussion
This study describes the experiences, attitudes, confidence, and training preferences of healthcare professionals in humanitarian settings toward children’s palliative care. Most healthcare professionals were relatively well informed about core palliative care concepts and had received some palliative care training during their professional training or through continuing professional education online courses; however, comfort and confidence with important aspects of palliative care communication were low. Most participants were very interested in further palliative care training, identifying online sessions as their preferred modality.
Providing training in humanitarian settings may be challenging, and in-person training can be particularly difficult due to the security context, remote location, cost, and availability of trainers.12,25,26 Online training suggests an innovative strategy to overcome some of these barriers.27,28 Project ECHO is one example of an online training and mentorship model identified in the literature to build healthcare workforce capacity in palliative care. Several authors of this manuscript have experience implementing Project ECHO-based programs in pediatric palliative care, with a number of studies describing the use of Project ECHO for children’s palliative care in South Asia and Africa.27,29,30 The present study identified that humanitarian healthcare professionals are receptive to online training, which suggests that humanitarian health organizations consider how best to use online training to effectively deliver basic palliative care training, which can be complemented with practical clinical exposure and mentorship to consolidate skill development.
Most healthcare professionals in the present study were aware of core palliative care principles, including the importance of starting palliative care early in the course of a serious illness, the importance of pain relief, and that morphine is safe when prescribed by trained providers. These results may reflect study respondents’ previous training in palliative care. However, despite a strong understanding of core palliative care principles, many participants agreed with common misconceptions related to delivering palliative care. For example, despite correctly identifying that dying persons should be given honest answers about their condition, most survey respondents agreed that it is best to change the subject to a cheerful one if they are asked by a child “Am I dying?.” This suggests that healthcare professionals may struggle to translate their palliative care knowledge into clinical practice. The contradiction between theoretical understanding and practical implementation highlights the need for simulation, clinical exposure, and mentorship to support clinical practice change. The importance of practical training should be considered in the design and delivery of children’s palliative care education programs for humanitarian healthcare professionals.
Humanitarian emergency responses are high stress environments where healthcare professionals are frequently exposed to serious injuries, suffering, and death. 31 Many study participants felt that it was traumatic to care for dying children and noted that the death of a child leads to a sense of personal failure. Providing training and support can ensure that healthcare professionals receive sufficient support to effectively address the psychological impacts of their work. Incorporating training on how to cope with exposure to trauma and suffering are important to consider when developing palliative care training in humanitarian settings.
Despite morphine being an essential medication for relieving moderate to severe pain, access to morphine and other opioids remains a significant challenge in many settings. Ensuring opioid availability and accessibility are important considerations in humanitarian settings, as opioid supplies when available are frequently interrupted. 32
This is the first study to specifically examine the attitudes and educational needs among healthcare professionals providing children’s palliative care in humanitarian settings. The study included participants from a wide variety of countries and included humanitarian healthcare professionals from varied clinical settings and levels of experience. This supports the study findings’ relevance for educators designing palliative care training tailored to the diverse global contexts where humanitarian crises occur and training should be contextualized to the setting.
This study has several limitations. Participants were recruited using a purposive, convenience sampling strategy through humanitarian health organizations and professional networks. This may have preferentially captured individuals with prior palliative care experience and prevented accurate determination of the total number invited or an overall response rate. The absence of a formal sample size or power calculation and the relatively small sample limited subgroup analyses, which may limit the generalizability of study findings. In addition, the survey was administered in English only, which may reduce applicability to non-English speaking humanitarian healthcare workers. Finally, the quantitative design did not allow participants to elaborate on contextual barriers or challenges in delivering pediatric palliative care. Future studies incorporating qualitative methods would provide a more nuanced understanding of training needs and experiences.
Conclusions
Most healthcare professionals in this study were relatively well informed about core principles of children’s palliative care and had received some palliative care training during their professional education or through continuing professional development. However, confidence and comfort with key aspects of palliative care delivery, particularly communication with children and families and psychosocial support, were limited. Nearly all participants expressed strong interest in further training, with a preference for online educational modalities. These findings suggest a need for context-specific, skills-based, and communication-focused children’s palliative care training programs to support healthcare professionals working in humanitarian settings.
Supplemental Material
sj-docx-1-his-10.1177_11786329261445187 – Supplemental material for Children’s Palliative Care Knowledge, Attitudes, and Learning Preferences Among Healthcare Professionals Working in Humanitarian Crisis and Emergency Settings
Supplemental material, sj-docx-1-his-10.1177_11786329261445187 for Children’s Palliative Care Knowledge, Attitudes, and Learning Preferences Among Healthcare Professionals Working in Humanitarian Crisis and Emergency Settings by Zachary Blatman, Spandana Rayala, Kathryn Richardson, Mohammed Ilias Kamal Risat, Rachel Yantzi and Megan Doherty in Health Services Insights
Supplemental Material
sj-docx-2-his-10.1177_11786329261445187 – Supplemental material for Children’s Palliative Care Knowledge, Attitudes, and Learning Preferences Among Healthcare Professionals Working in Humanitarian Crisis and Emergency Settings
Supplemental material, sj-docx-2-his-10.1177_11786329261445187 for Children’s Palliative Care Knowledge, Attitudes, and Learning Preferences Among Healthcare Professionals Working in Humanitarian Crisis and Emergency Settings by Zachary Blatman, Spandana Rayala, Kathryn Richardson, Mohammed Ilias Kamal Risat, Rachel Yantzi and Megan Doherty in Health Services Insights
Footnotes
Acknowledgements
None.
Ethical Considerations
This research was conducted in accordance with the World Medical Association Declaration of Helsinki. Ethical approval for the study was received from the research ethics board of the Children’s Hospital of Eastern Ontario (Approval Number: 22/90X; Date: July 26, 2022).
Consent to Participate
Written informed consent was obtained from participants prior to participation.
Consent for Publication
Not applicable.
Author Contributions
Z.B., S.R., and M.D. contributed to project conception, study design, data analysis and interpretation, and manuscript drafting. K.R. and R.Y. contributed to study design and data analysis and interpretation. MIKR. contributed to study design and data acquisition, analysis, and interpretation. All authors contributed to critical revision of the manuscript for important intellectual content and approved the final version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Available upon request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.